
Abstract
Brown-Séquard syndrome (BSS) has many etiologies, including penetrating trauma, extramedullary tumors, and disc herniation. However, thoracic ossification of the ligamentum flavum (OLF) is an extremely rare cause of this syndrome. A 46-year-old woman with motor weakness in her right lower extremity and urinary retention was admitted to our department. Based on the results of physical examination, computed tomography, and magnetic resonance imaging, a diagnosis of BSS with OLF was considered. The patient underwent urgent conservative treatment. BSS is a rare condition characterized by hemisection or hemicompression of the spinal marrow. The herein-described case of incomplete BSS due to OLF responded to conservative treatment. However, the successful nonoperative management of this case is insufficient evidence to consider it as the standard of care. Therefore, emergency laminectomy decompression remains the standard of care for BSS.
Keywords
Introduction
Brown-Séquard syndrome (BSS) is a type of incomplete spinal cord injury that was first described by Dr. Charles-Édouard Brown-Séquard in 1849. 1 The clinical manifestations of BSS are loss of ipsilateral motor function, decreased proprioception, and loss of contralateral pain and temperature sensation. 2 BSS is usually caused by hemisection or hemicompression of the spinal marrow. The syndrome is mostly seen in patients with penetrating trauma and extramedullary tumors.3,4 Thoracic ossification of the ligamentum flavum (OLF) is an exceptionally rare cause of BSS.
OLF is a type of pathological heterotopic ossification of the spinal ligaments. Polgar first reported the lateral radiographic findings of OLF in the thoracic spine in 1920. 5 Currently, biomechanical alterations are considered an important hypothesis for the development of OLF.6,7 The most frequent site of OLF is the thoracic level of the spine, 8 and it often presents as slowly progressive thoracic myelopathy and occasionally as posterior cord syndrome. 9 However, BSS caused by thoracic spinal stenosis due to OLF has rarely been reported. We herein describe a patient with asymptomatic OLF who developed BSS after minor trauma.
Case presentation
A previously healthy 46-year-old woman with motor weakness in her right lower extremity and urinary retention was admitted to Central Hospital Affiliated to Shenyang Medical College because of a sudden fall caused by a bicycle accident 1 day previously. Physical examination revealed Medical Research Council grade 3/5 motor weakness of her right lower limb. Neurologic examination revealed obviously decreased proprioception below the right T11/12 dermatome. Reduced sensation of pain and temperature in her left lower extremity was also noted. She exhibited slightly hyperactive deep tendon reflexes of her right lower extremity but bilateral negativity for Babinski’s reflex. These physical examination findings indicated a diagnosis of BSS.
Magnetic resonance imaging of the thoracic spine showed a large intracanal occupation at the T9 level, especially in the sagittal image (Figure 1(a)). Computed tomography showed evidence of classic OLF under the right T9/10 lamina (Figure 1(b)–(d)).

Magnetic resonance imaging scans (T2-weighted) of the spine in the (a) sagittal and (c) axial views revealed significant intracanal occupation and compression of the spinal cord at the T9/10 level (red arrow). Computed tomography scans in the (b) sagittal and (d) axial views showed remarkable ossification of the ligamentum flavum at the T9/10 level (red arrow).
The patient underwent conservative treatment with high-dose hormonal shock therapy (methylprednisolone at 30 mg/kg for 15 minutes followed by maintenance at 5.4 mg/kg/hour for the next 23 hours) and mannitol for detumescence.10,11 A neurological examination was performed daily to monitor for potential deterioration. After 3 days, the patient’s clinical symptoms, including her bladder sphincter control, had markedly improved. The catheter was removed 8 days later, at which time the muscle strength of her legs had improved to grade 4/5 and her bilateral sensory disturbance had improved. Fifteen days later, the patient was discharged and her physical condition had basically recovered.
Discussion
OLF, frequently described in Eastern Asian populations, is a neurological disease characterized by chronic growth and replacement of the ligamentum flavum with completely ossified bone. 12 According to the evolution of the ligament ossification, OLF can be classified into five types: the lateral type, extended type, hypertrophic type, fusion type, and tuberous type. 13 Progression of ossification may lead to compression of the lateral corticospinal tract, resulting in spastic paraplegia, as well as compression of the lateral spinal thalamus, resulting in loss of sensation. In particular, as seen in this case, BSS can be induced by occasional external forces based on the pathologic changes of OLF. To our knowledge, this is one of the few reported cases of thoracic OLF with BSS to date.
We reviewed cases of BSS caused by thoracic vertebral pathologies and their treatments reported from 1978 to 202114–44 (Table 1). Among these 50 cases, the age at presentation ranged from 11 to 76 years (average, 45.9 years). Several interesting etiologies were found. Thoracic spinal cord herniation was the most common cause of BSS, occurring in 25 cases (Table 2). In particular, Baldvinsdóttir et al. 45 reported that compression of the thoracic spinal cord with a cavernous hemangioma contributed to the development of BSS. Humaira et al. 2 presented a case of delayed-onset BSS resulting from an acquired spinal arteriovenous fistula. Several other conditions less commonly contributed to the initiation of BSS, including thoracic endovascular aortic repair, spinal intramedullary cysticercosis, solitary thoracic osteochondroma, demyelinating lesion, and intramedullary meningeal melanocytoma.46–51 In the current case, however, the development of BSS secondary to OLF was very unusual. To the best of our knowledge, only one other case of BSS secondary to OLF has been reported; this case occurred in the cervical spine in 2007. 12 No reports have described BSS secondary to OLF in the thoracic vertebrae. Although various subetiologies of BSS have been reported, BSS was ultimately caused by spinal stenosis or spinal cord injury among the previously reported cases. Therefore, when we encounter spinal stenosis and spinal cord injury in the clinical setting, we should take BSS into account.
Previously reported cases of Brown-Séquard syndrome at the thoracic spine.

Statistics and outcomes of surgical and conservative treatment of Brown-Séquard syndrome.
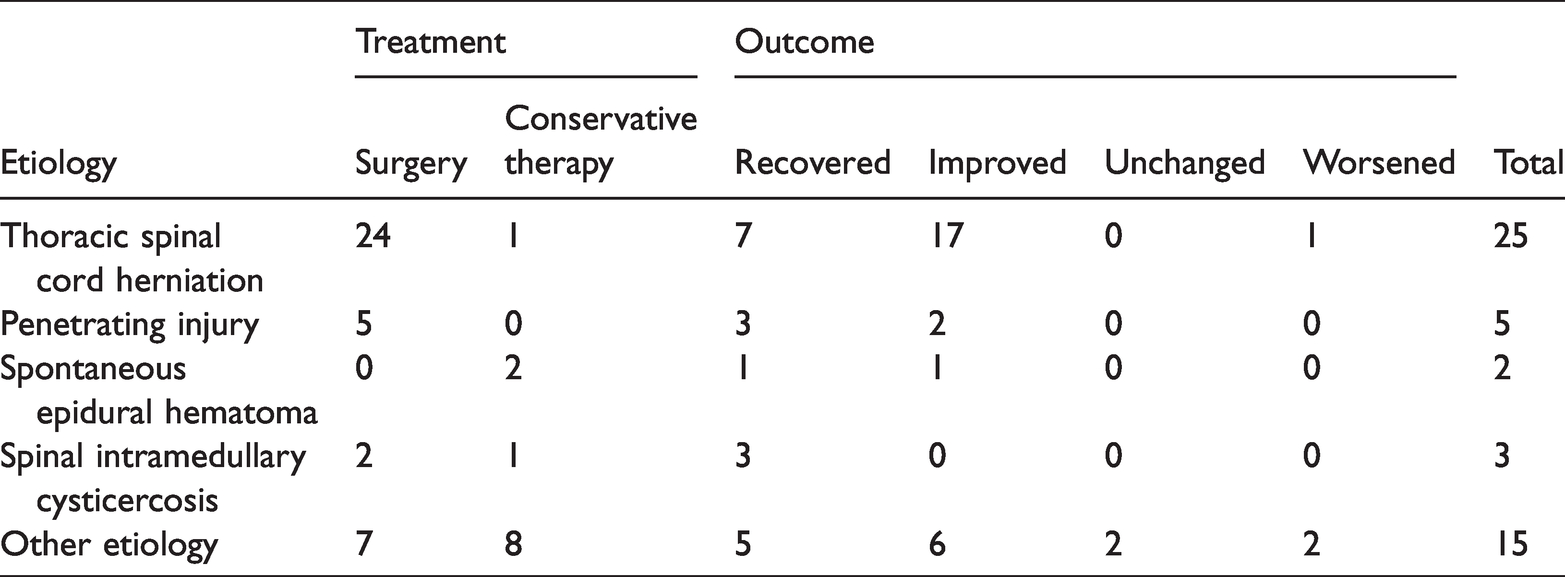
Among the 50 cases reported to date, posterior laminectomy or laminoplasty was performed with good results in 24 cases of spinal cord herniation and 5 cases of penetrating injury. Only one patient with spinal cord herniation was treated conservatively, and this patient’s status deteriorated after subsequent surgical treatment. 52 Two patients with an epidural hematoma were treated conservatively; one improved and the other recovered.53,54 Good results were obtained in three cases of BSS caused by intramedullary cysticercosis managed with different treatments (surgery in two cases and conservative treatment in one).47,48,55 Among the other 15 cases with rare etiopathogeneses, mixtures of conservative and surgical treatments were administered; 2 patients’ conditions deteriorated, 1 did not change, and the remaining improved or recovered. These cases indicate that prompt surgical decompression is a better choice for patients with BSS, and definite outcomes were achieved among these previous cases. However, the choice of treatment depends on the cause and severity of the disease. For example, conservative treatment is helpful for an epidural hematoma but may not be effective for spinal cord infarction.53,56
In the 46-year-old woman described in the present report, OLF was an uncommon cause of BSS. Although high-dose hormone therapy achieved remission in this case, the use of high-dose hormone therapy in early acute spinal cord injury remains controversial. The results of one meta-analysis may prompt arguments against the routine use of high-dose corticosteroids in acute spinal cord injury. 57 The meta-analysis also showed that the use of high-dose hormones may increase the risk of complications. However, considering the findings in the present case, we believe that decisions around high-dose hormone therapy should be based on the patient’s individual characteristics and left to the treating physician, who should balance potential benefits against potential complications. 57 Of course, caution is needed when administering large doses of hormones. Furthermore, after reviewing the reported cases of improvement or recovery with conservative treatment, we can infer that the prognosis may be favorable in patients with OLF presenting with incomplete neurological damage such as BSS. For patients with a stable and meliorative neurologic state, expectant treatment supervised by magnetic resonance imaging might eventually be a treatment choice once a much more complete understanding of the pathophysiology of this disease is achieved.
Conclusions
BSS is a rare condition characterized by hemisection or hemicompression of the spinal marrow. We have herein described a case of incomplete BSS due to OLF that responded to conservative treatment. However, the successful nonoperative management of this case is insufficient evidence to consider it as the standard of care. Therefore, emergency laminectomy decompression remains the standard of care for BSS.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221110069 - Supplemental material for Thoracic ossification of the ligamentum flavum causing Brown-Séquard syndrome: a case report and literature review
Supplemental material, sj-pdf-1-imr-10.1177_03000605221110069 for Thoracic ossification of the ligamentum flavum causing Brown-Séquard syndrome: a case report and literature review by Yeqiu Xu, Yuanzhuang Zhang, Yinzhou Luo, Guanzhen Qiu, Yize Liu, Wei Zhao and Yong Wang in Journal of International Medical Research
Footnotes
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
The reporting of this study conforms to the CARE guidelines. 58 This study was approved by the Institutional Review Board of Shenyang Medical College, and written informed consent for publication was obtained from the patient and his family. The corresponding author had full access to all the data and the final responsibility to submit for publication.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.