
Abstract
Background
COVID-19 has had a catastrophic effect on the healthcare system. Healthcare quality assessment measures the difference between expected and actual performances to identify gaps in the healthcare system. This study aimed to evaluate the quality of perinatal care for women with high-risk pregnancies (HPR) during the COVID-19 pandemic.
Materials and Methods
This cross-sectional study enrolled 450 women with HPR from health centers in Ahvaz, Iran, from December 2020 to May 2021, using a multi-stage sampling method. Quality of care was assessed using an observational checklist adapted from Ministry of Health guidelines. Data were analyzed using descriptive and statistical methods.
Results
The quality of the assessed aspect in comprehensive health centers and in peripartum, perinatal, and postpartum wards was moderate. The overall score for peripartum care was significantly positively correlated with the length of the retraining period, and the quality of perinatal care was significantly related to the proportion of elective cesarean sections and preterm delivery.
Conclusion
The development of care practices in health centers in Iran should focus on education and counseling. Practices in peripartum wards should emphasize the use of partographs, physical/mental support, and privacy for mothers, while perinatal wards should focus on timely counseling.
Introduction
High-risk pregnancies (HPR) are regarded as a major public health challenge, and addressing the healthcare needs of women with HPR is an aim of the World Health Organization (WHO) and Sustainable Development Goal 3. 1 HPR include any unanticipated medical or obstetrical issue related to pregnancy that presents an actual or potential risk to the health or well-being of the mother or fetus. 2 Approximately 20% of women experience HPR, 3 and WHO estimates that 50% of perinatal deaths occur in HPR. 4 In 2015, approximately 303,000 pregnant women died as a result of pregnancy complications, 5 with average mortality rates due to pregnancy complications in developing and developed countries of 200 and 20 per thousand live births, respectively. 6 Growing evidence suggests the existence of significant differences between maternal and infant mortality in developed and developing countries associated with differences in healthcare quality. 7 Achieving the required quality of care during pregnancy and childbirth is one of the most challenging aspects of the fifth Millennium Development Goal. 8 Quality of care (as defined by the American Medical Institute) is the degree of healthcare provided to individuals and communities that increases the likelihood of desired health outcomes and is consistent with current professional knowledge. 9 Maternal and infant mortality is considered as an indicator of healthcare quality, 10 and previous studies indicated that about 90% of deaths could be prevented by improving the quality of healthcare. 11 WHO also emphasizes the need for continuous monitoring and evaluation of health services to improve the quality of care. 12 One of the prerequisites for improving healthcare quality, especially in the field of maternal health, is the evaluation of different dimensions of care. 13 Measuring the quality of care not only determines how a program is delivered, in comparison with the standards, but also identifies the problem so that action can be taken to resolve it. 14
COVID-19 is an acute respiratory infection caused by a beta-coronavirus and was declared a pandemic by WHO on 11 March 2020. 15 Pregnant women were classified as a high-risk group and were advised to limit their social interactions to protect themselves against the virus. 16 Various countries also took new precautions to protect pregnant women, including only allowing asymptomatic partners in the delivery process or excluding supporting persons (doulas and partners) from maternity hospitals, the distribution of pregnant women and infants based on the epidemiological situation in different types of hospitals, telephone or video conferencing appointments, mask-wearing, and handwashing.17,18 However, emerging evidence indicates that services were impaired for many women, including suspended and/or canceled appointments, maternity-leave restrictions, continuous care, and ambiguities regarding partner attendance during childbirth. 19 According to Heaman et al., the quality of antenatal care is supported by constructs including information-sharing, preventive guidance, adequacy, accessibility, and availability, 20 which are likely to be disrupted during COVID-19 epidemics. 19 In addition, factors such as reassignment of midwives to general nursing duties, staff reductions due to COVID-19-related illness, the implementation of virtual rather than in-person appointments, 19 and restrictions on home births 21 and community visits, 22 could negatively affect the adequacy of services and the presence and availability of employees. These issues are of particular concern for maternity practices, because such restrictions can increase the adverse health consequences for both mother and baby. 23 Quality constructs for antenatal care thus require rapid adaptation to the COVID-19 pandemic. 19 For example, obstetric care staff have a responsibility to be aware of the availability of services and the impact of COVID-19 on pregnant women and their babies. 24 Javaid et al. showed the effect of COVID-19 on structural changes in the healthcare system and behavioral changes among pregnant women and their providers, redefining necessary and unnecessary procedures. 25
Given that the qualities of both prenatal and postnatal care can be directly affected by the COVID-19 pandemic, the main aim of this study was to evaluate the quality of perinatal care for women with HPR in Iran during the COVID-19 pandemic. The study also aimed to determine the relationships between the overall scores for care processes and predictor variables of service providers and maternal and neonatal health outcomes in perinatal and obstetric wards. The results may help to improve the quality of services and reduce maternal and infant mortality by improving our understanding of the current state of perinatal care and providing strategies to improve the quality of care.
Patients and Methods
This cross-sectional study collected information using a checklist and analyzed the data using descriptive and analytical statistics. This study was approved by the Ethics Committee of Shahroud University of Medical Sciences (confirmation ID: IR.SHMU.REC.1399.123). This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. 26 Participants were selected from 11 comprehensive health centers in the west and east of Iran and from three teaching hospitals affiliated with Ahvaz University of Medical Sciences, Khuzestan, Iran, from December 2020 to May 2021. The zone included four teaching hospitals affiliated with the University of Medical Sciences, one of which (Golestan Hospital) did not have a gynecology and obstetrics ward. Comprehensive health centers in this region were divided into west and east, with 22 and 17 comprehensive health centers, respectively.
Based on the study by Bajalan et al., 27 the sample size required to estimate the prevalence of cesarean delivery in HPR (as a measure of quality of prenatal care programs for women with HPR), with P = 0.550, d = 0.05 and α = 0.05, was calculated to be at least 379. Taking into account an estimated 15% non-participation/response rate, the required sample size was determined to be 436. Sampling was performed in several steps. Each comprehensive health center and educational hospital affiliated with Ahvaz University of Medical Sciences was considered as one level and the constituent units within each level were considered as clusters. The clusters in comprehensive health service centers consisted of urban health bases and health houses, and clusters in educational hospitals consisted of perinatal, delivery, and postpartum wards. The share of each cluster was then determined in proportion to the number of HPR in 2019 and samples were selected randomly from the clusters for each class. The sample size in each cluster was determined in proportion to the population covered by each base/health center and the number of referrals to each selected hospital in l2019. Among 200 individuals from comprehensive health centers, 85% (170 individuals) came from health centers in the west and 15% (30 individuals) from health centers in eastern Ahvaz. Among the 250 individuals from teaching hospitals affiliated with the university, 150 were from the perinatal ward and 100 from the delivery and postpartum wards. Sampling in each center was performed based on the following inclusion criteria using an easy and accessible method (Figure 1): women with HPR (any maternal and fetal risk status), gestational age greater than 22 weeks, and minimum literacy. The exclusion criteria were self-reported major psychiatric illness with a history of hospitalization and long-term treatment, current use of psychiatric drugs, and unwillingness to participate in the study.

Flowchart of study implementation.
The tools used in this study included the following four checklists: 1) participants’ personal and pregnancy information form; 2) care provider profile form; 3) checklist for care process by the service provider unit; and 4) outcome checklist.
Participants’ personal and pregnancy information form
The participants' personal and pregnancy information form consisted of 17 questions in two parts: personal information (7 questions) and pregnancy (10 questions). Personal information included age, level of education, occupation, income level, ethnicity, place of residence, and type of insurance. Pregnancy information included current pregnancy status (number of pregnancies, delivery, abortion, gestational age, starting time of care, body mass index, type of risk, risk in current pregnancy, place of care, pre-pregnancy care, whether or not pregnancy was wanted, time since previous pregnancy), past medical history (history of disease or surgery), history of high-risk behaviors (smoking, alcohol, imprisonment), and previous pregnancy status (previous HPR, history of preterm delivery, stillbirth, or neonatal death), and history of postpartum depression. The validity of this tool was determined by qualitative review, in which the researcher asked 10 faculty members specializing in maternal health and related research to present their views in writing after carefully studying the tool, and corrections were then made based on their opinions.
Care provider profile form
The care provider profile form consisted of 12 questions about age, work experience, degree, employment status, job position, job interest, retraining courses, history of communication and counseling skills courses, marital status, and pregnancy status. The validity of this instrument was determined by qualitative content review by five faculty members and five midwifery experts working in the health sector.
Checklist for care process by service provider unit
Each checklist item in the different sections was scored as “done” (2) “incompletely done” (1), or “not done” (0). If the item in question was not done, that item was not counted in the general calculation. The information obtained from this checklist was calculated compared with the desired level, with 0% to 33% indicating poor quality, 34% to 66% moderate quality, and 64% to 100% as good quality.
Outcome checklist
The outcome checklist was designed based on previous studies 32 evaluating quality-monitoring indicators of health-related obstetric care. The tool consisted of 19 indicators related to maternal and neonatal health outcomes. The indicators of neonatal outcomes included preterm delivery, low birth weight, macrosomia, shoulder dystocia, premature neonatal death, stillbirth, Apgar score less than 7 minutes in the first and fifth minute, and neonatal admission to the intensive care unit. Maternal outcomes included type of delivery, onset of labor, abnormal postpartum hemorrhage, placental abruption, grade 3 or 4 rupture, maternal admission to the intensive care unit, venous thrombosis, direct or indirect maternal death, and lactation problems. This checklist was validated by 10 faculty members of the university and finalized after applying their corrective comments.
In line with the code of ethics, the researcher presented a letter of introduction to the officials at each comprehensive health center and educational hospital in the care-provider unit and explained the objectives of the study, and was then allowed to evaluate the level of care. The service provider profile form was provided to the staff and they were asked to answer the questions honestly. Each morning, the researcher referred to one of the selected research environments and identified the qualified people. After obtaining written consent, they then completed the personal and midwifery profile form by interviewing the relevant personnel, and recorded their observations regarding caregiver performance and the relationship between caregivers and clients in the relevant checklist.
Statistical analysis
The obtained information was coded and analyzed using SPSS version 22 (IBM Corp., Armonk, NY, USA). The data were analyzed using descriptive statistical tests, including mean and standard deviation, as well as inferential χ2 and Fisher's exact tests, and Pearson’s correlation coefficient. P < 0.05 was considered to indicate a significant difference.
Ethical considerations
Written permission for the study was obtained from the ethics committee of Shahroud University of Medical Sciences, Shahroud, Iran (Approval ID: IR.SHMU.REC.1399.123). All participants were informed of the study methods and the benefits of the process, and all participants provided signed informed consent before beginning the study.
Results
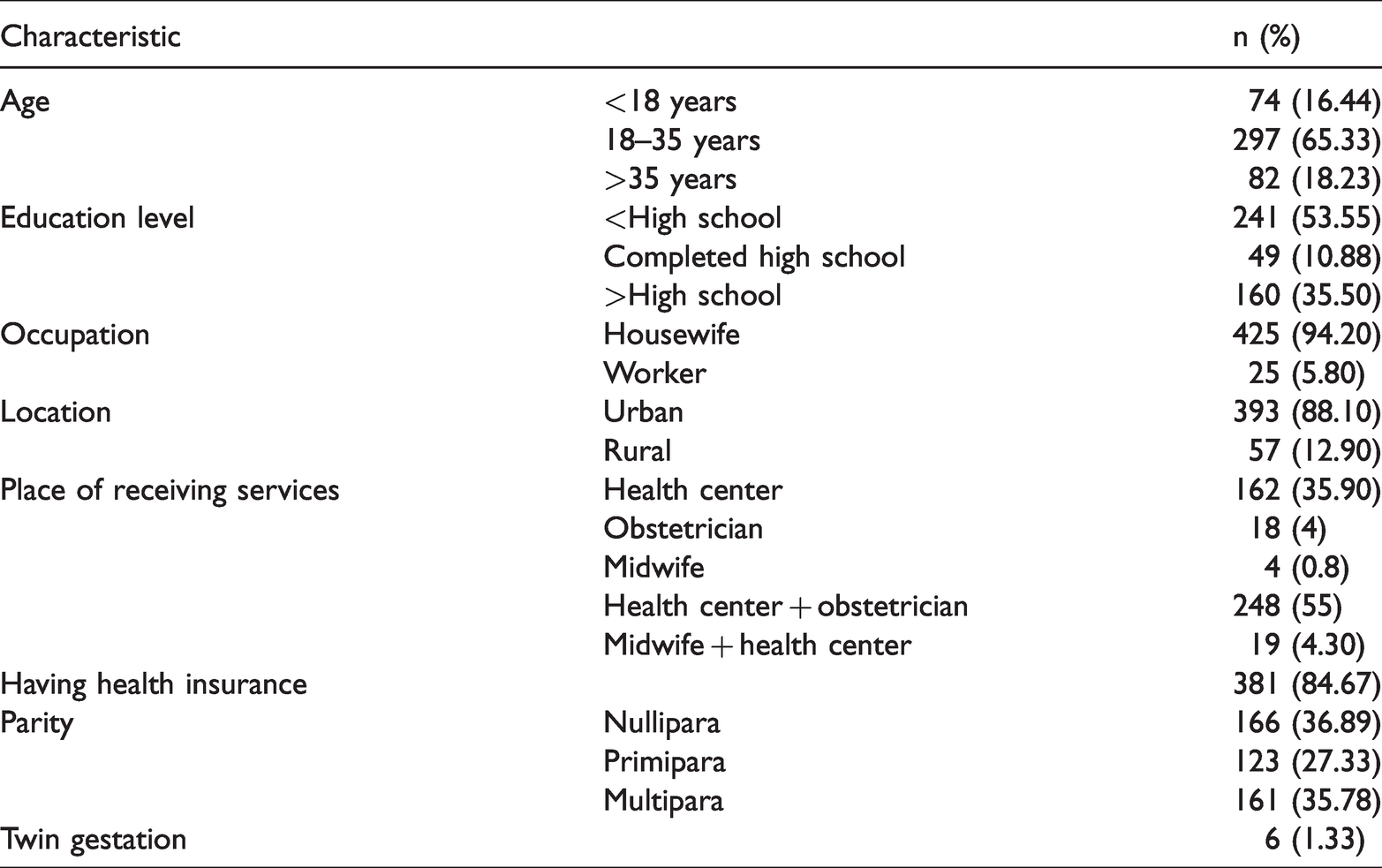
A total of 450 women with HPR from comprehensive health centers and different wards of selected hospitals were finally included in the study. The patients’ characteristics are given in Table 1. The mean gestational age was 30.17 ± 7.72 weeks, 20.88% had a history of HPR, and 7.70% had a history of preterm delivery, with a mean gestational age at their previous preterm delivery of 32.1 ± 2.08 weeks. Only 7.70% of patients had received preconception care and 96% had received prenatal care, with a mean gestational age at onset of prenatal care of 12.01 ± 6.70 weeks. The main pregnancy risk was preeclampsia (16.22%) followed by gestational diabetes (12.22%). Other risk factors with frequencies of less than 5% included twin pregnancy, fetal growth restriction, cardiac pacemaker, hydrocephalus, lupus, polyhydramnios, oligohydramnios, placenta accreta, impaired liver tests, rheumatoid arthritis, epilepsy, hepatic cholestasis, fetal heart hypoplasia, severe thrombocytopenia, vasoprevia, HIV-positivity, resistant pyelonephritis, cervical insufficiency, chronic hypothyroidism, type 1 diabetes mellitus, type 2 diabetes mellitus, asthma, COVID-19, high body mass index, third-trimester bleeding, premature rupture of the amniotic sac, preterm labor, and age under 18 years.
Individual characteristics of participants (n = 450).
In comprehensive health centers, counseling and clinical examination were considered to be of moderate quality in patients with gestational ages <30 weeks, 31 to 34 weeks, and 35 to 37 weeks, respectively. History taking was also moderate in 41.26% of cases at <30 weeks, 25.0% of cases at 31 to 34 weeks, and 38.46% of cases at 35 to 37 weeks (Table 2). The overall quality of peripartum care was moderate in 91% of cases, with a mean score of 235.93 ± 25.07 (possible range 0–394) (Table 3). The quality of care in the perinatal ward was moderate in 74% of cases, with a mean score of 29.18 ± 5.13 (possible range 0–48). The overall quality of postpartum care was moderate in 94% of cases, with a mean score of 51.72 ± 6.85 (possible range 0–92) (Table 4).
Frequency of care provided to women in health centers (n = 200).

Values reported as n (%).
aCommunication between care provider and client.
Frequency of peripartum care (n = 100).

Values reported as n (%).
aCommunication between care provider and client.
Frequency of perinatal and postpartum care.

Values reported as n (%).
aCommunication between care provider and client.
There was no significant correlation between the total perinatal and postpartum care scores and age, work experience, retraining hours, or communication skills course hours. However, the overall peripartum care score was significantly positively correlated with retraining course hours (r = 0.195, P = 0.047).
Table 5 shows the maternal–neonatal outcomes of the study participants. The mean gestational age at delivery was 37.88 ± 2.54 weeks. Based on Fisher's exact test, the quality of perinatal care was significantly related to the rates of elective cesarean section (χ2 = 7.50, P = 0.024) and preterm delivery (χ2 = 7.50, P = 0.023). Among individuals with good perinatal process scores, 11.11% experienced preterm delivery and 52.27% experienced planned cesarean section, compared with 33.33% and 33.33%, respectively, in individuals with moderate perinatal scores. Based on Fisher's exact test, the quality of peripartum care was not related to maternal–neonatal outcomes, including emergency cesarean section and preterm delivery. Among individuals with good scores for labor care, 0% underwent emergency cesarean section and 11.10% experienced preterm delivery, compared with 2.20% and 36.30%, respectively, among individuals with moderate postpartum care.
Maternal and fetal outcomes in women with high-risk pregnanciesa (n = 450).

aVenous thrombosis, fetal abnormalities, grade 3 and 4 perineal and vaginal rupture, and direct and indirect maternal death were not observed in the outcomes (frequency = 0 (0%)).
Discussion
This study aimed to evaluate the quality of perinatal care for women with HPR during the COVID-19 pandemic. The results showed that comprehensive health centers provided moderate to good care in terms of pregnancy trimester, and moderate levels of care in peripartum, perinatal, and postpartum wards of selected hospitals. To the best of our knowledge, this is the first study to evaluate the quality of perinatal care during the COVID-19 epidemic in Iran, and the results can thus be compared with the results of studies conducted at other times.
The quality of counseling, education, and clinical examination in comprehensive health centers was considered moderate, consistent with the findings of Esfandiariinejad et al. and Wilson et al. 33 However, Bahri et al. found that the health team showed poor performance in terms of training regarding the use of nutritional supplements. 34
History taking in the second and third trimesters was good in the current study, in line with the results of Bahri et al.’s study, 34 while Simbar et al. found that 48.71% of health personnel had a good performance in terms of history taking. 29
Partograph use during the first stage of labor was fairly good. A partograph provides a visual representation of the progress of labor, and can provide an accurate assessment of maternal and infant health and improve the quality of care when electronic fetal monitoring is not possible. 35 Palo et al. also reported low levels of use and completion of partographs. 36 The average level of emotional support and physical care in the first stage of labor was associated with poor scores for allowing movement during labor and giving information to the client, possibly due to a lack of understanding of women's autonomy in terms of self-care. Evidence-based information supports mobility in the first stage of labor in women without regional anesthesia 37 ; however, factors such as staff attitude and midwives' discomfort with delivery positions other than the lithotomy position may prevent its implementation. 38 At this stage, heart rate control was at the desired level, possibly due to the ease of use and availability of Sonicaid monitors. These results were consistent with the findings of Changaee et al. and Simbar et al.39,40 The quality of the Leopold maneuver, especially the first and second maneuvers, was good, in contrast to the findings of Changaee et al. 39 This apparent discrepancy may be attributed to the different environments in teaching hospitals (as in the present study), which may show greater observance of protocols and instructions compared with non-teaching hospitals. The score for checking vital signs (especially pulse) during the second stage of labor was poor, in accord with the findings of Changaee et al. 39 Emotional support and physical care in the second stage of labor (continuing care) were also unsatisfactory in 59% of cases. Continuous support from midwives during labor may reduce the duration of labor and the number of cesarean deliveries and should be available to all mothers. 41
Strong interpersonal communication skills and good interaction between healthcare providers and women are likely to increase women's satisfaction with the maternity care experience. 42 Poor scores for delivery readiness were due to a lack of scrubbing by the midwife and obstetrician and not respecting the mother's privacy at the time of delivery. WHO identified hand washing as one of the five key elements in patient safety, which is the foremost need in obstetrics. 43 Changaee et al. and Karimian et al. also showed unfavorable results for hand-washing in the second stage of labor.39,44 Lack of respect for the mothers' privacy is affected by a lack of education and empowerment of women, their low socioeconomic status, poor training of providers, and a lack of supervision and accountability. 45 However, the scores for placental detachment and neonatal evaluation in the third stage of care were good, indicating staff awareness of the importance of this care in improving maternal and infant health. These findings were consistent with the results of previous studies.40,44
Checking vital signs and providing emotional support and physical care of the mother during the fourth stage of labor were moderate, while controlling vital signs was important for controlling maternal health. Hypotension is a sign of postpartum hemorrhage (the leading cause of maternal death worldwide) that can be prevented by early diagnosis and treatment. 46 The quality of care in the perinatal department was poor in 26% of cases, mainly due to a lack of timely counseling, especially in terms of nutrition. Whitaker et al. also showed that nutritional counseling during pregnancy was limited and often failed to comply with protocols. 47 In this study, the quality of clinical examinations, counseling, and training in postpartum care (first 24 hours after delivery) was moderate, consistent with the results of Bahri et al. in Gorgan and Mirzaee et al. in Mashhad.34,48
In this study, there was no significant correlation between the overall score for the care process and the age of the service provider. Similarly, Aliakbari et al. found no significant correlation between nurses' performance scores for providing care in critical situations at different stages and ages. 49 In this study, there was a significant positive correlation between the overall score for care during delivery and the number of hours of retraining, while Ghaffari et al. found no significant relationship between participation in retraining and quality of performance. 11
In this study, 84% of women with HPR had health insurance (social security, health services), which allowed easy access to services (clinical and preclinical tests and screenings) provided to mothers free of charge or with low subsidies in health centers in Iran. However, increasing the volume of cases in these centers may present a challenge to the quality of the services.
In this study, the quality of peripartum care was not related to maternal–neonatal outcomes, including emergency cesarean section and preterm delivery, possibly due to the small sample size. However, previous clinical trials that controlled for confounding variables showed the effect of improved care during labor and delivery (especially continuous support and psychological support of the mother by a trained person) in reducing the rate of cesarean delivery and instrumental delivery, increasing the Apgar score, and in earlier start of breastfeeding. 50 This study described the current situation and had no control over how services were provided. However, the effect of perinatal risk status on the consequences of pregnancy and childbirth cannot be ignored.
One strength of this study was the comprehensive evaluation of the quality of care using tools taken from the guidelines of the Ministry of Health in women with HPR who need special care to reduce pregnancy complications, during the period of COVID-19. However, the study was limited by the cross-sectional nature of the research and by the lack of adjustment for time trends and lack of follow-up.
Conclusion
Developments in maternity care practices in health centers should focus on education and counseling, while the use of partographs, physical and mental support, and client privacy in peripartum wards, and timely counseling in perinatal wards also need to be improved.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221106723 - Supplemental material for Quality of perinatal care for women with high-risk pregnancies during the COVID-19 pandemic in Iran
Supplemental material, sj-pdf-1-imr-10.1177_03000605221106723 for Quality of perinatal care for women with high-risk pregnancies during the COVID-19 pandemic in Iran by Solmaz Mohammadi, Kobra Shojaei, Elham Maraghi and Zahra Motaghi in Journal of International Medical Research
Footnotes
Acknowledgements
We would like to thank all the women who participated in this study for sharing their views.
Conflict of interest
None declared.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Shahroud University of Medical Sciences (code: 860).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.