
Abstract
Contiguous spinal metastasis poses a challenge for spine surgeons. In patients with a short remaining life expectancy, surgery may be discouraged. However, in select cases, surgery may be inevitable to eliminate pain and improve the patient’s quality of life. Additionally, with advancements in systemic cancer therapy, the efficacy and duration of tumor control have improved significantly. Consequently, a patient’s life expectancy may be difficult to estimate with existing prognostic scores. Because patients may achieve prolonged survival, spinal metastasis surgery could greatly benefit a patient’s quality of life. In this report, we present the details of two patients with non-small lung cancer with contiguous spinal metastasis who underwent spinal surgery for their metastatic disease. After surgery and targeted therapy with epidermal growth factor tyrosine kinase inhibitors (EGFR TKI), the patients attained substantial healing of their previously lytic spines and achieved prolonged survival of up to 42 months. With modern systemic therapy for lung cancer, the treatment of spinal metastatic disease can achieve decent outcomes, even in poor surgical candidates.
Mini-abstract
In this report, we present two cases of contiguous spinal metastatic disease in non-small cell lung cancer patients who achieved prolonged survival and stable spinal fixation after treatment with EGFR TKIs.
Keywords
Introduction
Spinal metastases affect up to 14% of all cancer patients. 1 However, in lung cancer, the incidence of spinal invasion may reach as high as 40%. 2 Spinal canal decompression and instrumentation for spinal metastasis can prevent neurological deterioration or promote neurological recovery in patients with spinal canal compromise caused by tumor invasion. Additionally, fixation of the unstable spinal segment may relieve a patient’s pain and maintain or improve their quality of life. 3,4 However, surgery in certain patients may be precluded by a short life expectancy, where the surgical risks outweigh the benefits. 5,6 Moreover, the presence of contiguous level spinal metastases may prevent achieving stable spinal stabilization, which may lead to catastrophic instrument failure. 7 Nevertheless, advancements in systemic therapy for lung cancer, especially the development of targeted therapy, could help prolong life expectancy and promote healing of bony lytic lesions in responsive candidates. 8 –13 Therefore, the improved prognosis could lead to changes in therapeutic decision making. In this report, we present the details of two patients with non-small cell lung cancer who achieved long-term stable spinal fixation in contiguous level metastases after surgery, combined with adjuvant targeted therapy and radiation. The reporting of this study conforms to the CARE guidelines. 14
Case reports
Case 1
A 47-year-old woman presented with a 5-month history of intermittent neck pain. Prior to the spine clinic consultation, she had a history of multiple emergency room visits owing to neck pain and radicular pain in both arms, and she was treated with symptomatic pain control. She reported no history of malignancy but had a history of 20-pack-year household second-hand smoking. At the visit to our clinic, she was still able to perform her activities of daily living (ADL) independently. Physical examination showed midline cervical tenderness and paravertebral muscle spasms. Cervical range of motion was limited owing to pain, and she had minor weakness in hand gripping bilaterally (grade 4/5; left/right, respectively). The Spurling test result was positive bilaterally. Plain radiographs showed an osteolytic lesion in the C4 vertebral body. Magnetic resonance imaging (MRI) revealed multiple contiguous spinal metastasis from C2 to T2, with vertebral body collapses at C4 and C7. Computed tomography (CT) showed a 1.7-cm spiculated nodule in the left upper lung, which was a suspected primary lung cancer, and multiple lung and lymph node metastases (Figure 1). Tumor markers revealed elevated levels of carcinoembryonic antigen (CEA), cancer antigen (CA) 12-5, and CA 19-9. The provisional diagnosis was stage IV lung cancer (T1bN3M1). The patient was immobilized with a rigid cervical orthosis while awaiting surgical stabilization.
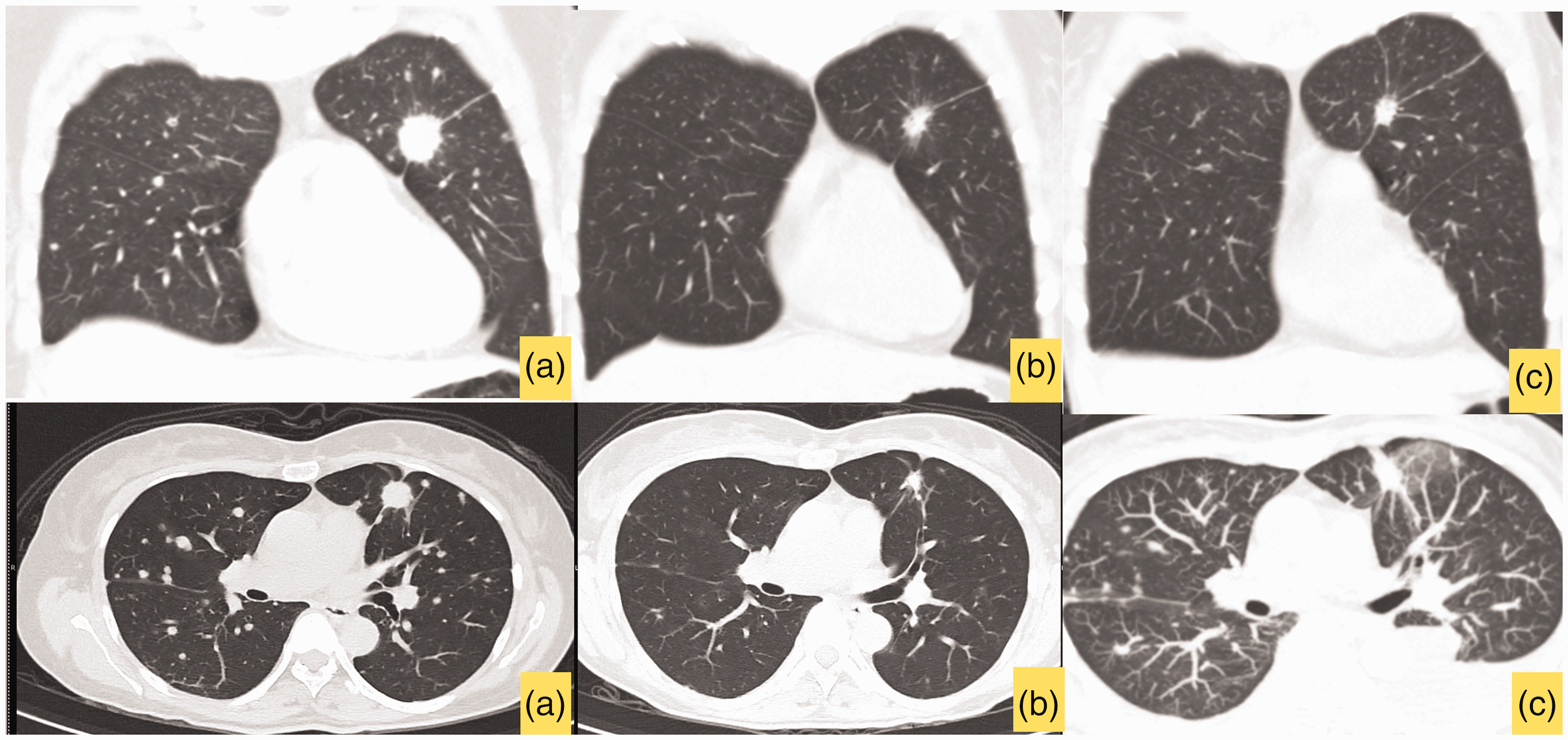
Case 1: Chest computed tomography (CT) (upper images: coronal views; lower images: axial views) (a) Initial CT scan showing a 1.7-cm spiculated mass in the left upper lung suggesting primary lung cancer, with multiple lung and lymph node metastases. (b) Four months after treatment with gefitinib, decreases in the sizes of the primary lung mass, metastatic pulmonary nodules, and lymph nodes are noted and (c) At 26 months, the patient developed EGFR TKI resistance. Disease progression is evident by the increased sizes of the primary lung mass and metastatic pulmonary nodules.
One month after the initial clinic visit, the patient developed acute incomplete spinal cord compression and presented with progressive quadriparesis, decreased sensation below the C5 level, and loss of bowel and bladder control. Her residual neurological function was graded as American Spinal Cord Injury Association (ASIA) impairment scale D below the C5 level. Radiographs revealed further collapse of the C4 vertebral body. The modified Tokuhashi score was 7, indicating an expected survival time of less than 6 months, and the spinal instability neoplastic score (SINS) was 11. The patient’s neurological function partially improved after skull traction. She subsequently underwent anterior cervical corpectomy of the C3–C5 vertebral bodies, and a fibular strut autograft was used for vertebral augmentation. Anterior plate fixation was performed from C2 to C6 (Figure 2). Postoperatively, the patient was immobilized with a custom-molded body jacket with a four-post head band, extending to the T8 level. She also underwent 30 Gy external beam radiation therapy (EBRT) from C1 to T1 in 10 fractions, and she subsequently regained nearly full motor recovery and full bowel and bladder function.

Case 1: Imaging of spinal metastatic disease (a) Initial plain radiograph (lateral view) showing an osteolytic lesion with minimal vertebral height loss in the C4 vertebra. (b) T1-weighted MRI (sagittal view) showing contiguous spinal metastasis from C2 to T6. (c) Plain radiograph (lateral view) 1 month after initial presentation showing that bony destruction has progressed, with increasing collapse of the C4 vertebra. (d) T2-weighted MRI (sagittal view) showing spinal cord compression at the C4 level and spinal metastasis from C2–T6. (e) Postoperative plain radiographs (upper image, anteroposterior view; lower image: lateral view) after anterior cervical corpectomy of C3–C5 with a fibular strut autograft and C2–C6 anterior plating. (f) Postoperative CT image (sagittal view) after systemic treatment with EGFR TKIs, EBRT, and zoledronic acid. An osteoblastic reaction is visible along the previously lytic spine and (g) Plain radiographs (upper image: anteroposterior view; lower image: lateral view) at 39 months, after posterior supplemental fixation at 7 months. The spinal construct is still durable.
Operative tissue pathology revealed metastatic adenocarcinoma, and next-generation sequencing showed epidermal growth factor receptor (EGFR) exon 19 deletion mutation. She was prescribed gefitinib, which is an EGFR tyrosine kinase inhibitor (TKI) at 250 mg per day. Follow-up CT 4 months after gefitinib therapy showed decreases in the sizes of the primary lung mass, metastatic pulmonary nodules, and lymph nodes. Seven months after the first operation, she underwent supplemental posterior instrumentation at C2–T2. Radiographs showed stable fixation without kyphosis at the previous construct. In the previously lytic C2–T6 vertebrae, increased sclerosis of the vertebral bodies was evident after systemic lung cancer therapy.
Twenty-six months after gefitinib therapy, she developed disease progression with enlarged pulmonary nodules and new metastases to the T5 and T6 vertebrae, and the skull base. Liquid biopsy revealed T790M mutation, which causes resistance to gefitinib. The patient was offered osimertinib, a third generation EGFR TKI, but she chose to continue treatment with platinum-based chemotherapy for financial reasons. She also received EBRT at the T4–T8 vertebrae and clivus and monthly intravenous zoledronic acid. At 32 months, she developed new metastases at the T8 and T12 vertebrae without neurological deficits, and she underwent palliative EBRT at the new metastatic sites. At 39 months, she developed symptomatic brain and leptomeningeal metastases and underwent whole brain radiation therapy. At 40 months, the patient and her family chose to discontinue treatment. She passed away peacefully 42 months after the surgery.
Case 2
A 77-year-old woman without a known history of malignancy presented with back pain with acute paraparesis and loss of bowel and bladder function. She was unable to perform her ADLs or ambulate independently. Her residual neurological function grade was ASIA D, with decreased sensation below the T2 dermatome. While motor function was intact in the upper extremity muscles, the motor examination grade was 4/5 in the proximal lower extremity muscles, with bilateral drop foot. MRI revealed multiple contiguous spinal metastases from the subaxial cervical region to the T6 vertebra, with index spinal cord compression at the T2 level. A bone scan showed additional bony metastases to the left side of the T12 vertebra, right iliac crest, and posterior 7th and 8th ribs. CT showed a 6 × 2.2 × 2.3-cm mass in the left upper lung with paratracheal lymph node metastasis (Figure 3). Additionally, tumor marker panels revealed an elevated CEA level. The provisional diagnosis was stage IV lung cancer (T3N2M1). The modified Tokuhashi score was 2, indicating an expected survival time of less than 6 months, and the SINS score was 11.
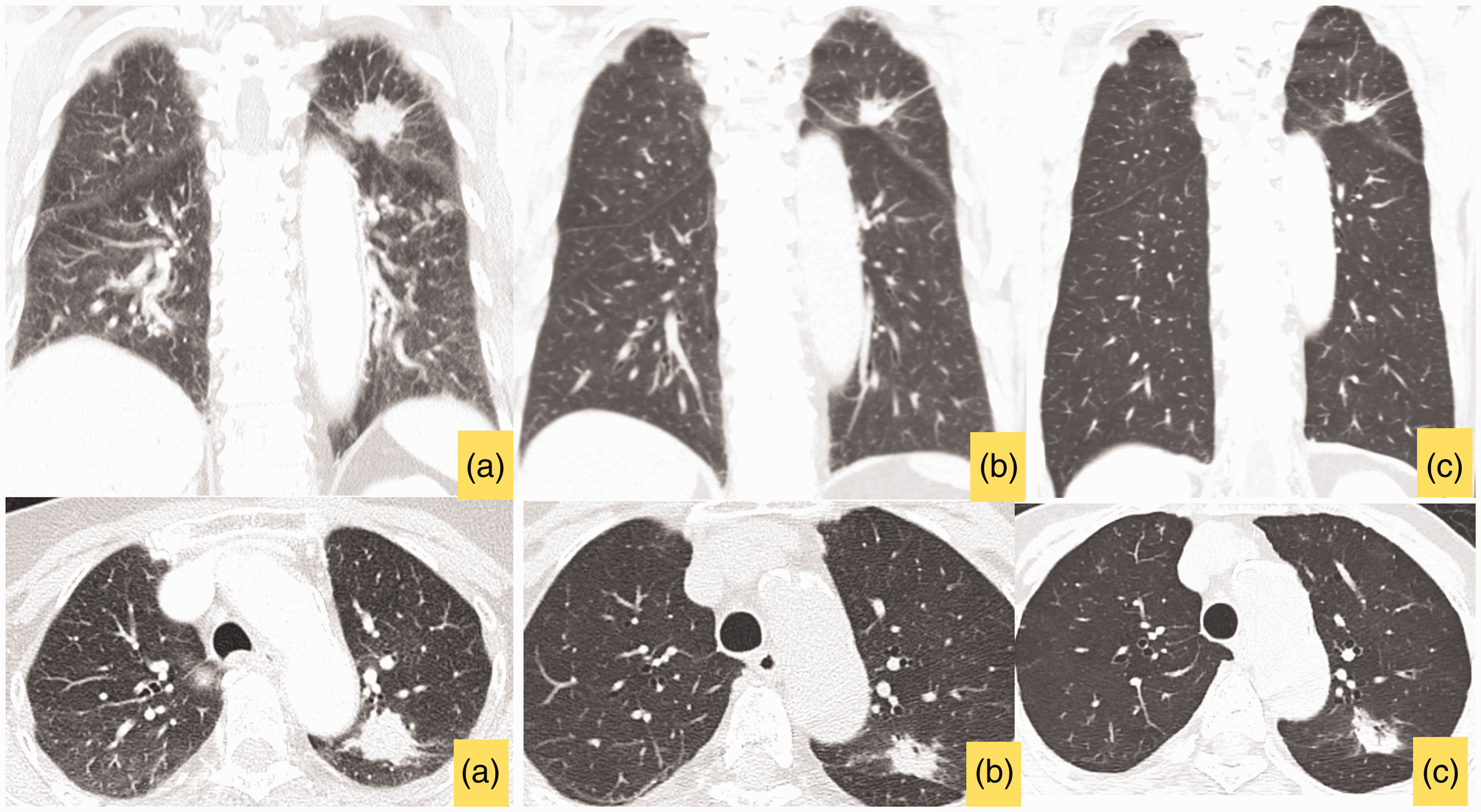
Case 2: Chest computed tomography (CT) (upper images: coronal views; lower images: axial views) (a) Initial CT images showing a large mass in the left upper lung, with paratracheal lymph node metastasis. (b) Five months after treatment with gefitinib, a reduction in the size of the primary lung mass size is observed and (c) At 24 months, the patient developed EGFR TKI resistance, which resulted in increases in the sizes of the index lung mass and paratracheal lymph nodes, and new lung metastases.
The patient underwent decompressive laminectomy at T1–T2 with transpedicular decompression at T2 and T1–T5 spinal instrumentation. Owing to bony destruction at the T1 pedicle, a transverse process hook was used at the upper instrumented vertebrae (Figure 4). Postoperatively, the patient received spinal immobilization with a sternal occipital mandibular immobilizer (SOMI) brace. Surgical pathology revealed metastatic adenocarcinoma, which was positive for the EGFR exon 21 L858R mutation. Also postoperatively, the patient was prescribed gefitinib at 250 mg per day, intravenous zoledronic acid every 3 months, and she underwent spinal EBRT. Her neurological function improved significantly, and she regained independent ADLs and ambulation. At 5 months, follow-up CT showed a reduction in the size of the lung mass to 1.3 × 1.8 × 1.4 cm. Spinal radiographs showed stable fixation and increased sclerosis of the previously lytic vertebrae.

Case 2: Imaging of spinal metastatic disease (a) Initial plain radiographs (upper image: anteroposterior view; lower image: lateral view) showing subtle osteolytic lesions along the subaxial cervical vertebrae. (b) T1- (upper image) and T2- (lower image) weighted sagittal MRI showing contiguous spinal metastasis from C4 to T6, with spinal cord compression at T2. (c) Postoperative plain radiographs (upper image: anteroposterior view; lower image: lateral view) after decompressive laminectomy at T1–T2 with transpedicular decompression at T2 and T1–T5 spinal instrumentation. A transverse process hook was applied at T1 owing to bony destruction. (d) Sagittal CT image, 5 months after treatment showing that an osteoblastic bone reaction is visible in the previously lytic regions and (e) Plain radiographs (upper image: anteroposterior view; lower image: lateral view) at 26 months showing that the spinal fixation construct is stable, without signs of implant loosening.
At 7 months, the patient developed gefitinib-induced hepatotoxicity. At 8 months, the transaminitis had not improved; therefore, she was prescribed erlotinib, another EGFR TKI. At 15 months, she developed new-onset interscapular pain. Spine MRI showed an enhanced soft tissue mass at the right lateral spinal canal, which was suspected invasion of the right C7 nerve. Chest CT revealed new pulmonary nodules in the right upper and middle lobes, and liquid biopsy confirmed drug resistance, indicated by the presence of the T790M mutation. The patient continued erlotinib after developing disease progression, and she was prescribed symptomatic pain control. At 24 months, medication failed to relieve her interscapular pain. CT revealed further disease progression with increased sizes of the index lung mass and paratracheal lymph nodes, and new lung, adrenal, and T12 and L1 spinal metastases. Erlotinib was discontinued, and platinum-based chemotherapy was initiated. After three cycles of chemotherapy, at 26 months, the primary lung tumor, and the lung and lymph node metastases had regressed significantly. Additionally, the lytic T12 and L1 vertebrae showed signs of osteoblastic changes. At this point, the patient had achieved stable disease control and continued treatment with palliative goals.
Discussion
Metastatic lung cancer was previously associated with a short life expectancy, with a reported median overall survival of 7 months without treatment. 15 The quality of life in patients with metastatic lung cancer may be negatively affected by spinal metastasis, which occurs in up to 40% of patients. 3,4 In cases where surgery is warranted, it is crucial to accurately determine the patient’s life expectancy to plan the aggressiveness of the surgical intervention. Several prognostic scoring systems have been proposed to quantify a patient’s life expectancy, which assists in therapeutic decision making. The modified Tokuhashi score has been used widely; however, its accuracy is questioned in the era of targeted therapy. 16,17
In this report, we presented two cases of lung adenocarcinoma with extensive contiguous spinal metastasis who achieved long-term survival and durable spinal instrumentation. The modified Tokuhashi scores for case 1 and case 2 were 7 and 2, respectively. Thus, the expected survival time was less than 6 months in both cases. 17 With such a short life expectancy combined with surgical difficulty indicated by contiguous spinal metastases of 11 and 10 spinal levels in case 1 and 2, respectively, the surgeons may have chosen to avoid surgery owing to the expected insecure spinal fixation and imminent risk of implant failure. Furthermore, at presentation, both patients had no known history of malignancy. Thus, the spinal decompression and fixation surgeries were performed without knowing if targetable mutations were present. Owing to the emergent treatment of spinal cord compression, we did not perform a staged tissue biopsy and waited for the pathological and mutation test results. Fortunately, tumoral tissues from the spinal metastatic sites were positive for EGFR mutations in both patients. With EGFR TKI targeted therapy, case 1 survived to 42 months, and case 2 survived to 26 months. These patient survival results contradict the life expectancies forecasted by the modified Tokuhashi score, highlighting the need for more accurate predictors of life expectancy.
The Skeletal Oncology Research Group (SORG) nomogram was developed to estimate life expectancy and showed high accuracy in estimating 3- and 12-month survival in operable spine metastatic disease. 18 However, biological factors, such as the presence of targetable mutations, were not considered in the SORG nomogram. 18 Our cases further highlight the need for incorporating targetable mutations into life-expectancy prognostication models to aid treatment decisions. This is especially important when deciding whether to perform surgery and when planning for a fixation construct, which are decisions that can be affected by longer patient survival. The presented cases had no previously known malignancy upon presentation to our clinic. Waiting for the results of EGFR mutation testing via liquid biopsy or primary tumor biopsy may not be appropriate in cases of clinical spinal cord compression. This issue further highlights that the current investigation modalities for targetable mutations may still be insufficient in the real-world setting. Furthermore, upcoming studies exploring the use of preoperative radiomics data from computed tomography and positron emission tomography imaging have shown promising possibilities for predicting EGFR mutations via artificial intelligence and machine learning, allowing for faster identification of targetable mutations. 19 –22
An EGFR mutation is reported in up to 47% of Asian patients with non-small cell lung cancer. 23 The common variants of EGFR mutation are exon 19 deletion and exon 21 L858R, as highlighted in the present cases. 24 With the presence of targetable mutations, treatment with EGFR TKIs leads to significantly longer progression-free survival (PFS) and overall survival (OS). Maemondo et al. reported that the median PFS and OS in metastatic non-small cell lung cancer patients receiving first-line gefitinib versus platinum-based chemotherapy were 10.8 months and 30.5 months versus 5.4 months and 23.6 months, respectively. 25 PFS and OS have improved further with the recent development of the third-generation EGFR TKI, osimertinib. Ramalingam et al. reported the median PFS and OS in patients receiving osimertinib was 18.9 months and 38.6 months, respectively, compared with 10.2 months and 31.8 months, respectively, in those receiving earlier-generation EGFR TKIs; i.e., gefitinib and erlotinib. 10 The limitation of this case report is that the patients were treated with first-generation EGFR TKIs, which may hinder patients’ OS compared with the OS achieved with third-generation EGFR TKIs. Nevertheless, third-generation EGFR TKIs may not be widely available in lower-income countries owing to the much higher cost.
With prolonged survival, instrumentation of spinal metastatic disease has become a challenge as implant failure may lead to catastrophic outcomes. In contiguous spinal metastasis, obtaining secure spinal fixation may be problematic and may discourage surgeons from choosing surgical interventions. In the Dutch national guideline, Bollen et al. suggested a contraindication for surgery in patients with at least three contiguous levels of spinal metastasis. 26 The results of the present cases could challenge this guideline, illustrating that stable fixation is possible even in adjacent multi-segment osteolytic spinal metastasis, after receiving targeted therapy. Prolonged systemic control and fixation durability were achieved in our cases even with the use of first-generation EGFR TKIs. This further emphasizes that precise systemic treatment is of the utmost importance in achieving good outcomes in metastatic cancer, especially in spinal metastasis cases.
The authors decided to perform staged anterior cervical corpectomy and fixation and short posterior spinal fusion in case 1 and 2, respectively. In case 1, after systemic treatment with EGFR TKIs, the previously identified spinal metastatic lesions had resolved, and osteoblastic changes were seen on the radiographs. During the staged supplemental posterior instrumentation, this bone healing allowed us to obtain stable fixation without extending the fixation to the occiput. This surgery helped to retain the patient’s cervical range of motion and preserved her quality of life. In case 2, bone healing after systemic targeted therapy helped maintain the stability of the posterior spinal fixation without the need for revision surgery for additional stability. Nevertheless, the authors recommend that physicians engage in in-depth counselling with patients and their families when deciding to perform short fixation and inform them of the risk of possible revision surgery given the patients’ frailty.
Postoperatively, the combination of radiotherapy and systemic treatment comprising chemotherapy and targeted therapy can lead to good healing of the pre-existing bony destruction caused by tumors. This healing can be further augmented by zoledronic acid or denosumab therapy to reduce bone resorption and prevent new skeletal-related events. Furthermore, recent evidence suggests that both zoledronic acid and denosumab contribute to increased PFS and OS in metastatic lung cancer patients. 27,28 With the combination of these treatment modalities, the present cases showed reactive osteoblastic change in the metastatic bone, with stable spinal fixation for almost 4 years, in one case.
Our report illustrates that prolonged survival can be achieved in metastatic non-small cell lung cancer patients treated with targeted therapies. Future prognostic scoring systems should incorporate the presence of targetable mutations to estimate remaining life expectancy. With recent advancements in systemic cancer therapies, physicians should not be discouraged from performing spinal surgery, even in contiguous metastatic disease. However, the choice of instrumentation should be planned cautiously to ensure construct durability in the light of longer patient life expectancy. With our treatment strategies, the patients in this study and their families were able to enjoy high quality of life during the patients’ remaining life expectancy despite being initially considered poor surgical candidates.
Conclusion
In this report, we presented two cases of extensive contiguous spinal metastatic disease in non-small cell lung cancer patients who achieved prolonged survival and stable spinal fixation after treatment with first-generation EGFR TKIs.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221105003 - Supplemental material for Prolonged durability of extensive contiguous spinal metastasis stabilization in non-small cell lung cancer patients receiving targeted therapy: two case reports and a literature review
Supplemental material, sj-pdf-1-imr-10.1177_03000605221105003 for Prolonged durability of extensive contiguous spinal metastasis stabilization in non-small cell lung cancer patients receiving targeted therapy: two case reports and a literature review by Pilan Jaipanya and Pongsthorn Chanplakorn in Journal of International Medical Research
Footnotes
Acknowledgements
The authors would like to thank the patients and their family members for their permission to share the patient’s case information in this report.
Author contributions
PC was the main surgeon and performed the operations. PC critically revised the manuscript, and PJ drafted the manuscript. All authors have read and approved the final manuscript.
Ethics statement
The Institutional Review Board of the Faculty of Medicine Ramathibodi Hospital approved this research (approval number: MURA 2021/885). Written informed consent to use and publish the patients’ information and images was provided by the patient for case No. 2 and by a first-degree relative for case No. 1.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.