
Abstract
Colonic mucinous adenocarcinoma rarely metastasizes to the paratesticular region, highlighting the importance of a correct diagnosis. We herein present a case involving a 65-year-old man with paratesticular carcinoma associated with scrotal swelling 1 year after radical resection of colon cancer. Computed tomography revealed a low-density tumor in the right scrotum and mild enhancement of the mass after administration of a contrast agent. The patient underwent radical surgery to remove the right testis. Pathology and immunohistochemistry revealed mucinous adenocarcinoma of the paratesticular tissue. The patient was discharged from the hospital 6 days after surgery. We reviewed the recent literature to summarize the clinical manifestations, treatments, and prognosis of this disease.
Keywords
Introduction
Colonic mucinous adenocarcinoma accounts for only 10% to 15% of all colon cancers, and metastasis to the paratesticular tissue is even less common. The prostate, kidneys, and gastrointestinal tract are the most common sites of metastasis to paratesticular tissue. 1 We herein report a case of metastatic paratesticular mucinous adenocarcinoma originating from colon cancer. We also reviewed relevant studies and discuss the diagnosis and pathway of metastasis in this article.
Case presentation
This manuscript was prepared and revised according to the CARE Checklist, and the reporting of this study conforms to the CARE guidelines. 2 A 65-year-old man presented to the First Hospital of Jilin University (Changchun, China) with a chief complaint of swelling in the right scrotum for 1 month. His history included radical resection of colon cancer (70 cm from the anal margin and hepatic flexure) 1 year previously, and postoperative pathologic examination of the lesion led to a diagnosis of moderately differentiated mucinous adenocarcinoma (pTNM: T3N1a) (Figure 1). The patient received six courses of intravenous oxaliplatin (85 mg/m2) combined with capecitabine (1.5 g twice daily). Physical examination revealed right scrotal swelling and right testicular tenderness. Laboratory markers including lactate dehydrogenase, β-human chorionic gonadotropin, and α-fetoprotein were nonspecific. Ultrasound of the scrotum revealed high echogenicity in the right scrotum and a hydrocele in the right testicular tunica vaginalis (Figure 2). Chest computed tomography (CT) findings were normal. Abdominal CT revealed a low-density shadow (61 × 51 mm2) in the right scrotum with local nodular enhancement (Figure 3). The patient underwent radical surgery to remove the right testis and ligate the spermatic cord (Figure 4). During the operation, we found that the patient had a right oblique inguinal hernia. Subsequent histopathology confirmed infiltration of mucinous adenocarcinoma in the testis, epididymis, and spermatic cord, and immunohistochemistry revealed positivity for CDX2 (Figure 5). The patient recovered well and was discharged from the hospital 6 days after surgery. Importantly, this case illustrates that testicular metastasis may be the first sign of widespread disease or that the patient already has peritoneal dissemination. Our patient was recommended to receive further treatment in the oncology department. Thus, a longer follow-up period is needed.

(a) Resection of the colon tumor located 70 cm from the anal margin and hepatic flexure and (b) Hematoxylin–eosin-stained tissue section from the patient in the present case (65-year-old man initially diagnosed with mucinous colorectal adenocarcinoma) exhibiting abundant extracellular mucin (×400).

Ultrasound of the scrotum revealed high echogenicity in the right scrotum and a hydrocele in the right testicular tunica vaginalis. Some point-shaped blood signals were found on color Doppler flow imaging.
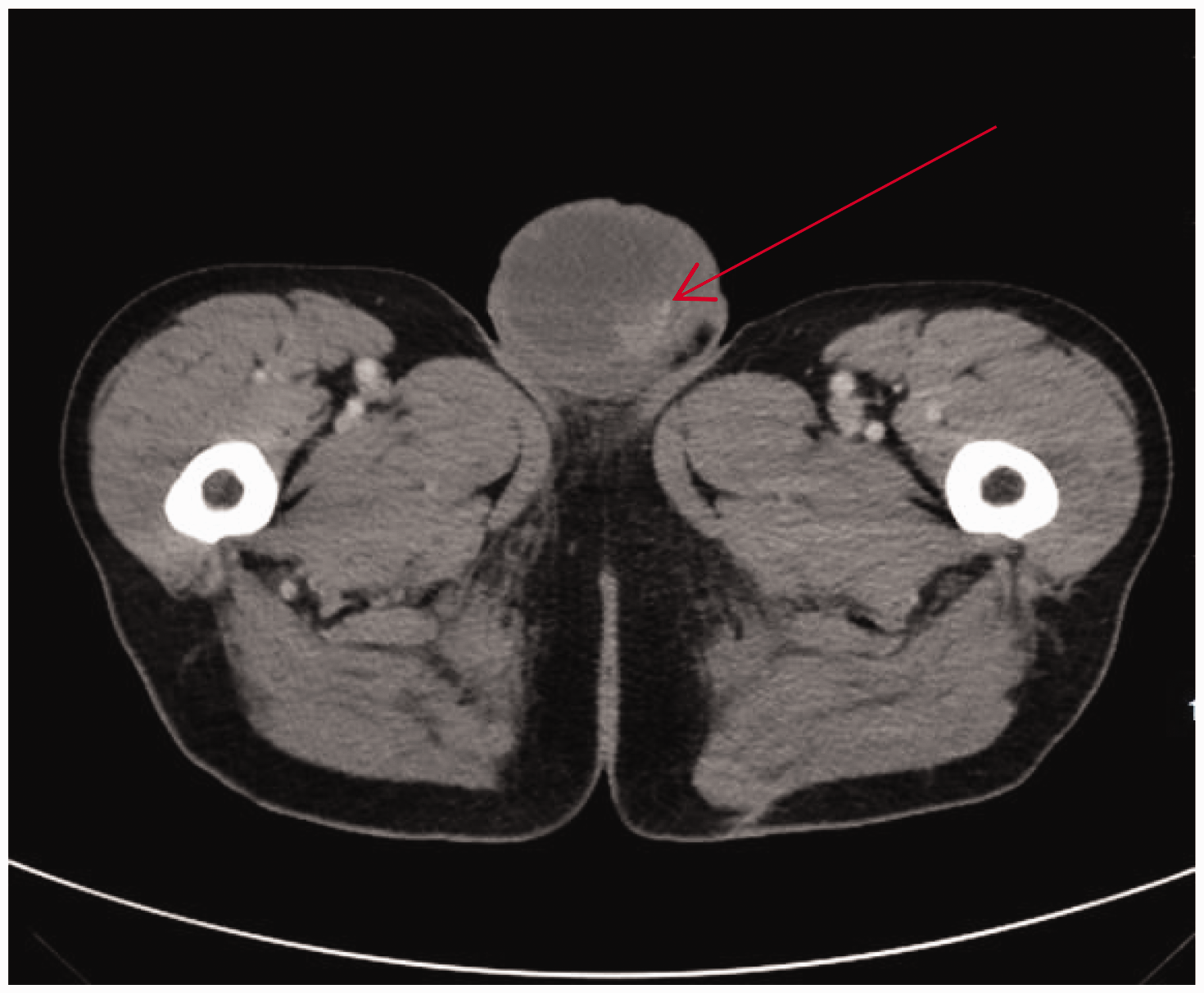
Abdominal computed tomography revealed a low-density shadow in the right scrotum (61 × 51 mm2) with local nodular enhancement.

On gross examination, a light brown mass (4 × 3 × 2 cm3) and hydrocele were present in the tunica vaginalis of the right testis.

Hematoxylin–eosin staining and immunohistochemistry of the specimen. (a) Hematoxylin–eosin-stained specimen and (b) On immunohistochemistry, the specimen was positive for CDX2 (×100).
Discussion
Colon cancer is one of the most common causes of cancer-related death. Globally, approximately 400,000 people die of colorectal cancer and 700,000 new cases are diagnosed annually.1,3 Adenocarcinoma is the most common pathological type of colon cancer, whereas mucinous adenocarcinoma accounts for only 10% to 15% of colon cancers. 4 In general, the regional lymph nodes represent the most common site of colon cancer metastasis (50%–70%). However, an axillary mass can develop several years after successful hemicolectomy. The occurrence is rare, but liberal use of positron emission tomography/CT scans and the semi-dry dot-blot technique is encouraged to diagnose metastasis early. 5 Other sites of metastatic spread include the liver (35%–50%), lungs (21%), and bone (8.7%).4,6 Metastasis of colon cancer to the scrotum is extremely rare; we have herein described such a case. Similar cases are summarized in Table 1.
Clinical characteristics of cases of colonic mucinous adenocarcinoma with paratesticular metastasis.

Ref, reference number; NR, not recorded; CR, colon resection; OR, orchiectomy; WLR, wedge lung resection.
The incidence of a secondary testicular tumor on biopsy ranges from 0.02% to 2.5%, and approximately 200 cases of testicular metastasis have been reported globally.7,8 Bunn et al. 9 reported a case of a 29-year-old man with paratesticular mucinous adenocarcinoma of the lungs. Gastric carcinoma and appendiceal adenocarcinoma are other differential diagnoses of mucinous paratesticular tumors.8,10 Seo et al. 11 reported that the prostate, kidneys, gastrointestinal tract, lungs, and breasts were the most common sites of metastasis of paratesticular tissue. Another study showed that testicular metastatic mucinous tumors were more common than primary mucinous testicular tumors, and metastatic tumors were characterized by multifocality, obvious testicular stroma growth, and conspicuous vascular stroma involvement. 12 In other studies, metastatic tumors of the testes were often accompanied by a hydrocele of the tunica vaginalis.8,13 The authors considered that the most important components of the differential diagnosis were identifying the location of the primary cancer and analyzing the cases of metastatic cancer. In our case, the testicular tumor was considered a metastatic lesion because the patient had undergone radical colon cancer resection.
Metastasis of colon cancer to the scrotum is rare. In addition to lymphatic and vascular routes, there are several other pathways by which colon cancer may metastasize to the scrotum. These pathways include retrograde venous extension and direct invasion, transperitoneal seeding, and arterial embolization.8,11,12,14 In the present case, we believe that the tumor moved along the peritoneum to the testis because the patient had a right oblique inguinal hernia. Thus, we suggest that hernias should be repaired during radical colon cancer resection to reduce the possibility of metastasis.
Secondary testicular tumors should be differentiated from primary testicular tumors before surgery. The detection of α-fetoprotein, human chorionic gonadotropin, and lactate dehydrogenase has great reference value in the diagnosis, staging, treatment, and prognosis of testicular tumors. Because CDX2 plays important roles in the occurrence, development, and metastasis of colorectal cancer, we believe that testicular tumors may originate from colon cancer metastasis. Surgery is the main treatment for secondary testicular tumors, and the basic methods are orchiectomy and retroperitoneal lymphadenectomy.
Conclusion
Secondary paratesticular mucinous adenocarcinoma is extremely rare. The differential diagnosis should aim to identify the site of the primary tumor. The main treatment method is surgery, including orchiectomy and retroperitoneal lymphadenectomy. Because the prognosis of mucinous adenocarcinoma is poor, whether to administer adjuvant treatment should be determined according to the pathological nature and stage of the lesion. Furthermore, if the patient has an indirect inguinal hernia, repair of the hernia is recommended to reduce the probability of metastasis.
Footnotes
Ethics statement
Study protocol approval was not required because this is a case report. Written informed consent was obtained from the patient for publication of the case report and accompanying images. All details have been deidentified to protect the patient’s identity.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
Min Liu and Yanpeng Fan are the first co-authors and contributed equally to this work. Min Liu and Yanpeng Fan wrote the manuscript. Senqiang Zhu revised the manuscript. Shusheng Zhu designed the structure of the review and revised the manuscript. All authors contributed to the article and approved the submitted version.