
Abstract
Aneurysmal bone cyst is a type of benign bone pathology with expansile and osteolytic features whose etiology remains unclear. Graves’ disease is an autoimmune disease characterized by diffuse goiter and hyperthyroidism. Moyamoya disease is a progressive cerebral vasculopathy. It has been reported that Graves’ disease and Moyamoya disease share a similar etiology involving cytokines and autoimmune and genetic factors. There are no previous reports regarding the relationship between aneurysmal bone cyst and Graves’ disease. Here, we present the rare case of a 25-year-old woman with suspected aneurysmal bone cyst of the left proximal femur and a definite preoperative diagnosis of Graves’ disease, in whom lesion resection combined with left total hip replacement was indicated. Biopsy confirmed the diagnosis of aneurysmal bone cyst. Three days postoperatively, the patient developed acute ischemic cerebral infarction owing to Moyamoya disease, which was subsequently confirmed. This case elucidates the potential interaction among aneurysmal bone cysts, Graves’ disease, and Moyamoya disease and provides lessons regarding appropriate perioperative preparation for patients with Graves’ disease who require surgery to avoid potential severe complications.
Keywords
Introduction
Aneurysmal bone cyst (ABC) is a type of benign bone pathology with expansile and osteolytic features. 1 ABC accounts for approximately 1% of all bone tumors, and more than 70% of cases are seen in individuals younger than 30 years old. 2 ABC is commonly encountered in long bones like the femur, tibia, and humerus; 70% of cases are considered a primary lesion without any preexisting bone disease, and the remaining cases are considered secondary to a known antecedent osseous lesion.3,4 Since it was first reported in 1942, 5 ABC has been studied for more than 60 years. However, the underlying pathogenesis of ABC is still ambiguous. Several etiological hypotheses regarding ABC has been put forward, including posttraumatic bone architecture aberrance, hemodynamic abnormality, and genetic predisposition.1,3,6
Graves’ disease (GD) is an autoimmune disease characterized by the production of thyroid stimulating hormone receptor antibody (TRAb) in the blood, resulting in diffuse goiter and hyperthyroidism. 7 Moyamoya disease (MMD) manifests as progressive vasculopathy in cerebral vascular stenosis and compensatory malformation of net-like collateral vessels. 8 It has been reported that GD and MMD share a similar etiology involving cytokines and autoimmune and genetic factors. 9 These two diseases also possess a common pathological correlation with T-lymphocyte dysregulation. 10 More interestingly, GD and MMD have been found together in the same individual. In patients with MMD but without GD, elevation of thyroid autoantibodies is frequently encountered; additionally, thyrotoxicosis can worsen the ischemic condition of MMD.10,11 This indicates a complicated interaction between GD and MMD.
Here, we present the rare case of a 25-year-old woman with suspected ABC of the left proximal femur and a definite preoperative diagnosis of GD in whom en bloc resection of the lesion combined with left total hip replacement was indicated. Three days postoperatively, the patient developed acute ischemic cerebral infarction owing to MMD, which was undiscovered preoperatively. To the best of our knowledge, no previous case of ABC concomitant with GD and MMD has been reported. The lessons drawn from our experience in this case can serve to broaden our understanding and provide valuable information for clinical practitioners regarding the management of similar cases in the future.
Case report
A 25-year-old woman was admitted to our ward complaining of pain and limited movement in the left hip after a fall 6 hours earlier. She had no previous symptoms in her left hip nor any prior similar trauma. Diffuse goiter was found 3 years earlier, but she had not consulted a physician and had not received any treatment. Her history was otherwise unremarkable. The reporting of this case conforms to the CARE guidelines. 12
On admission, physical examination revealed shortening and external rotation of the left lower limb with slight exophthalmos. Significant tenderness at the left inguinal region and grade II enlargement of the thyroid gland were found on palpation. Radiography of the left hip revealed a fracture of the left femoral neck, with a large cystic osteolytic lesion involving the left femoral head and neck and the greater trochanter region (Figure 1a). Computed tomography (CT) indicated a vacuous medullary space expanding from the left femoral head to the greater trochanter region, except for the fracture of the left femoral neck. The cortex of the proximal femur was intact (Figure 1b and 1c). Magnetic resonance imaging (MRI) demonstrated a lobular lesion with septa in the left femoral head on a T2-weighted axial sequence (Figure 1d).

Preoperative and postoperative imaging of the patient’s left hip. (a) X-ray revealed fracture of the left femoral neck, with a large cystic osteolytic lesion involving the left femoral head and neck and the greater trochanter region. (b-c) CT scan revealed a vacuous medullary space expanding from the left femoral head to the greater trochanter region with intact cortex and (d) T2-weighted axial sequence on MRI demonstrated a lobular lesion with septa in the left femoral head.
The lesion of the left proximal femur was highly suspicious for ABC. Because the nature of the lesion was undefined and the bone structure was extensively damaged, a treatment protocol of en bloc resection of the lesion combined with total hip replacement was proposed. However, the patient’s preoperative examination results were abnormal, with serum thyrotropin (<0.01 mIU/L, reference range (RR): 0.27–4.2 mIU/L), triiodothyronine (>10 nmol/L, RR: 1.3–3.1 nmol/L), thyroxine (>320 nmol/L, RR: 66–181 nmol/L), free triiodothyronine (41.1 pmol/L, RR: 3.1–6.8 pmol/L), free thyroxin (>100 pmol/L, RR: 12–22 pmol/L), anti-thyroperoxidase antibody (352 IU/mL, RR: <34 IU/mL), anti-thyroglobulin antibody (3652 IU/mL, RR: <115 IU/mL), and TRAb (14.1 IU/L, RR: 0–1.75 IU/L). Additionally, ultrasonography of the neck showed diffuse enlargement of the thyroid gland. Thus, an endocrinology consultation was requested, and the diagnosis of GD was subsequently confirmed. It was suggested that the scheduled operation could not be performed until thyroid hormone levels were under control. Accordingly, anti-thyroid drug therapy was initiated. Once thyroid hormone levels were controlled, the proposed surgery was carried out (Figure 2). Postoperatively, histological results from biopsy of the lesion confirmed the diagnosis of ABC (Figure 3).

Radiograph of the left hip after surgery.

Histologic findings. (a) Low-magnification histological slice demonstrating multiple cystic spaces filled with red blood cells (magnification: 10X) and (b) High-magnification histological slice showing osteoclast-like giant cells (arrows) (magnification: 20X).
Three days after surgery, the patient developed sudden aphasia, flattening of the left nasolabial fold, and disability of the left upper limb. A subsequent head CT scan showed acute infarction of the bilateral frontal and parietal lobes (Figure 4a), corresponding to hyperintense lesions on diffusion-weighted imaging (DWI) in MRI (Figure 4b). Magnetic resonance angiography (MRA) of the head revealed occlusion of the right middle cerebral artery with multiple cerebral artery stenoses (Figure 4c). After consultation with a neurosurgeon, the diagnosis of MMD was confirmed. The patient was transferred immediately to the neurosurgery department for further treatment.
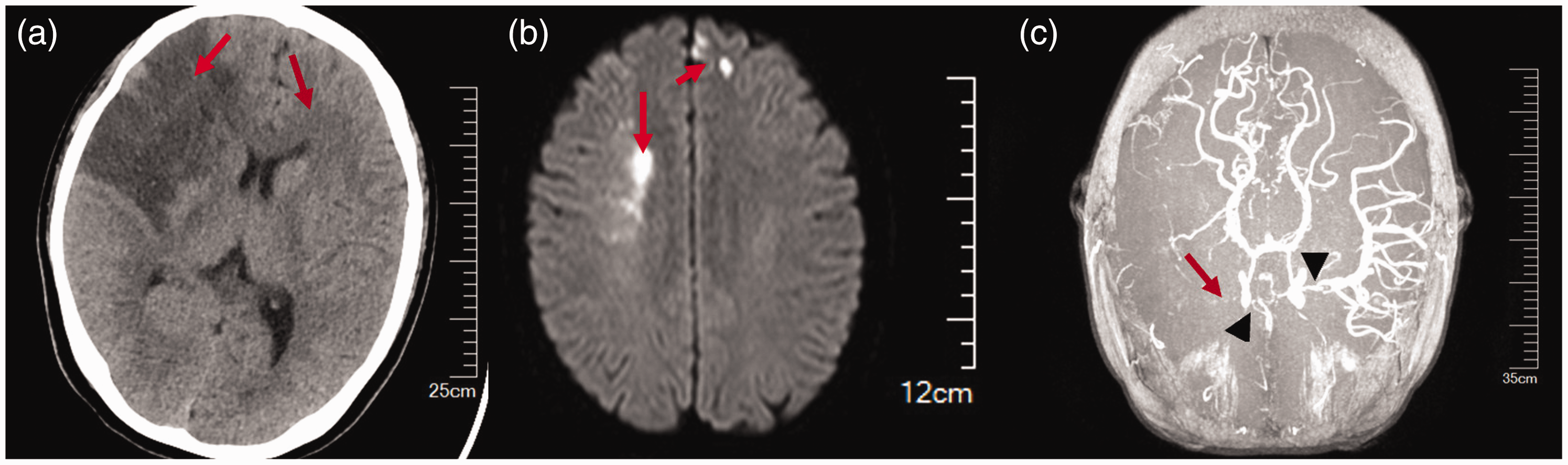
Results of head imaging. (a) Acute infarction of bilateral frontal and parietal lobes (arrows) corresponding to (b) hyperintense lesions on DWI sequence in MRI (arrows) and (c) MRA showing occlusion of the right middle cerebral artery (arrow) with multiple cerebral artery stenoses (arrowheads).
Discussion
In the bone remodeling cycle, osteoblast-mediated bone formation activity and osteoclast-mediated bone resorption activity are kept in balance to maintain bone homeostasis. 13 It has been clarified that under the condition of hyperthyroidism, the activity of osteoclasts is enhanced whereas that of osteoblasts is attenuated, leading to bone loss. 14 In patients with hyperthyroidism, substantial calcium loss can be observed, which leads to negative calcium balance and increases the risk of osteoporosis and pathological fractures. 15 However, no previous reports are available regarding the relationship between hyperthyroidism and the development of ABC. In the present case, the diagnosis of ABC in the left proximal femur was confirmed via biopsy. There is no doubt that the patient developed ABC and GD preoperatively. According to the theory of negative calcium balance mentioned above, the activity of bone resorption should be much more active than that of bone formation in this patient. Theoretically, it is plausible that excessive thyroid hormone levels may drive the development of ABC through the activation of osteoclasts. However, no previous data are available elucidating the link between ABC and hyperthyroidism; thus, further research is warranted.
In clinical settings, cases of MMD concurrent with GD are rarely encountered. However, once concurrent with MMD, GD may increase the risk of developing ischemic cerebral infarction owing to the condition of hyperthyroidism. 10 Thyrotoxicosis will also aggravate the ischemic situation in MMD. 11 The underlying reason for this is unknown, but several pathological mechanisms have been proposed. First, thyrotoxicosis tends to induce hypermetabolism and increases oxygen consumption in the brain. 11 Second, excessive thyroid hormone levels contribute to vessel malformation and vasoconstriction through sympathetic nervous system activation.9–11 Additionally, T-lymphocyte dysfunction can result in vascular dysregulation and vessel wall hyperplasia.9,10 Furthermore, high thyroid hormone levels may lead to hypercoagulability and homocysteinemia, which augments the risk of developing cerebral infarction. 11 Certain synchronous changes between the hyperthyroid state and cerebral ischemic events have been observed; cerebral ischemic symptoms in MMD become intensified under the state of thyrotoxicosis and are alleviated with normal thyroid function. 11
Despite administration of anti-thyroid drugs and normalization of thyroid function preoperatively, our patient developed acute ischemic cerebral infarction 3 days after surgery. We hypothesized that the operation induced a stress response and activated the sympathetic nervous system, which may have resulted in direct cerebral vasoconstriction and the subsequent infarction event. However, activation of the sympathetic nervous system can also lead to thyrotoxicosis or a thyroid storm, which in turn enhances activity of the sympathetic nervous system. Such a vicious circle can reasonably have triggered the cerebral infarction event. Additionally, the operation itself, which caused blood volume loss, may have exacerbated the ischemic condition of the cerebrum. Cerebral fat embolism (CFE) is a rare syndrome seen in long bone fracture and total hip or knee replacement. 16 The diagnosis of CFE is usually based on clinical manifestations and imaging. In most cases of CFE, apart from aphasia and hemiplegia, consciousness disorder and even coma are typically observed in patients. 17 However, CT scan of the head seldom reveals any abnormality. 17 The gold standard for CFE is the DWI sequence in MRI, on which multifocal, scattered, and small hyperintense lesions can be observed in the acute stage, which is known as the “starfield pattern.”16,17 In the present case, first, the patient showed aphasia and hemiplegia without consciousness state alteration. Second, head CT scan revealed hypointense lesions of the bilateral frontal and parietal lobes, corresponding to focal hyperintense lesions on DWI in MRI. Thus, the diagnosis of acute cerebral infarction could be confirmed.
Diverse treatment protocols have been proposed for ABC, including arterial embolization, curettage and bone graft, cryotherapy, sclerotherapy, radionuclide ablation, and en bloc resection.3,6 As revealed on imaging, the lesion in our patient had destroyed most of the left proximal femur, with involvement of the femoral head and neck and the greater trochanter region. Such substantial bone loss necessitates curettage and bone graft or en bloc resection. Taking curettage and bone graft into consideration, a large autogenous bone and even vascular bone graft was warranted, which could induce donor site complications and lengthen the time of surgery. It has been pointed out that with massive bone destruction of the femoral neck owing to benign or malignant lesions concurrent with pathological fracture, total hip replacement is indicated, 18 and en bloc resection for ABC has the lowest rate of recurrence.3,19 Therefore, we chose en bloc resection of the lesion combined with uncemented total hip replacement.
To our knowledge, no previous case has been reported regarding ABC concomitant with GD and MMD. Several valuable lessons for clinical practitioners can be drawn from this case. First, because we were unaware of the link between GD and MMD, the diagnosis of MMD in this patient was not confirmed preoperatively; this diagnosis was not confirmed until the development of acute ischemic cerebral infarction 3 days after surgery. This event should sound a cautionary note that when dealing with patients who have GD and require surgery, additional examinations must be conducted to rule out the concurrence of MMD so as to prevent postoperative complication with cerebral infarction. Second, despite control of thyroid hormone levels in patients with GD and MMD, the impact of surgery may aggravate the ischemic condition of the cerebrum through thyrotoxicosis or blood volume loss. Apart from controlling thyroid hormone levels preoperatively in these patients, close monitoring of thyroid function and blood volume should also be conducted postoperatively. Moreover, control of blood pressure during the perioperative period is of great importance to protect against ischemic cerebral infarction. In retrospect, we did not regularly monitor the patients’ blood pressure because we failed to understand the importance of blood pressure control.
The scant data available regarding the patient’s blood pressure revealed 120–145/79–90 mmHg, averaged 132/83 mmHg preoperatively, compared with 101–138/42–77 mmHg, averaged 117/58 mmHg postoperatively. It is obvious that her blood pressure before the operation was much higher than that after surgery. We neglected to control blood pressure during and after the operation, which may be a cause of the cerebral infarction event. Lastly, although no previous data are available regarding the relationship between ABC and hyperthyroidism, our patient’s past history revealed a diagnosis of GD but she was otherwise healthy. Hyperthyroidism may play a role in the course of ABC, but it is unclear whether this patient developed GD prior to ABC. The interaction between GD and ABC is still obscure and warrants further investigation. It is unknown whether the simultaneous occurrence of ABC, GD, and MMD in this patient was a coincidence.
In conclusion, we described a case of ABC in the left proximal femur concomitant with GD and MMD. Our patient had a history of thyroid goiter and suspected ABC of the left proximal femur. In preoperative examination, we confirmed the diagnosis of GD, and postoperative biopsy confirmed ABC of the left proximal femur. After surgical en bloc resection of the lesion combined with total hip replacement, the patient developed acute ischemic cerebral infarction. The diagnosis of MMD was subsequently confirmed on further examination. She was transferred to the neurosurgery department for further management. To our knowledge, this is the first case regarding ABC concomitant with GD and MMD. This case elucidates the potential interaction among aneurysmal bone cyst, GD, and MMD and provides information regarding appropriate perioperative preparation for patients with GD who require surgery to prevent potential severe complications. The valuable lessons drawn from this case broaden our understanding of this rare presentation and our experience can help clinical practitioners in the management of similar cases. The potentially novel concepts regarding the pathogenesis of ABC that arise from this case warrant further investigation.
Footnotes
Ethics statement
The patient provided written informed consent for treatment and for publication of this case and her data for scientific purposes. Ethical approval and informed consent was not required because we only reported a patient case.
Data availability statement
The data used to support the findings of this study are available from the corresponding author upon request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
Wen-Xue Jiang designed the study, Gao-Rui Cai and Guo-Neng Chen collected the data, and Gao-Rui Cai wrote the paper.