
Abstract
Mullerian cysts are benign tumors that are very rare in the posterior mediastinum. It is necessary to distinguish Mullerian cysts from benign tumors or other types of cyst in the posterior mediastinum. A 42-year-old woman visited our hospital for a routine check-up, and a mediastinal mass was identified on chest computed tomography (CT). Contrast-enhanced chest magnetic resonance imaging (MRI) revealed a 4.0 × 2.6 × 2.8-cm mass, and a neurogenic tumor or esophageal cyst was suspected. Single-port thoracoscopic surgery was performed for cyst removal. Histopathological examination of the resected tissue revealed that the cyst wall was covered with a single layer of ciliated columnar epithelium. Immunohistochemical staining revealed positivity for paired box gene 8 (PAX8), Wilms tumor protein 1 (WT-1), estrogen receptor (ER), and progesterone receptor (PR). Therefore, a diagnosis of mediastinal Mullerian cyst was made. Mediastinal Mullerian cysts should be included in the differential diagnosis of posterior mediastinal cysts. Cystic lesions in the posterior mediastinum should be removed surgically and undergo immunohistochemical examination.
Keywords
Introduction
Cysts of the mediastinum, which are benign masses and relatively uncommon, represent 12% to 18% of all primary mediastinal lesions. The classification of mediastinal cysts comprises a broad range of etiologies, such as neurogenic tumors, bronchogenic cysts, mesothelial cysts, thymic cysts, and other types. 1 Mullerian cysts in the mediastinum were first described by Hattori. 2 Since then, several studies have reported mediastinal Mullerian cysts. We report a case of Mullerian cyst in the mediastinum in a 42-year-old female patient. To the best of our knowledge, this is the first case report of surgical resection of a mediastinal Mullerian cyst in China. The reporting of this study conforms to the CARE guidelines. 3
Case report
A 42-year-old woman visited our hospital for a routine checkup, and a mass was incidentally found on chest computed tomography (CT). She was mildly hypertensive, denied any notable family history, had no history of gynecological abnormalities, was not overweight, and did not complain of any symptoms. Physical examination findings and laboratory test results were unremarkable. Contrast-enhanced chest magnetic resonance imaging (MRI) identified a 4.0 × 2.6 × 2.8-cm, well-defined cyst in the right posterior mediastinum with slight compression of the trachea (Figure 1). Radiologic evaluation indicated a benign tumor, such as a neurogenic tumor with cystic change or an esophageal cyst. The patient underwent tumor resection by video-assisted thoracoscopic surgery. Grossly, the mass was a round unilocular cyst with a thin, translucent wall containing clear watery liquid.

Chest contrast-enhanced computed tomography (a) and axial magnetic resonance images (b) showing a well-defined ovoid thin-walled cystic mass without enhancement (arrows) in the right paravertebral space adjacent to the fourth vertebra and (c) Chest coronal T2-weighted magnetic resonance image showing a homogenous cyst with a high-intensity signal equal to that of the density of water.
Single-port thoracoscopy was performed via an incision at the anterior axillary line of the right 4th intercostal space. The cyst was located above the azygous vein and was in close proximity to the vertebral body. After careful dissection, the absence of adhesions or communication between the tumor and the surrounding tissue was confirmed except for contact with the azygous vein. The cystic contents comprised watery, transparent fluid, and the cyst wall was thin and translucent. The azygos arch was divided and ligated to facilitate the exposure for surgery. The cyst was completely removed using the Ligasure vessel sealing system (Valleylab, Boulder, CO, USA) (Figure 2). Postoperatively, a chest tube was placed through the incision to drain effusions from the thoracic cavity.
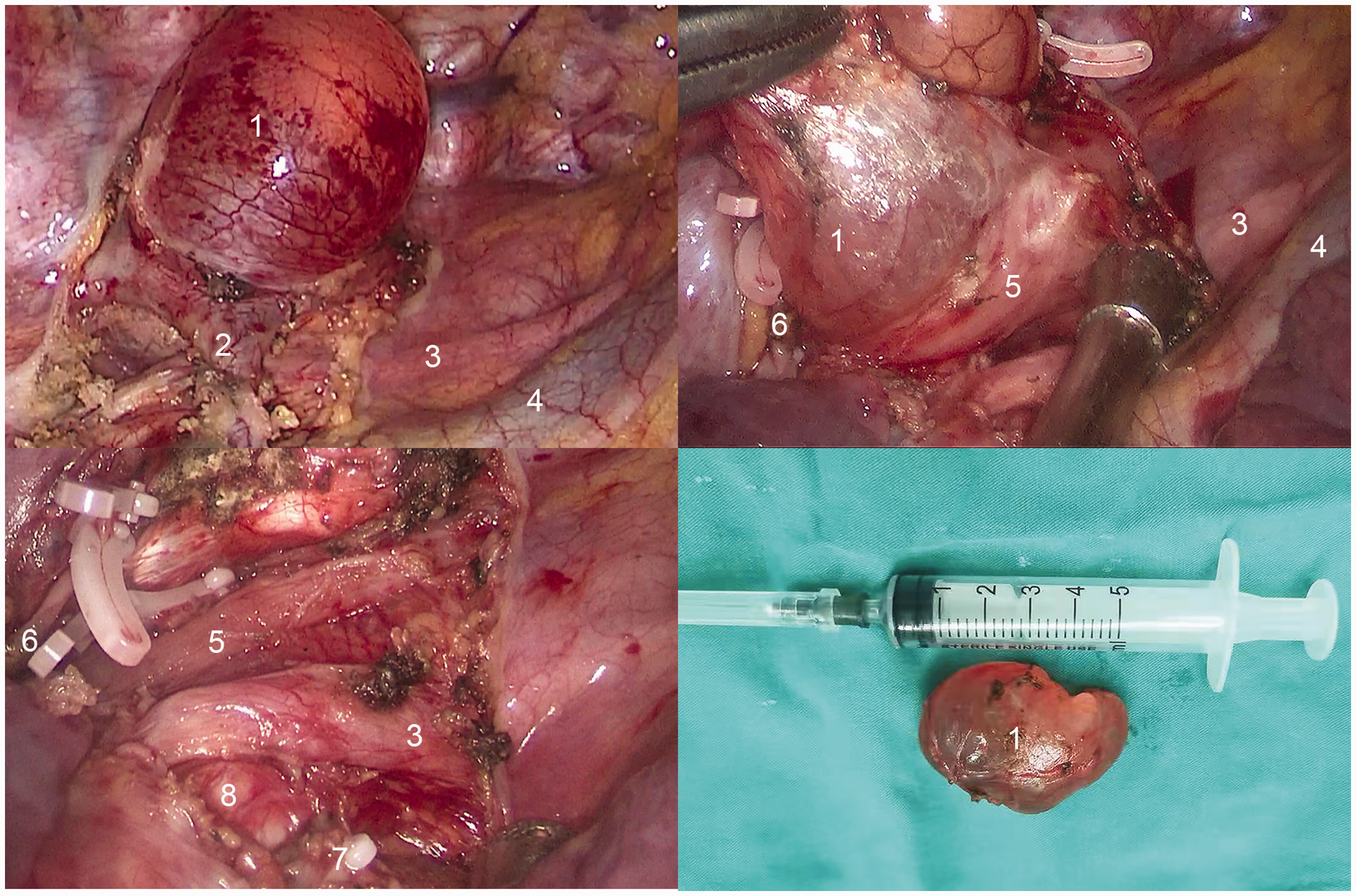
Thoracoscopic resection of a Mullerian cyst. 1. cyst, 2. azygos arch, 3. right vagus nerve, 4. superior vena cava, 5. esophagus, 6. distal azygos arch stump, 7. proximal azygos arch stump, and 8. right main bronchus.
The excised cyst stained positive with immunohistochemical stains for paired box gene 8 (PAX8), Wilms tumor protein 1 (WT-1), estrogen receptor (ER), and progesterone receptor (PR) (Figure 3). The final diagnosis was a Mullerian cyst. There were no postoperative complications (Figure 4). The patient was discharged on the second postoperative day after the chest tube was removed, and there was no recurrence during the 6-month follow-up.

Histopathological image showing the cystic wall lined by a single layer of ciliated columnar epithelial cells, in which some epithelial cells have a clear cytoplasm. The morphology is similar to that of the fallopian tube, and distribution of a thin layer of smooth muscle tissue is seen under the epithelium (hematoxylin and eosin, ×200; left image) (hematoxylin and eosin, ×400; right image).

Chest X-ray on the first postoperative day.
Discussion
Paravertebral and paraspinal tumors in the posterior mediastinum are predominantly neurogenic in origin, and bronchial cysts and pericardial cysts are not uncommon. Mullerian cysts commonly develop in the male pelvis, where the Mullerian duct is retained, although female Mullerian cysts in the retroperitoneum and mediastinum have also been reported. 4 Syred and Weissferdt stated in a review that the paravertebral location in the posterior mediastinum is the exclusive site for Mullerian cysts. 5 In our case, both radiologically (CT, MRI) and intraoperatively, the lesion was diagnosed as a neurogenic tumor/cyst, esophageal cyst, or enteric cyst. However, positive postoperative immunohistochemical staining for PAX8, WT-1, ER, and PR did not support these differential diagnoses. The ER and PR expression and the histologic similarity to fallopian tubes with the ciliated columnar epithelium followed by a smooth muscular layer revealed the Mullerian origin. The expression of cytokeratin 5/6 was negative in our case, which is also a good marker for differentiating both bronchogenic cysts and pericardial cysts from mediastinal cysts with Mullerian differentiation. 6 Currently, PAX8 immunohistochemical staining is used to identify Mullerian tumors, among others.7,8 Immunostaining for WT1 was also positive in our case, which lent further support to a Mullerian origin for the cyst.
The Mullerian ducts, derived from the mesoderm in embryos of both genders, are also called the paramesonephric ducts; however, these ducts go on to develop the reproductive organs only in female embryos. Mullerian cysts are lined by epithelium derived from the Mullerian ducts and may originate from any part of the Mullerian ducts. The etiology of Mullerian cysts may be associated with renal agenesis, and these cysts are usually seen in the abdomen and pelvis. Clinically, Mullerian cysts in female patients, also known as paraventricular cysts, are extremely rare. Mediastinal cysts composed of Mullerian epithelium are a recently recognized entity.3,9 Konishi et al. postulated that the lesion described in their case report was derived directly from the primary Mullerian apparatus itself, which could also be applicable to the lesion in our case. 10 Alternatively, the lesion in our case could have been derived from misplaced mesothelium and mesenchyme with the characteristics of the secondary Mullerian system.
Two retrospective analyses reported the incidence of Mullerian cyst in mediastinal cysts as 15.8% (3/19) 3 and 5.5% (9/163), respectively. 6 These studies show that Mullerian cysts may not be that rare. After the first report by Hattori, 9 to date, 29 cases of Mullerian cysts have been reported, including our case.6,11 –18
Mullerian cysts generally occur in women 40 to 60 years of age and most are asymptomatic.15,19 The median size of Mullerian cysts is approximately 30 mm, and the majority of the reported cases occurred near the Th4 vertebra.11,12 Our case was in a 42-year-old woman who had no previous history of gynecological abnormalities and who was not overweight, which are findings that differ slightly from those in previous reports. 3 In our case, the Mullerian cyst occurred near the right Th4 vertebra, and the cyst was positive for both estrogen and progesterone receptors. These findings are consistent with the characteristics of Mullerian cysts in previous reports. In all reports, including in our case, the cyst was filled with watery liquid. We took care to protect the cystic capsule from damage during the resection, and we removed the entire cyst.
Conclusion
Mediastinal Mullerian cysts should be included in the differential diagnosis of posterior mediastinal cysts. These cysts have a benign behavior, and the prognosis is presumed to be good after surgical removal. Immunohistochemical examination of resected mediastinal Mullerian cyst tissue is warranted to avoid misdiagnosis.
Footnotes
Authors' contributions
KK performed the literature search and wrote the manuscript; SW designed the study and revised the manuscript; BL contributed to writing the manuscript; MW contributed to the figure processing; FX was involved in drafting the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Hubei Cancer Hospital (no. LLHBCH2022YN-010). The patient provided written informed consent prior to surgery.
Consent for publication
Written informed consent for publication of this case report was obtained from the patient.
Declaration of conflicting interest
The authors have no competing interests to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.