
Abstract
Granulocyte-colony stimulating factors (G-CSFs) are the cornerstone of peripheral blood stem cell mobilization and apheresis. However, splenic rupture following G-CSF treatment represents a serious and potentially fatal adverse event. Here, we report the case of a patient in their late 50s with severe pancytopenia post-autologous stem cell transplantation reinfusion suffering from splenic rupture after treatment with lenograstim. We also reviewed the literature describing cases of splenic rupture during G-CSF administration.
Keywords
Introduction
Granulocyte-colony stimulating factors (G-CSFs) represent the cornerstone of peripheral blood stem cell (PBSC) mobilization and apheresis. Furthermore, these drugs are used for the treatment of chemotherapy-induced neutropenia in patients with non-myeloid malignancies receiving myelotoxic chemotherapy because they increase white blood cell proliferation, maturation and functional capacity. 1 G-CSF therapy is generally safe and well tolerated in patients with oncohematological diseases and healthy subjects, with the exception of extremely rare but important side effects, such as myocardial infarction, stroke and splenic rupture. Atraumatic splenic rupture (ASR) represents a rare but poorly recognized life-threatening condition. 1 A limited number of splenic rupture cases following G-CSF administration for chemotherapy-induced neutropenia and mobilization procedures has been described in the literature in patients with hematological diseases undergoing autologous hematopoietic stem cell transplantation (ASCT) and healthy donors. 1
Here, we report the case of a male patient with mantle cell non-Hodgkin lymphoma (MCL) suffering from splenic rupture and severe pancytopenia post-ASCT reinfusion during lenograstim treatment who was successfully treated with emergency open splenectomy. A review of the literature was also performed to describe cases of splenic rupture during G-CSF administration.
Case report
A man in his late 50s was diagnosed with MCL stage IIIA according to the Ann Arbor classification in February 2011 at another center. His past medical history included Graves’ disease in pharmacological treatment and occult hepatitis B infection. The patient was initially treated with the R-CHOP immunochemotherapy regimen, including rituximab, cyclophosphamide, doxorubicin and vincristine, every 21 days for a total of six cycles between March 2011 and July 2011, achieving complete remission. Unfortunately, in February 2012, disease relapse occurred. Therefore, second-line immunochemotherapy with the R-DHAP regimen (rituximab, dexamethasone, cytarabine and cisplatin) was initiated in March 2012 at our institute for three cycles, along with PBSC mobilization after the second cycle. In May 2012, positron emission tomography/computed tomography (PET/CT) showed complete remission, although minimal residual activity with an uncertain significance was present in the left axillary lymph node. Because of suspected residual disease, two additional cycles of rituximab were administered, with a negative PET/CT scan in September 2012.
The patient was subsequently hospitalized at our department after signing an informed consent form for high-dose conditioning chemotherapy with the FEAM regimen (fotemustine, etoposide, cytarabine and melphalan) for 7 days, followed by autologous PBSC reinfusion in October 2012. Physical examination at admission did not show superficial lymphadenopathies or hepatosplenomegaly. On day +1, G-CSF treatment with lenograstim (263 µg) was initiated because of grade 4 neutropenia with an absolute neutrophil count (ANC) less than 500/µL. On day +6, the patient had an acute hypotensive episode in the afternoon (50/40 mmHg), lipothymia and moderate abdominal pain in the absence of tenderness, but body temperature was within the normal range. Given the lack of response to colloid polygeline intravenous fluids and hydrocortisone, an urgent complete blood cell count analysis was performed, revealing acute worsening of anemia (hemoglobin 55 mg/dL in the afternoon compared with 84 mg/dL in the morning) together with severe thrombocytopenia (6.000/µL) and neutropenia (100/µL) (Figure 1). An emergency abdominal CT scan with contrast demonstrated a deformed splenic lodge with the presence of hyperdense areas from possible splenic rupture and portal bleeding, forming a noticeable collection of serohematic fluid in the abdominal cavity (Figure 2).

Blood cell count analysis following ASCT.

CT scan with contrast. (a) Coronal CT scan showing peri-splenic fluid collection (blood) and the niche of rupture (arrow) and (b) Axial CT scan showing splenic rupture.
Because of the patient’s critical clinical conditions with hypovolemic shock and subsequent blood pressure decrease (50/30 mmHg, heart rate 114 beats per minute), dopamine was started intravenously. He was alert and orientated, with a Glasgow coma scale score of 13. Furthermore, units of packed red blood cells, platelet concentrates and fresh frozen plasma were requested urgently as part of perioperative transfusion management. Upon the arrival of blood units and after informing the patient of potential life-threatening risks associated with the procedure, he was taken to the operative room for emergency open splenectomy. Blood products were transfused during the procedure, which revealed a completely shattered spleen with vascular hilar injury and more than 2 L of massive hemoperitoneum volume. Therefore, given the considerable active bleeding, an emergency splenectomy maneuver was performed with clamping of the hilum and its resection with a large endovascular stapler (Echelon; Ethicon, Raritan, NJ, USA). After great gastric curvature hemostasis was completed, a drainage tube was placed in the splenic lodge with suturing. The patient’s vital signs were stable, and he was immediately transferred to our transplantation unit because of the high risk of opportunistic infections, where he continued transfusion support, maintaining a platelet count between 70 to 100.000/µL. Lenograstim was continued until day +8 because of prompt ANC engraftment (morning of day +7 = 210/µL, afternoon of day +7 = 810/µL, morning of day +8 = 3120/µL) (Figure 1). The postoperative course was free of complications, and the patient was discharged on day +14 after the stabilization of his hemoglobin level and platelet count with low molecular weight heparin prophylaxis. After being discharged, he was regularly vaccinated against Pneumococci, Meningococci and Haemophilus influenza B.
Macroscopically, anatomic pathology analysis showed two fragments of modestly enlarged splenic parenchyma 11 × 6 × 3 cm3 and 10 × 7 × 1.5 cm3 in size. Microscopically, there were no signs of neoplastic infiltration in the parenchyma (negative CD20 and CD79a markers). However, numerous immature myeloid elements (positive myeloperoxidase) were present at the level of the red pulp with marked vascular congestion (Figure 3). The patient was in 6-year disease-free follow-up until 2018 in the absence of splenectomy-associated complications when disease relapse occurred, which was successfully treated with rituximab, bendamustine and cytarabine (R-BAC regimen), achieving complete remission once again. The reporting of this study conforms to CARE guidelines. 2 Signed informed consent was acquired for publication purposes, and all patient details have been de-identified.
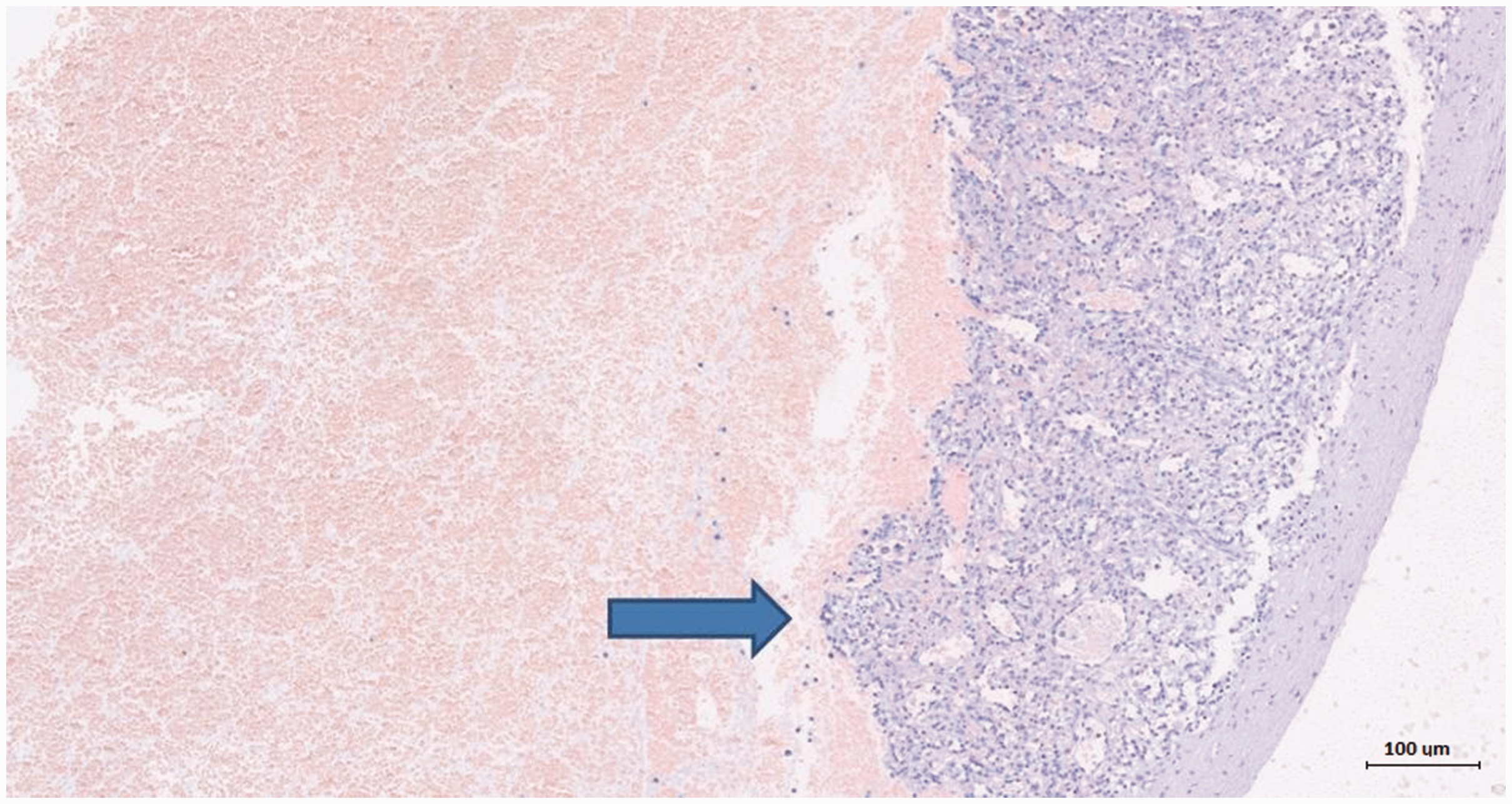
Histopathology of spleen biopsy with hematoxylin and eosin staining. The infiltration of immature myeloid elements (arrow) and marked vascular congestion of the spleen’s red pulp were observed.
Discussion
ASR represents a rare but life-threatening condition with non-specific symptoms, such as abdominal pain, marked asthenia, dizziness, confusion and shallow breathing, and in 8% of cases, the diagnosis is made only at autopsy. 3 Transient spleen enlargement during G-CSF treatment in healthy PBSC donors was described previously in two prospective trials.4,5 Furthermore, the association of G-CSF administration with the development of ASR has been reported as part of the pharmacovigilance assessment of the Food and Drug Administration adverse event reporting system 6 and in anecdotal case reports in both healthy donors and patients with cancer. 7
A review of the literature identified 27 cases of spleen rupture following G-CSF administration with comparable men/women ratios (in one case, sex was not specified) and a median age of 49 years (range 15–88 years) (Table 1). Neutropenia and mobilization were the main clinical indications of G-CSF use, with two cases of granulocyte-macrophage colony-stimulating factor use and one case of plerixafor in combination with G-CSF. Open splenectomy was the preferred treatment choice, and nearly 90% of patients survived the procedure. Table 2 summarizes the characteristics of the above-mentioned case reports.
Clinical characteristics of 27 patients with splenic rupture following G-CSF administration.
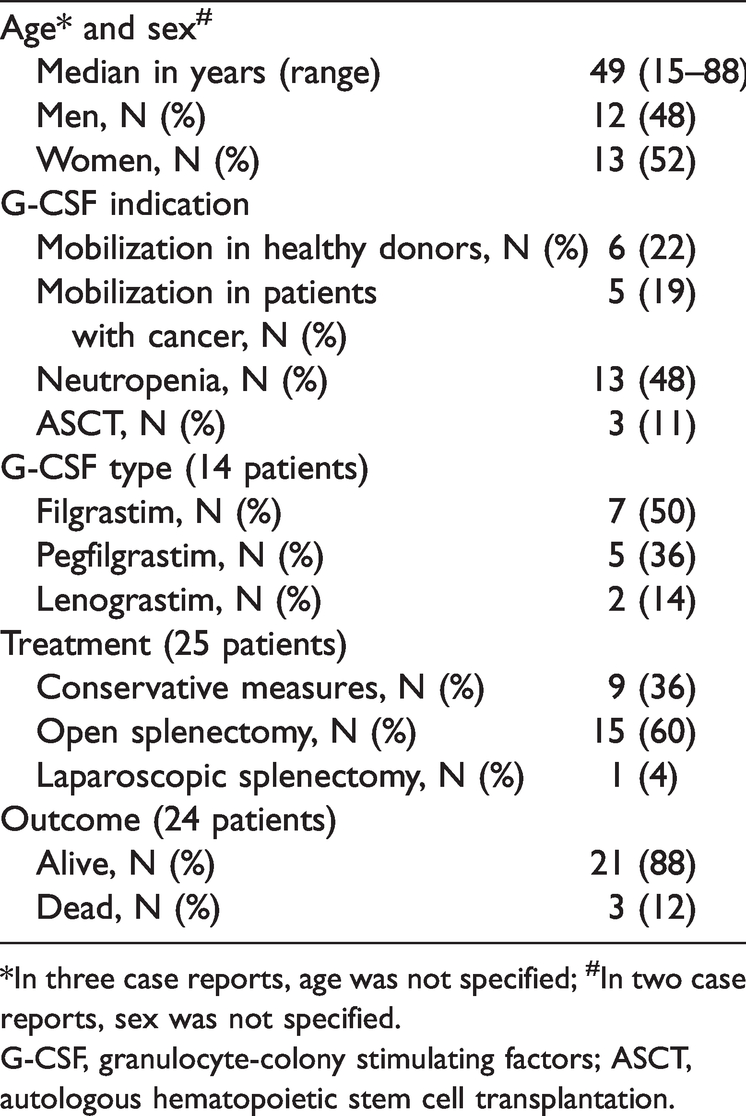
*In three case reports, age was not specified; #In two case reports, sex was not specified.
G-CSF, granulocyte-colony stimulating factors; ASCT, autologous hematopoietic stem cell transplantation.
Summary of 27 splenic rupture case reports following G-CSF administration.
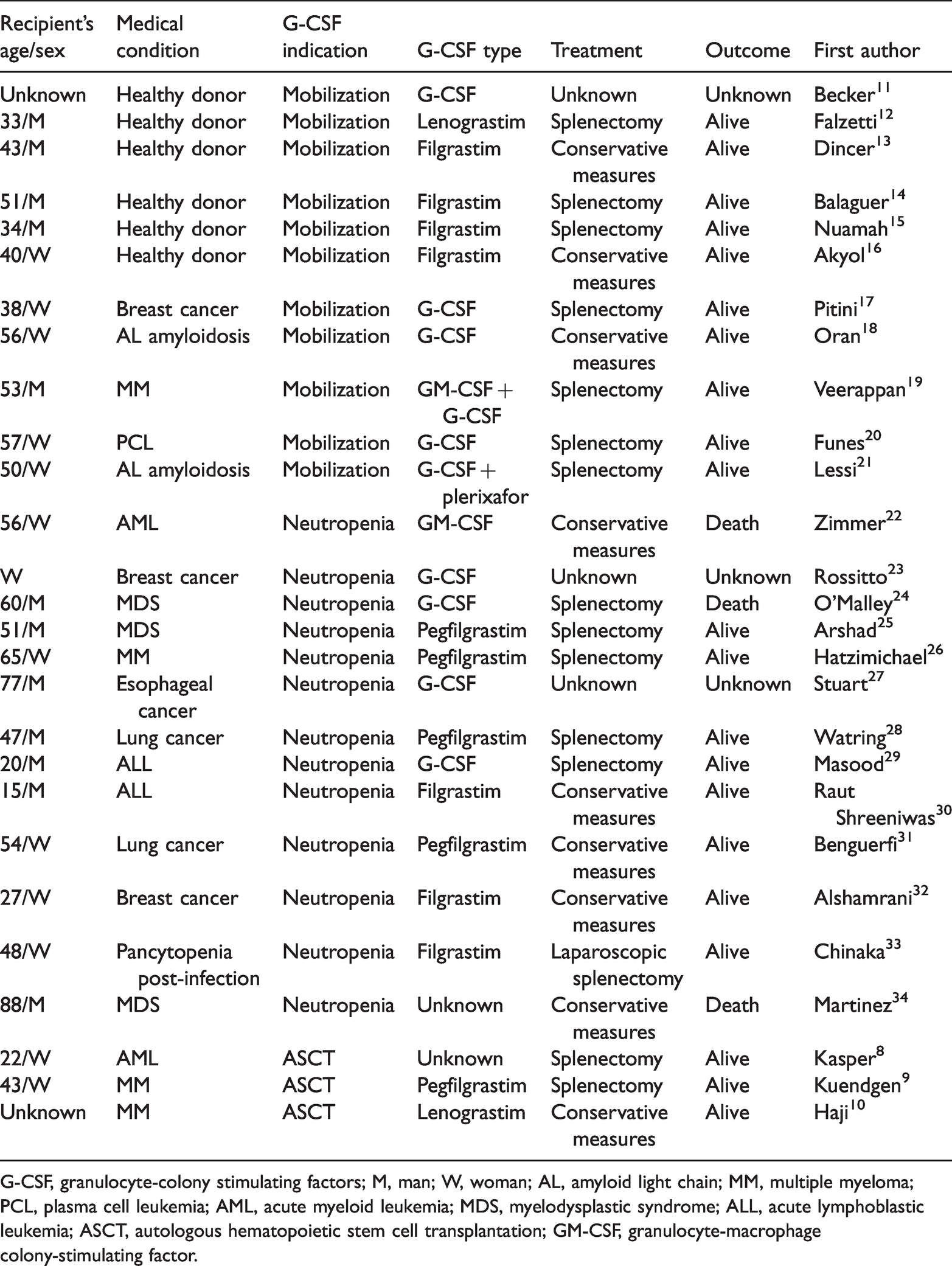
G-CSF, granulocyte-colony stimulating factors; M, man; W, woman; AL, amyloid light chain; MM, multiple myeloma; PCL, plasma cell leukemia; AML, acute myeloid leukemia; MDS, myelodysplastic syndrome; ALL, acute lymphoblastic leukemia; ASCT, autologous hematopoietic stem cell transplantation; GM-CSF, granulocyte-macrophage colony-stimulating factor.
Three cases of splenic rupture occurred following ASCT during the course of G-CSF administration. In the first case, a 22-year-old female patient with acute myeloid leukemia (AML) underwent ASCT, and on day +10, she had an episode of splenic rupture. However, the patient was not severely neutropenic or thrombocytopenic before splenectomy. 8 The second case describes a 43-year-old woman who underwent ASCT because of multiple myeloma (MM) and developed splenic rupture on day +9 during pegfilgrastim treatment. Nevertheless, the patient underwent neutrophil regeneration prior to emergency splenectomy, with grade 3 thrombocytopenia (count around 25–30.000/µL). 9 Finally, a third patient with a plasma-cell neoplasm received lenograstim following ASCT, and because of severe myelosuppression, they were treated with non-surgical transcatheter embolization of the splenic artery with success. 10
In our case, the rupture occurred on day +6 following PBSC reinfusion with severe grade 4 neutropenia and thrombocytopenia during treatment with lenograstim. The patient showed no signs of an acute abdomen, even in the presence of more than 2 L of blood in the peritoneum. The suspicion of disease relapse was based on the presence of moderate abdominal pain, a frequent symptom in patients after ASCT due to mucositis, and hypotension without significant compensatory tachycardia. Given the quantity of hemoperitoneum from portal bleeding and splenic rupture at the hilum level, emergency open splenectomy was preferred to laparoscopy and conservative measures, even though the patient had a significant risk of bleeding and infections. Furthermore, the post-operative management was not performed in the intensive-care unit to reduce the opportunistic infection risk, and the patient had no complications before being discharged.
Regarding the histopathological findings, both patients with AML and MM exhibited a normal spleen size and the expected presence of immature myeloid elements,8,9 although the spleen was not described in the third case. 10 However, in our case, modest spleen enlargement with numerous positive myeloperoxidase elements and marked vascular congestion were possible rupture-associated causes.
ASR represents a clinical challenge, especially in patients with non-specific symptoms in the absence of an acute abdomen. The role of G-CSF in ASR occurrence needs further study given its rarity, and the successful management of ASR (surgical or conservative), especially in extremely fragile patients with severe pancytopenia, needs to be optimized to further reduce the mortality rate.
Supplemental Material
sj-jpg-1-imr-10.1177_03000605221095504 - Supplemental material for Splenic rupture following lenograstim in post-autologous stem cell transplantation treated with emergency open splenectomy: a case report and literature review
Supplemental material, sj-jpg-1-imr-10.1177_03000605221095504 for Splenic rupture following lenograstim in post-autologous stem cell transplantation treated with emergency open splenectomy: a case report and literature review by Uros Markovic, Cristina Colarossi, Antonio Iuppa, Paola Scire, Ausilia Gorgone, Federica Galbo, Gabriella Amato and Gaetano Moschetti in Journal of International Medical Research
Footnotes
Author contributions
All authors made substantial contributions to the following: UM: interpreted data, drafted the final article and critically revised it. AI, CC, PS, AG, FG and GA: obtained patient consent and acquired, analyzed and interpreted the data. GM: revised the article for important intellectual content and approved the final version for submission.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethics statement
Ethical approval was not required at our institution to publish an anonymous case report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.