
Abstract
We report a 58-year-old Asian woman who was diagnosed with systemic lupus erythematosus (SLE) and lupus nephritis, together with a mixed pulmonary bacterial and fungal infection including Aspergillus. The infection did not respond well to the routine administration of anti-bacterial and anti-fungal drugs, and the patient’s creatinine levels continued to rise and protein remained in her urine. The patient’s SLE persisted without going into remission. Finally, surgical resection of the pulmonary aspergilloma brought the SLE back under control.
Keywords
Introduction
Systemic lupus erythematosus (SLE) is an autoimmune disease that affects multiple organs. SLE can lead to the development of a severe form of kidney damage known as lupus nephritis (LN). Because of the long-term use of corticosteroids and other immunosuppressants required to manage this disease, patients are more likely to be infected by pathogens. Indeed, the leading cause of death in patients with SLE was reported to be infection. 1
We report a case of SLE combined with LN, together with pulmonary mixed bacterial and fungal infection that did not respond well to the routine administration of anti-bacterial and anti-fungal drugs. This represents a rare clinical case of SLE complicated with LN and pulmonary fungal ball infection, in which proteinuria was finally brought under control after surgery. The reporting of this study conforms to the CARE guidelines. 2
Case report
We report a 58-year-old female patient hospitalized with facial erythema, oral ulcer, hair loss, and joint pain in July 2017. Physical examination revealed butterfly erythema on her face, several ulcers in her mouth, and a vasculitis-like rash on the palms of her hands and the ends of her fingers. Auxiliary examination showed the white blood cell (WBC) count to be 3.27 × 109/L, an erythrocyte sedimentation rate (ESR) of 65 mm/hour (reference range, <21 mm/hour), C-reactive protein (CRP) levels of 58 mg/dL (reference range, 0.068–8.2 mg/dL), C3 of 38 g/L, IgG levels of 17.5 g/L, positive anti-nuclear 1:1000 and anti-Smith (SM) antibodies, strongly positive anti-ribonucleoprotein (RNP), anti-Sjögren’s syndrome-related antigen A (SSA), anti-Ro-52, and anti-ribosomal P protein antibodies, normal renal function, and normal urine function. A diagnosis of SLE was made, with an SLE disease activity index (SLEDAI) score >15 points (vasculitis, 8 points; arthritis, 4 points; rash, 2 points; alopecia, 2 points; and mucosal ulcer, 2 points).
Given that SLE was in the severely active stage, we administered daily 500 mg methylprednisolone pulse therapy. However, the patient was unable to tolerate large doses of corticosteroids, showing neuropsychiatric symptoms such as mania and insomnia. We therefore administered 40-mg methylprednisolone and 0.2-g cyclophosphamide once daily. The cyclophosphamide infusion was stopped after it caused severe nausea and vomiting when used continuously for 3 days. The patient was discharged after symptoms improved with 40-mg methylprednisolone daily, and was followed up in the outpatient department.
In August 2018, the patient was admitted to hospital with cough, expectoration, fatigue, headache, and edema of both lower limbs. Auxiliary examination revealed a 24-hour urine protein content of 2.44 g, creatinine levels of 432 µmol/L, albumin levels of 29 g/L, C3 of 0.36 g/L, ESR of 55 mm/hour, CRP levels of 136 mg/dL, and bronchiectasis. Infection in the lower lobe of the left lung was observed, with a suspected sputum thrombus or aspergilloma, and bilateral pleural effusion seen on a chest computed tomography (CT; Figure 1). Filamentous fungal growth was found in bronchoalveolar lavage fluid, and renal pathology was consistent with LN (class III and V lesions). A diagnosis of SLE with LN was made, as well as bacterial and fungal pulmonary infection with an SLEDAI score >15 points (lupus headache, 8 points; arthritis, 4 points; pleurisy, 4 points; proteinuria, 4 points; and skin rash, 2 points). Because SLE was in the severely active stage, methylprednisolone pulse therapy would ideally have been performed, but the patient could not tolerate large doses of corticosteroids and was suffering from pulmonary fungal infection, so was instead given an intravenous infusion of 40-mg methylprednisolone once daily and hydroxychloroquine 200 mg twice a day as immunomodulatory therapy, as well as voriconazole for the infection. After 2 weeks of anti-infective treatment, ESR and CRP levels were normal, C3 was 0.54 g/L, serum creatinine levels were 123 µmol/L, the 24-hour urine protein content was 0.59 g, the pulmonary infection was controlled, and the renal function was gradually recovering. The patient was discharged from hospital after stabilization with a discharge treatment plan to continue taking oral itraconazole as well as the immunomodulators prednisone (40 mg, once daily), hydroxychloroquine, and mycophenolate (0.75 g, twice a day).
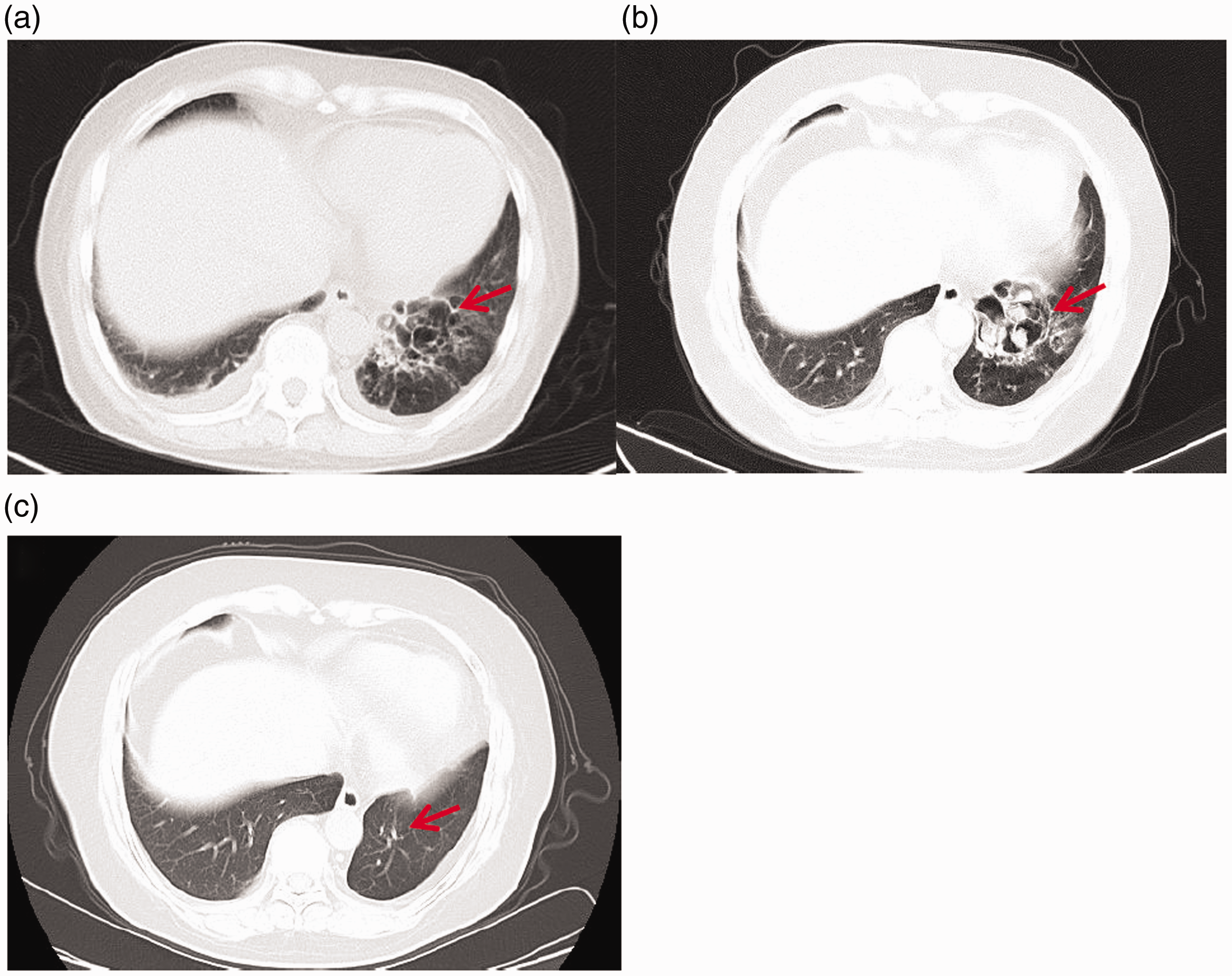
Chest CT findings. (a) Aspergilloma was suspected in the lower lobe of the left lung in August 2018. (b) A nodule in the left lower lobe of the lung was thought to be a fungus ball in October 2020. (c) Post-surgery in January 2021. Red arrow shows lung lesions and pulmonary manifestations after resection.
From December 2018 to December 2019, the patient did not regularly take itraconazole anti-fungal therapy or prednisone and mycophenolate immunomodulatory therapy.
In October 2020, the patient was hospitalized again with general fatigue and joint pain. Her WBC count was 11 × 109/L, with a neutrophil percentage of 0.82%, a 24-hour urinary protein content of 1.1 g, creatinine levels of 126 µmol/L, albumin levels of 38.2 g/L, and C3 of 0.45 g/L. The beta-D-glucan fungal antigen test and sputum loop-mediated isothermal amplification assay were negative. Anti-nuclear 1:1000, anti-SM, and anti-RNP antibody levels were weakly positive, and anti-SSA and anti-Ro-52 antibody levels were strongly positive. Sputum culture showed Aspergillus fumigatus, and re-examination of the chest CT showed possible bronchiectasis and infection in the lower lobe of the left lung, an intraluminal nodule, possible fungus ball, and a sputum thrombus, and was awaiting the exclusion of possible new organisms (Figure 2). A diagnosis of SLE with LN was made, with a bacterial and fungal pulmonary infection with an SLEDAI score of 12 points (arthritis, 4 points; pleurisy, 4 points; and proteinuria, 4 points).
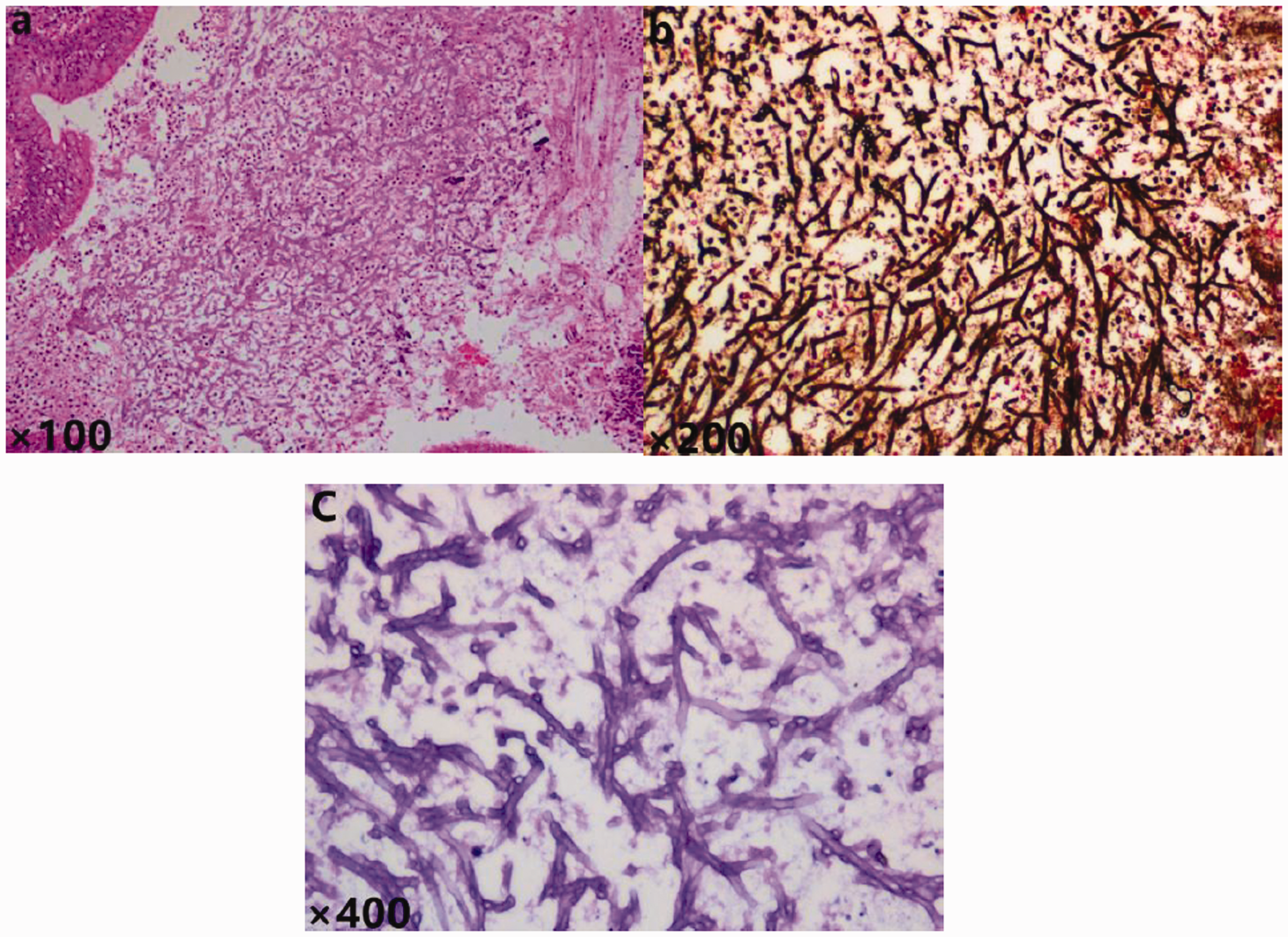
Lung histopathology findings. (a) HE staining of lung tissue (magnification ×25). Multiple fungal hyphae and spores were found in the bronchioles. (b) Hexamine silver staining of lung tissue (magnification ×200). Fungal hyphae and spore are stained dark brown, and hyphae show acute branching. (c) PAS staining of lung tissue (magnification ×400). Fungal hyphae are divided into two parts.
Because SLE was in the moderately active stage, we continued with 5-mg prednisone once daily and 0.75-g mycophenolate immunomodulatory therapy once daily. We usually consult with the thoracic surgery department, respiratory department, and imaging department about the possibility of lung disease deriving from a fungus ball. However, the patient’s general condition was poor and she was not fit for surgery. There were no guidelines for performing emergency surgery, such as for massive hemoptysis, so our department was advised to continue treating the fungus. Considering that the fungus was an intracapsular ball, the patient’s blood supply was poor, anti-fungal drugs could not effectively reach the lesion and thus had limited effectiveness, LN caused proteinuria, and the patient had a poor response to previous treatment, we suggested surgical removal of the fungal ball after consultation with the patient.
After receiving informed consent of the patient, she underwent lobectomy of the lower left lobe under general anesthesia on November 12, 2020. The postoperative pathological result was pulmonary aspergillosis (Figure 2). To reduce the risk of infection, mycophenolate was stopped on the day of surgery and 2 weeks after the operation, and prednisone was reduced to 5 mg daily. Voriconazole anti-fungal therapy was continued post-surgery. C3 was re-examined after 2 weeks, showing an increase from 0.45 g/L to 0.78 g/L; serum creatinine levels decreased from 126 µmol/L to 108 µmol/L, the 24-hour urinary protein content decreased from 1.1 g to 0.59 g, and there was a gradual improvement in renal function and control of LN. In January 2021, a follow-up chest CT showed that lung lesions were greatly reduced, and fatigue symptoms had also greatly improved.
Discussion
SLE is a diffuse connective tissue disease that affects many systems and organs, including the kidney. The proportion of patients with SLE in China was previously reported to be 47.4%. 3 Patients with SLE require the long-term use of corticosteroids and/or immunosuppressants, resulting in a greatly increased rate of serious infections, 4 which is one of the main causes of death. Indeed, 20% to 55% of patients with SLE who died were found to carry an infection, 5 and infection was shown to be the most common cause of death of patients with SLE in China. 6 Therefore, active control of infection is an important measure of controlling the progression of SLE and delaying renal damage.
The present case had many predisposing factors leading to infection. First, connective tissue disease itself is associated with immune dysfunction, leading to affected patients becoming more easily infected. Second, the long-term use of corticosteroids and immunosuppressants increases the likelihood of infection. Third, patients showing poor adherence to medical instructions and irregular dosing of medication are less able to alleviate long-term SLE and LN, increasing their risk of infection. Fourth, patients diagnosed with SLE and LN who experience repeated bacterial infection and are repeatedly administered broad-spectrum antibiotic treatment are more prone to opportunistic infection, particularly fungal infection. The mortality rate of invasive fungal disease is high,7,8 so the prognosis of patients with SLE carrying fungal infections is worse than that of the general SLE population.9,10 Furthermore, the prognosis of patients with LN complicated with fungal infection is also worse than that of the general LN population, with higher mortality. 11
Since being diagnosed with SLE, our patient’s clinical manifestations and laboratory indicators have been evaluated using the SLEDAI scoring system (Table 1). Her disease has been moderately to severely active, and proteinuria was not effectively controlled. Studies have confirmed an independent relationship between the level of proteinuria and the histological severity of renal damage in patients with LN, 12 so the level of proteinuria is an effective index for the detection and control of LN. Additionally, SLE itself can lead to the development of cell-mediated immune disorders, resulting in increased vulnerability to invasive fungal infection.
SLE disease activity score (SLEDAIP).
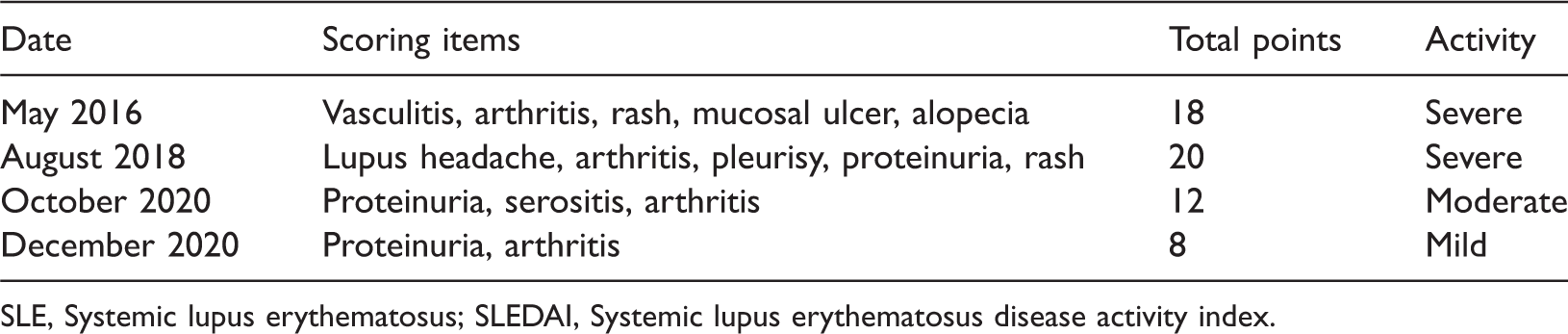
SLE, Systemic lupus erythematosus; SLEDAI, Systemic lupus erythematosus disease activity index.
Both T cells and B cells play critical roles in defense against fungal infection, and CD4+ T cells isolated from lupus-prone mice displayed immune disability in defense against intracellular infection. 13 Comprehensive analysis of the relationship between patients with long-term lupus proteinuria not in remission and pulmonary Aspergillus infection showed that ineffectively controlled fungal infection aggravates kidney damage. 8
Since December 2018, the sputum culture of our patient showed filamentous fungal growth. This finding combined with chest CT imaging led to the consideration of pulmonary aspergillosis, so she was administered the long-term successive treatment of anti-fungal drugs nystatin, voriconazole, and itraconazole. However, this was not effective, and follow-up chest CT showed no reduction in the size of the lesions. This is because the pulmonary fungus was an intracapsular ball with a poor blood supply, so the anti-fungal drugs could not reach their target effectively.
Current treatment options for LN complicated with fungal infection include systemic or local anti-fungal drugs, surgical resection, or conservative treatment, which all require long-term follow-up. 14 Patients with asymptomatic aspergillosis generally do not need special treatment such as surgery if they lack hemoptysis.14,15 For localized pulmonary fungal infection with a definite location, surgical treatment can be considered when drugs are ineffective. 16 Although our patient was of an advanced age, had more basic diseases, and a high surgical risk, surgery was nevertheless strongly recommended to remove the lesions because her SLE had persisted long-term without remission (continuous proteinuria) and because of its association with fungal infection. Pulmonary aspergillosis was confirmed by pathology after operation, and itraconazole anti-fungal therapy was continued post-surgery. After 2 weeks, her 24-hour urine protein had greatly decreased to 0.59 g, complement C3 was greatly increased, lupus activity had decreased from moderate to mild activity, renal function was gradually recovering, and LN was effectively brought under control.
Conclusion
For patients with poorly controlled lupus, we suggest actively searching for the focal point of infection, with particular emphasis on potential foci such as cholecystitis, gingivitis, appendicitis, vaginitis, and skin infection. Because the inflammatory response to infection can increase the severity of the condition, bringing this under control is important. Surgery should be considered in patients with lupus and aspergilloma to remove the lesions and help keep the lupus under control.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221095224 - Supplemental material for Surgical resection of lupus nephritis with pulmonary Aspergillus infection: a case report and review of the literature
Supplemental material, sj-pdf-1-imr-10.1177_03000605221095224 for Surgical resection of lupus nephritis with pulmonary Aspergillus infection: a case report and review of the literature by Xiaoli Pan, Yuan Yuan, Yu Tian, Jinjing Wang, Yida Li and Mei Tian in Journal of International Medical Research
Footnotes
Statement of ethics
The patient provided informed written consent for participation in the study, and its publication. The study protocol was approved by the Medical Ethics Committee of Affiliated Hospital of Zunyi Medical University.
Declaration of conflicting interest
All authors declare that there is no conflict of interest.
Funding
This study received financial support from the National Natural Science Foundation of China (81860297).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.