
Abstract
Patients with pancreatic walled-off necrosis (WON) treated by minimally invasive approaches often require repeated necrosectomy instead of conventional open necrosectomy. A 55-year-old woman with lateral infected pancreatic WON was successfully treated by an infrequently used technique involving an ultrasonic pneumatic lithotripsy system (UPLS) and double-catheter aspirated lavage through a percutaneous drainage tract. No perioperative complications occurred. The mean operating time of the repeated procedures was 35 minutes (range, 25–48 minutes). The total hospitalization stay was 46 days, and no recurrence of the fluid collection was observed during the 15-month follow-up period. UPLS-assisted necrosectomy and double-catheter aspirated lavage is an alternative technique for lateral WON that fails to improve by percutaneous drainage. It efficiently combines disintegration and aspiration procedures and can be safely repeated under total intravenous anesthesia through sinus tracts.
Keywords
Introduction
Patients with acute pancreatitis (AP) often develop accumulated peripancreatic fluid collections and even symptomatic or infected walled-off necrosis (WON), 1,2 resulting in a poor prognosis, high incidence of complications, and increasing mortality rate. The step-up approach is often recommended as the first-line strategy for the treatment of symptomatic or infected pancreatic necrosis (IPN). 3 –5 Although minimally invasive approaches (MIAs) have resulted in less invasion and fewer complications, high efficiency and safety remain basic requirements particularly in complex cases, and repeated procedures are often required.
In this report, we describe our performance of an infrequently utilized technique involving an ultrasonic pneumatic lithotripsy system (UPLS) for treatment of WON through a percutaneous drainage tract, followed by double-catheter aspirated lavage after necrosectomy. The UPLS can dissolve necrotic tissue for easy absorption without damaging blood vessels, and the procedure can be repeated under total intravenous anesthesia (TIVA) through the sinus tract for patients with the appropriate indications. To the best of our knowledge, few reports have described the use of this technique for WON.
Case presentation
A 55-year-old woman with AP presented to our emergency department on 25 April 2020 with a 3-day history of acute upper abdominal pain, nausea, and mild fever. She had a medical history of biliary stones but no history of alcoholism, hyperlipidemia, or surgery. Computed tomography (CT) and laboratory results suggested AP in a local hospital; no therapy was administered before she presented to our hospital.
Physical examination revealed an increased heart rate, abdominal distention, and upper abdominal tenderness without resistance. Laboratory results showed an elevated serum amylase concentration of 1850 U/L (reference range, 0–100 U/L) and urine amylase concentration of 5180 U/L (reference range, 0–500 U/L), a reduced serum calcium concentration of 1.51 mmol/L (reference range, 2.0–2.6 mmol/L), an elevated white blood cell count of 16.9 ×109/L (reference range, 3.5–9.5 × 109/L), and a normal hemoglobin concentration of 124 g/L (reference range, 115–150 g/L). CT showed a peripancreatic fluid collection (Figure 1(a)). Moderately severe AP was confirmed according to the 2012 revised Atlanta classification. 6 Intensive care, fluid resuscitation, antibiotics, and left-sided retroperitoneal percutaneous catheter drainage (2 weeks after the onset of AP) were performed in accordance with the guidelines on the management of AP. About 3 weeks after the initial treatment, the patient developed a persistent fever and showed gas in the collections on CT, and Escherichia coli was isolated from a culture of the drainage fluid. According to the 2013 IAP/APA 7 and 2018 ESGE 8 evidence-based guidelines, further intervention was required to treat the IPN, which had a poor prognosis.

Pancreatic computed tomography before and after necrosectomy. (a) Peripancreatic fluid collections before necrosectomy (axial view) and (b) Reduction of peripancreatic fluid collections after necrosectomy (axial view).
The following innovative retroperitoneal approach was used. Four weeks after the onset of AP, necrosectomy was performed using an EMS-III (LithoClast®) UPLS (EMS – Electro Medical Systems, Nyon, Switzerland) (Figure 2(a)) through sinus tract nephroscopy. The system consists of a LithoClast® Master (device that combines pneumatic and ultrasound lithotripsy) and an ultrasound handpiece (Figure 2(b)). It can drive energy generated by compressed gas. In the present case, this device was combined with a suction system that can aspirate pus and fragments of necrotic tissue. The whole procedure was completed under a video monitor. Warm normal saline solution was infused into the operation area, and the necrosis attached to the wall of the cavity was then extracted by gently pulling the tissue with nephroscopic forceps; the necrosis left free in the cavity was fragmented and aspirated by the UPLS (Figure 3(a)). A large-bore drainage tube composed of a double catheter was placed in the cavity until the free necrotic fragments were cleared (Figure 3(b)), with continuous negative-pressure lavage by warm normal saline at a rate of 100 to 125 mL/h after surgery. The same procedure was repeated twice through the drainage tract at an interval of 5 to 7 days until the abscess cavity collapsed (Figure 1(b)) and the patient’s clinical condition improved. The repeated procedures were performed under TIVA, and the mean operation time was 35 minutes (range, 25–48 minutes). Lavage was continued until the drainage fluid turned clear. The tube was gradually pulled out until the output was less than 20 mL/day and was then withdrawn. No intraoperative or postoperative surgery-related complications occurred. The duration of hospitalization was 46 days, after which the patient was discharged home and satisfied with her outcome. No recurrence was observed during the 15-month follow-up period. The patient’s detailed information and treatment data are shown in Table 1. The reporting of this case conforms to the CARE guidelines. 9
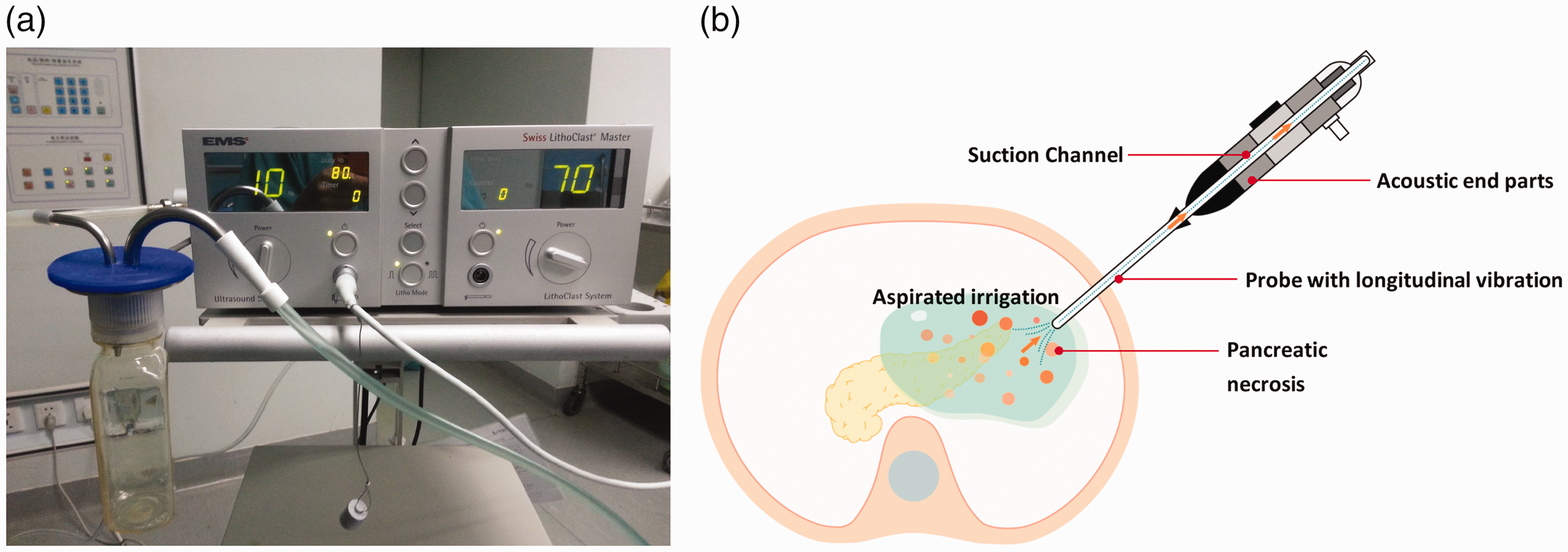
Ultrasonic pneumatic lithotripsy system and working principle. (a) Ultrasonic pneumatic lithotripsy system and (b) Working principle of ultrasound handpiece.

Pancreatic necrosectomy using ultrasonic pneumatic lithotripsy system. (a) Ultrasonic pneumatic lithotripsy system-assisted necrosectomy and (b) Clearance of free necrosis after necrosectomy.
Patient information and treatment.

PCD, percutaneous catheter drainage; UPLS, ultrasonic pneumatic lithotripsy system.
Discussion
During the past two decades, cases of IPN treated by alternative MIAs have not usually required conventional open necrosectomy. 4 –8, 10 Common MIAs include percutaneous radiological drainage, a transgastric approach, a transperitoneal approach, and a retroperitoneal approach. 11 –13 Retroperitoneal necrosectomy is an approach that has risen to favor in this regard, especially for patients with lateral necrosis. However, because this technique is limited by the bore size of the sinus tract and the size of the forceps, repeated debridement is required in complex cases until clinical success is reached. Thus, repeated surgical invasion and the operating time should be strictly controlled to avoid operation-related complications such as bleeding, perforation, and respiratory insufficiency.
In this case, the fluid collection was mainly located around the distal pancreas, and the distance between the WON and posterior gastric wall was more than 1 cm; therefore, we considered performing a left-sided retroperitoneal procedure instead of an endoscopic approach. In the regular nephroscopic procedure, the necrotic tissues are pulled and removed repeatedly by forceps; however, only one piece of necrotic tissue can be extracted each time, lengthening the procedure time and requiring great patience by the operator. We instead use an UPLS for easier debridement and aspiration. Ultrasound energy driven by the UPLS can emulsify and dissolve large and solid necrosis into fragments. This system produces little heat, and the amplitude before and after impact is less than 2 mm. The mucosa sustains only slight transient injury, and the blood vessels are clearly visible, helping to avoid major hemorrhage. Moreover, we combine this device with a suction system that can automatically aspirate pus and necrotic fragments. Repeated procedures under TIVA can also reduce the risk of respiratory insufficiency compared with general anesthesia. In addition, oral intake and out-of-bed activities can be resumed on the day of surgery.
This report has illustrated that use of an UPLS is an alternative treatment method for lateral WON that fails to improve by percutaneous drainage. To the best of our knowledge, use of an UPLS combined with double-catheter aspirated lavage has rarely been reported to date, and it is an innovative procedure compared with regular nephroscopic necrosectomy. It combines disintegration and aspiration procedures for efficient necrosectomy, and it can be safely repeated under TIVA through sinus tracts. However, because this was a case report, we cannot draw any conclusions regarding its superiority to open surgery, endoscopic necrosectomy, or other retroperitoneal necrosectomy approaches. Details and standards of the technique require further evaluation.
Footnotes
Ethics statement
All procedures were performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This case was approved for publication by the Ethics Committee of Hangzhou First People’s Hospital (2020-009-01). Written informed consent was obtained from the patient to publish this case report. The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient provided her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published and that due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Author contributions
Dr. Bei Lu, Dr. Junjie Yin, Dr. Jingrui Wang, Dr. Yang Cai, and Dr. Xiao Xu were involved in compilation of the data and drafting of the article. All authors have read and approved the final manuscript. Dr Yang Cai and Dr Xiao Xu contributed equally to this work and should be considered co-corresponding authors.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.