
Abstract
Objective
The characteristic features, including blood test data, of the novel coronavirus disease 2019 (COVID-19) versus influenza have not been defined. We therefore compared the clinical parameters, including blood test data, of COVID-19 and influenza.
Methods
This retrospective cross-sectional survey was conducted at Juntendo University Nerima Hospital. We recruited patients diagnosed with COVID-19 between 1 January 2020 and 31 December 2020 who underwent blood tests. For comparison, we recruited an equivalent number of patients who were diagnosed with influenza and who underwent blood tests.
Results
During the study period, 228 patients (male:female, 123 [54.0%]:105 [46.0%]; age, 54.68 ± 18.98 years) were diagnosed with COVID-19. We also recruited 228 patients with influenza (male:female, 129 [56.6%]:99 [43.4%]; age, 69.6 ± 21.25 years). An age of 15 to 70 years (vs. 71 years), breathing difficulty, and malaise were significantly more common in patients with COVID-19 than in those with influenza. However, nausea, body temperature >38.1°C, and white blood cell count >9000/μL were more common in patients with influenza.
Conclusions
Our results are useful for differentiating COVID-19 from influenza, and these findings will be extremely helpful for future practice as we learn to coexist with COVID-19.
Keywords
Introduction
In December 2019, a series of pneumonia cases of unknown etiology featuring clinical presentations that greatly resembled those of viral pneumonia were reported.1–3 The novel coronavirus disease (COVID-19) pandemic poses a great threat to human life. Many case reports on the similarities between COVID-19 and influenza have been published,4–7 but the disease presentation continues to vary among individuals. Symptoms that differ from those observed in past viral infections have also been reported. For example, there are reports of patients presenting with substantial loss of smell and taste.8,9 The wide range of reported features is believed to reflect effects on non-respiratory systems, and they indicate that signs may be observed in infected patients who lack apparent respiratory symptoms. 10
Before 2019, influenza was a common infectious disease causing fever, especially in seasonal epidemics. However, it is difficult to discriminate influenza from COVID-19 because more emphasis is being placed on diagnosing the latter condition. Some studies directly compared the burden of COVID-19 and influenza individually.11–14 In a previous study, anosmia (53% vs. 17%, P < 0.001), dysgeusia (49% vs. 20%, P =0.001), diarrhea (40% vs. 20%, P = 0.021), frontal headache (26% vs. 9%, P = 0.021), and bilateral crackling sounds (24% vs. 9%, P = 0.034) were significantly more common in patients with COVID-19 than in those with influenza. However, sputum production (52% vs. 29%, P = 0.010), dyspnea (59% vs. 34%, P = 0.007), sore throat (44% vs. 20%, P = 0.006), conjunctival hyperemia (30% vs. 4%, P < 0.001), tearing (24% vs. 6%, P = 0.004), vomiting (22% vs. 3%, P = 0.001), and rhonchi sounds (17% vs. 1%, P = 0.002) occurred more frequently in patients with influenza than in those with COVID-19. 13 However, no studies to date have compared COVID-19 and influenza using blood test data. In a previous study, an elevated red blood cell distribution width (RDW) at the time of hospital admission and an increased RDW during hospitalization were associated with an increased risk of mortality in patients with COVID-19. 15 In another study, the fibrinogen-to-albumin ratio and platelet count were independent risk factors for severe illness. 16 Thus, COVID-19 may be diagnosed according to clinical symptoms as well as blood test data, and a comparison of COVID-19 and influenza using blood test data is believed to have clinical significance. In cases of suspected influenza, a physical examination is performed to examine characteristic features such as influenza follicles;17,18 however, since the COVID-19 outbreak, physical examinations are often omitted. Therefore, this cross-sectional study aimed to identify the characteristics of COVID-19 versus influenza using blood test data to aid in their discrimination.
Materials and methods
Study design and study population
We recruited patients diagnosed with COVID-19 between 1 January 2020 and 31 December 2020 who underwent blood tests. For comparison, we recruited an equal number of patients diagnosed with influenza who also underwent blood tests between 11 January 2015 and 31 December 2020. Children (age < 14 years) with COVID-19 or influenza were excluded. COVID-19 was diagnosed using polymerase chain reaction for the detection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) nucleic acids, whereas influenza was diagnosed using a rapid influenza diagnostic kit (Quick navi -Flu2; Otsuka Pharmaceutical, Tokyo, Japan). Furthermore, more than two doctors were involved in each diagnosis. This retrospective cross-sectional study was performed at Juntendo University Nerima Hospital, a 400-bed university-affiliated hospital in Tokyo, Japan. The clinical information extracted by chart review was as follows: demographic factors, underlying conditions, symptoms, vital signs, and laboratory data.
Statistical analysis
Bivariate comparisons of each variable between COVID-19 and influenza were performed using an independent-samples t-test for continuous data or the chi-square test for categorical data. Differences were considered statistically significant at P < 0.05. Significant variables in the bivariate analysis were subjected to multivariate logistic regression analysis. The accuracy of the multivariate logistic regression models was assessed using the area under the of the receiver operating characteristic curve (AUC). All statistical analyses were performed using EZR (Saitama Medical Center; Jichi Medical University, Saitama, Japan), a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). EZR is a modified version of R Commander designed to add statistical functions that are frequently used in biostatistics. 19
This retrospective study was conducted in accordance with relevant guidelines and regulations and received approval from the ethics committee of Juntendo University Nerima Hospital, Tokyo, Japan (approval number: 2020066). Because of the retrospective study design, the requirement for written or verbal informed consent was waived by the ethics committee. The reporting of this study conforms to the STROBE guidelines. 20
Results
During the study period, 228 patients (male:female, 123 [54.0%]:105 [46.0%]; age, 54.68 ± 18.98) were diagnosed with COVID-19. None of the patients had a history of vaccination for COVID-19 before SARS-CoV-2 infection. Meanwhile, 228 patients with influenza (male:female, 129 [56.6%]:99 [43.4%]; age, 69.6 ± 21.25) were also recruited. All influenza patients were classified as having type A disease. As presented in Table 1, 456 patients (male:female, 252 [55.3%]:204 [44.7%]; age, 62.12 ± 21.47 years) were included in this study. Table 1 also presents the characteristics of the patients with COVID-19 versus those with influenza and the results of bivariate analysis (Table 1).
Patient variables and univariate analysis results.
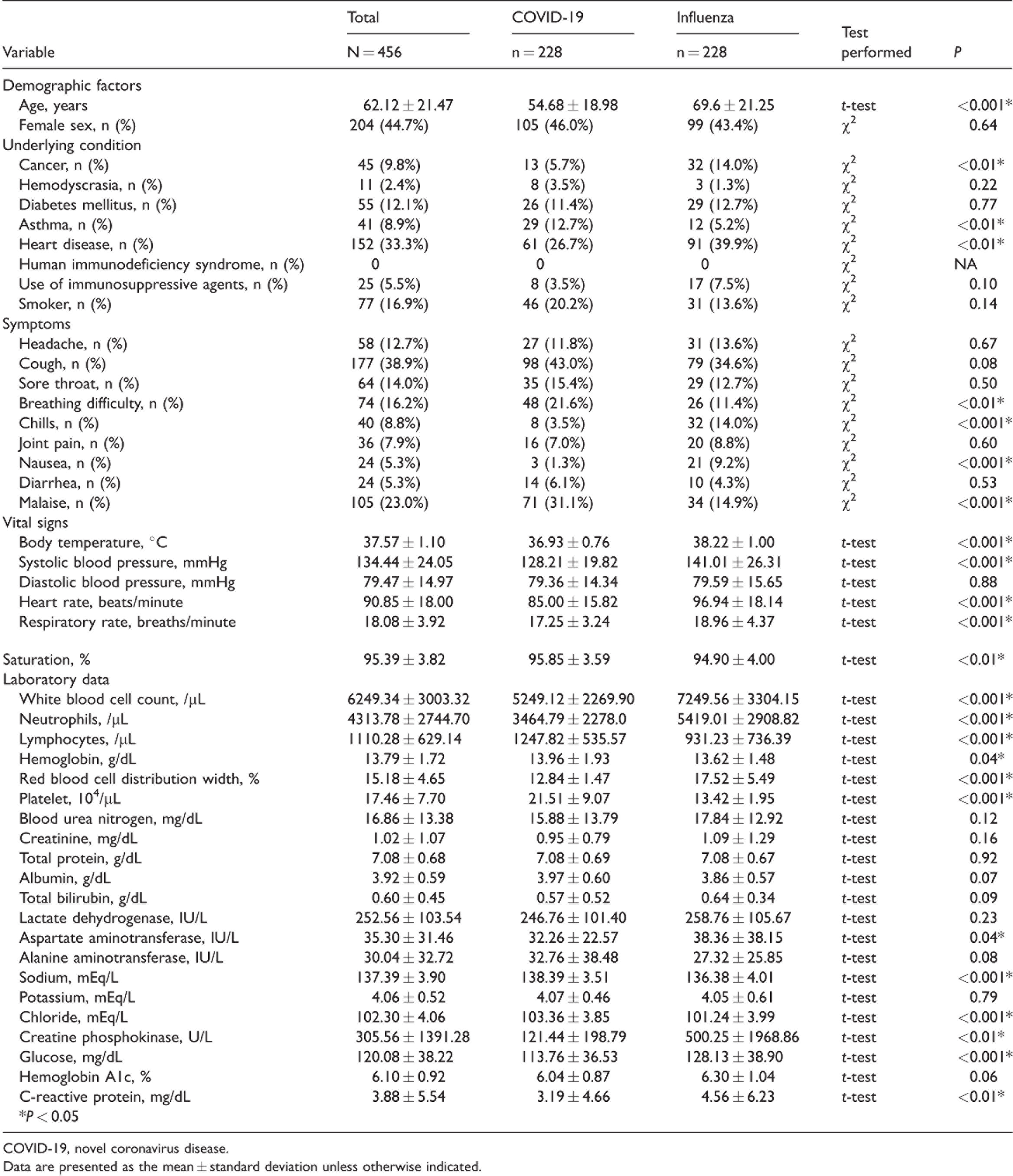
COVID-19, novel coronavirus disease.
Data are presented as the mean ± standard deviation unless otherwise indicated.
We conducted multivariate logistic regression analysis based on the results of bivariate analysis (Table 2). We incorporated factors considered clinically useful. We excluded factors with a significant difference over the normal range, even if it was significantly different. Based on the cutoff value, body temperature was categorized as hypothermia (<35.9°C) or hyperthermia (>38.1°C), and a body temperature of 36 to 38°C was used as the reference range. Furthermore, the cutoff white blood cell (WBC) count was >9000/μL, which was higher than the normal upper limit. The cutoff for the lymphocyte count was >1800/μL (20% of the cutoff [>9000/μL] for the WBC count), and that for the creatine phosphokinase level was >300 U/L. Because the percentages of neutrophils and lymphocytes were highly correlated with each other, the percentage of lymphocytes was used in the multivariate analysis as a representative. The significant factors in the multivariate analysis were an age of 15 to 70 years (vs. 71 years; odds ratio [OR] = 7.11; 95% confidence interval [CI] = 3.97–12.70; P < 0.001), breathing difficulty (OR = 3.33; 95% CI = 0.18–2.16; P < 0.01), nausea (OR = 0.92; 95% CI = 0.02–0.43; P < 0.01), malaise (OR =2.21; 95% CI = 1.09–4.48; P = 0.03), body temperature >38.1°C (OR = 0.04; 95% CI = 0.02–0.09; P < 0.001), and WBC count >9000/μL (OR = 0.07; 95% CI = 0.02–0.24; P < 0.001). We evaluated the quality of this multivariate logistic regression model using the AUC, which was 0.91 (95% CI = 0.88–0.94). Thus, the model used in this study had sufficient power.
Multivariate logistic regression model.

*P < 0.05CI, confidence interval; OR, odds ratio.
Discussion
To the best of our knowledge, this is the first study to directly compare patients with COVID-19 and those with influenza using laboratory test data collected from a university hospital. An age of 15 to 70 years (vs. 71 years), breathing difficulty, and malaise were significantly more common in patients with COVID-19 than in those with influenza. However, nausea, body temperature >38.1°C, and WBC count >9000/μL were significantly more common in patients with influenza than in those with COVID-19.
Other studies reported that the age at the onset of COVID-19 is lower than that at the onset of influenza.14,21 The results of these studies support the results of the present study. In Japan, many patients with COVID-19 are hospitalized to control the disease’s spread, even if they are young and asymptomatic. Patients with COVID-19 are usually treated at the hospital, where their blood samples can be tested; however, young patients with influenza do not require hospitalization, and they remain at home, which hinders blood testing.
SARS-CoV-2 mainly invades respiratory epithelial cells by adhering to angiotensin-converting enzyme 2; thus, infected patients may develop mild-to-severe inflammatory responses and acute lung injury. 22 Another study reported that COVID-19 causes acute respiratory failure because of the predominance of influenza. 14 These studies support the results of our study, revealing a higher number of cases of dyspnea in COVID-19 than in influenza.
Similarly, malaise has been reported in many patients with COVID-19. 14 In a previous study, 63% of patients with COVID-19 had malaise. 23 These findings support the results of our study, in which the prevalence of malaise was higher in patients with COVID-19 than in those with influenza. Malaise may be related to an increased viral load and an immune response to infection. 24 In addition, insufficient energy production to meet the required metabolic demands is related to malaise. 25
In our study, a WBC count exceeding 9000/μL was more frequently associated with influenza than with COVID-19, a finding supported by the results of another study. 26 Regarding the differential WBC count, one meta-analysis detected lymphopenia in 62.5% of patients in COVID-19 (95% CI = 45–72; P < 0.001), which was higher than the rate of 49% in patients with influenza type A (95% CI = 35–56.4; P < 0.001). 27 Another study also reported low lymphocyte counts in patients with COVID-19. 28 Our study did not find significant lymphopenia, but the WBC count may be useful for differentiating COVID-19 from influenza.
Our study also revealed that CRP levels are not useful for differentiating COVID-19 from influenza. Similarly, a previous study reported that the CRP level was not an effective discriminator of COVID-19 and non-COVID-19. 29 However, CRP levels were significantly higher in the severe COVID-19 group than in the non-COVID-19 group, which confirms the findings of previous studies regarding the clinical utility of the CRP level as an indicator of severe disease and progressive inflammation.30,31 In our study, no significant difference in CRP levels was observed because none of the patients with COVID-19 had severe disease. In contrast to the results of a previous meta-analysis, 32 a recent meta-analysis revealed that procalcitonin levels were not significantly different between the severe and non-severe groups. Procalcitonin levels were assessed in only a few cases in this study; therefore, we did not add this as an extraction item. However, we believe that procalcitonin levels may have value for discriminating COVID-19 and influenza in the future.
Body temperature >38.1°C was a more frequent characteristic of patients with influenza than of those with COVID-19. Many cases of COVID-19 that do not involve fever have been reported.33,34 We believe that these findings are consistent with our results. However, this may have occurred because patients receiving antipyretics could not be excluded. Furthermore, many patients with COVID-19 had to be hospitalized for isolation for infection control, and they underwent laboratory tests even when they were asymptomatic.
Nausea is more frequently associated with influenza than with COVID-19. In one study, nausea occurred in approximately 3.9% of patients with COVID-19. 33 Similarly, the prevalence of nausea is unknown, but influenza can cause digestive symptoms. The mechanism underlying nausea is unclear and requires further investigation. Inflammatory reactions may occur when a virus infects gastrointestinal mucosal bleeding cells, and digestive symptoms such as nausea are believed to occur during these reactions. In this study, the significantly lower rate of nausea in patients with COVID-19 may reflect its greater effect on the respiratory tract than on the gastrointestinal tract. Breathing difficulty was significantly more common in patients with COVID-19 than in those with influenza, which may support our hypothesis.
Influenza and coinfection by COVID-19 should also be discussed. According to the World Health Organization influenza surveillance report, the incidence of influenza after the COVID-19 outbreak decreased sharply globally as well as in Japan. It appears that many people were practicing infection prophylaxis for COVID-19 (wearing masks and washing hands), which reduced the number of patients with influenza. Because influenza is transmitted by droplets or aerosol and contact similarly as COVID-19, it is inferred that measures against COVID-19 also protect against influenza. Furthermore, it is believed that the reduction in cross-country travel also contributed to decrease the number of patients with influenza. Coinfected patients were not observed in this study, but the incidence of coinfection may increase in the future. Animal experiments revealed that coinfection exacerbates pneumonia. 35 A discussion of this topic in the future is necessary.
This study had some limitations. First, it is possible that patients with COVID-19 were hospitalized more frequently as required by the law in Japan. Many patients with COVID-19, even young and asymptomatic patients, are hospitalized for isolation purposes to help control the spread of this highly infectious disease. Furthermore, an influenza extraction period of several years was chosen (from 11 January 2015 to 31 December 2020). Annually, the symptoms of seasonal flu can vary, and this effect may have influenced the study’s results. However, the influenza type did not influence the results, as no patients with influenza type B underwent blood tests.
In addition, influenza vaccine history was difficult to obtain from a chart review. Thus, we were unable to examine the effects of vaccination for influenza in this study. Similarly, a comparison of the severity of symptoms was difficult from a chart review. These issues need to be examined in future studies. In addition, we did not extract the data for three symptoms (taste disturbance, dysosmia, and conjunctival hyperemia) because they were inaccurate; therefore, these symptoms were not included in the chart reviews of patients with influenza. Additionally, the patients enrolled in this study were limited to those from a single hospital. Finally, this was a retrospective study. Hence, a multicenter prospective study should be conducted with a larger number of patients to verify our results.
Conclusions
Our results are useful for differentiating COVID-19 from influenza. An age of 15 to 70 years (vs. 71 years), breathing difficulty, and malaise were significantly more frequent in patients with COVID-19 than in those with influenza. However, nausea, body temperature >38.1°C, and WBC count >9000/μL were more frequent in patients with influenza than in those with COVID-19.
Footnotes
Authors’ contributions
All of the authors contributed to the study concept and design. SF and AI enrolled the participants and acquired the data. SF and DK analyzed and interpreted the data. SF, AI, MS, and TN prepared the manuscript.
Data sharing statement
No additional data are available.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.