
Abstract
We report the immediate improvement of weakened muscles after combined treatment with transcranial direct current stimulation (tDCS) and peripheral electrical stimulation (PES) in a patient with acute central cord syndrome (CCS) who presented with severe upper limb motor dysfunction. A 70-year-old man sustained CCS with severe motor deficits in the left upper limb, which did not improve with conventional training until 6 days after injury. On the seventh day after the injury, the left upper limb was targeted with combined tDCS (1 mA for 20 minutes/day, anode on the right, cathode on the left) and PES (deltoid and wrist extensors, 20 minutes/day at the motor threshold), and his performance score immediately improved from 0 to 6 on the Box and Block test. After four sessions, the left upper limb function improved to 32 on the Box and Block test, and manual muscle test scores of the stimulated deltoid and wrist extensors improved from 1 to 2. This improvement of the left upper limb led to improved self-care activities such as eating and changing clothes. Exercise combined with tDCS and PES may be a novel treatment for upper limb movement deficits after acute CCS.
Keywords
Introduction
Central cord syndrome (CCS) is the most common type of incomplete cervical spinal cord injury (SCI) and commonly occurs after traumatic injuries. 1 CCS is characterized by an injury to the central portion of the cervical spinal cord. Muscle weakness is more severe in the upper limbs than in the lower limbs because the corticospinal tracts in the upper limbs are more central than those in the lower limbs in the transverse section of the cervical spinal cord. 1 Other clinical manifestations include severe motor paralysis of the upper limbs combined with sensory disturbances, neuropathic pain, and bladder and rectal disorders, resulting in a wide variety of functional disabilities and movement restrictions. 2,3 Blasetti et al. 4 reported that patients with CCS have a residual loss of function in the upper limbs and fingers, leading to reduced self-care abilities and difficulty using walking aids. They also reported that patients with CCS have poorer outcomes related to activities of daily living (ADLs) than those with incomplete cervical spinal cord injuries without CCS. 4 Therefore, it is essential to aggressively improve upper limb and hand functions as early as possible to achieve ADLs such as self-care.
Transcranial direct current electrical stimulation (tDCS) can noninvasively modulate the excitability of the cerebral cortex via application of a weak direct current to the scalp and has been proposed to modulate spontaneous neuronal firing rates during stimulation in the short term and synaptic plasticity in the long term. 5 –7 A recent review that included studies in healthy adults suggested that anodal tDCS of motor-related brain regions can positively affect motor performance because anodal stimulation excites these brain regions. 8,9 The mechanism is not yet fully elucidated, but it has been reported to be mediated by N-methyl-D-aspartate receptors and sodium and calcium channels. 10,11
Peripheral electrical stimulation (PES) is another adjunctive therapy widely used in rehabilitation to restore movement after paralysis. The efficacy of PES in the recovery of paralyzed muscles has long been reported and has been suggested by recent meta-analyses. 12 –16 The putative mechanisms have been reported to include GABAergic interneurons at the level of the cerebral cortex, alteration of spinal excitability, antidromic activation of motor and Renshaw neurons, promotion of synapse formation, and release of neurotransmitters that facilitate synapse formation. 17 –19
We examined whether the combination of tDCS and PES, which have different mechanisms of action, could restore motor function in an additive manner. Previous reports have suggested that combined tDCS and PES may contribute to the recovery of upper limb dysfunction in patients with CCS, 20 –23 but, to the best of our knowledge, there are no such reports of this treatment in patients. In the present case report, we present the treatment details of a patient with CCS with severe motor impairment in the left upper limb who was treated with combined tDCS and PES. This case report suggests that a combination of tDCS and PES may be a potential treatment option for refractory upper limb dysfunction in patients with CCS.
Case report
A 70-year-old man was injured after falling 70 cm into a rice paddy while riding his road bike. At presentation to the emergency department, he had severe motor paralysis and intense numbness in both upper limbs. On physical examination, the patient was awake with stable vital signs. Manual muscle testing (MMT) indicated severe upper limb weakness, predominantly on the left side, but no muscle weakness in the lower limbs (Table 1). According to the International Standards for Neurological and Functional Classification of Spinal Cord Injury (ISNCSCI), 24 the patient's lower limb motor score was maximal, while the upper limb motor scores were 12 points for the right upper limb and 7 points for the left upper limb. The patient's pinprick and light touch sensory scores were both 102 points, with declines observed only in the two upper limbs. The patient also complained of hypesthesia and severe numbness predominantly in the left upper limb, although no left-right difference could be detected in the sensory scores. The patient did not present with any deep tendon or pathological reflex, bladder dysfunction, or other autonomic dysfunction. Cervical plain radiographs showed no fractures, dislocations, or cervical spine instability, and cranial computed tomography showed no acute intracranial lesions. Cervical magnetic resonance imaging revealed mild stenosis at the C3 to C7 level and intraspinal hyperintensity with a slight left-sided predominance at the C4/5 level on T2-weighted images (Figure 1a, b). The patient's clinical diagnosis was CCS, classified as C4 AIS D according to the ISNCSCI. The patient had a history of hypertension and medication use. His occupation of manufacturing precision metal molds required skillful upper limb and hand functions. This case study was conducted after receiving approval from the Research Ethics Committee of the University of Fukui (approval number 20138018) and conformed to the standards set out by the World Medical Association Declaration of Helsinki. We explained the purpose of the study to the patient and obtained his signed consent. This case report was prepared according to CARE guidelines. 25
Manual muscle testing at admission, at the start of rehabilitation, and at transfer to the acute care hospital.

R, right; L, left.

T2-weighted magnetic resonance imaging of the cervical spine shows a hyperintense region at the C4/5 level (arrow) in the sagittal view (a) and on the left side at the C4/5 level (arrow) in the axial view (b).
Physical therapy and occupational therapy were initiated 3 days after the injury. The patient’s chief complaint during rehabilitation was the inability to move both upper limbs, especially the left upper limb. The left upper limb muscle strength showed improvement on MMT of the elbow extensors and slight improvement not reflected by MMT compared with that at the time of injury, but severe muscle weakness remained (Table 1). The patient was classified on the American Spinal Cord Injury Association Impairment Scale as category D and on the modified Frankel classification as D1, with incomplete paralysis in the C5 medullary segment. The patient was unable to use his upper limbs while standing and required significant assistance. He could hold the sitting position independently and walk with a walker with minimal assistance. Our occupational therapist provided the patient with conventional upper limb training for 40 to 60 minutes per day, which consisted of active assistive exercises using a portable spring balancer and sanding exercise from the fourth to the sixth day after the injury, but no change was observed. Therefore, we decided to perform a left upper limb training protocol during combined tDCS and PES in addition to conventional upper limb training.
Combined tDCS and PES
The protocol shown in Figure 2a was administered to the patient once a day for 4 days, starting on the sixth day after injury. First, the Box and Block Test (BBT) was used as an upper limb functional assessment before stimulation. The BBT assesses the number of cubes that can be moved from one box to the contralateral box in 1 minute using the unilateral upper limb and has been reported to be highly reproducible. 26,27 Next, upper limb exercises were performed for 20 minutes per day during combined tDCS and PES. After the stimulation, the BBT was performed again, and then further conventional upper limb exercises were performed by an occupational therapist.

(a) Treatment session. (b) Schema of combined tDCS and PES. BBT: Box and Block Test, tDCS: transcranial direct current stimulation, PES: peripheral electrical stimulation.
A schema of the combined tDCS and PES is shown in Figure 2b. The DC-Stimulator Plus (NeuroConn, Ilmenau, Germany) was used to apply tDCS. On the basis of the International 10–20 system, the anode was placed over the right primary motor cortex (C4), and the cathode was placed over the left primary motor cortex (C3) using 5 × 7-cm saline-soaked electrodes, and stimulation was applied at 1 mA for 20 minutes. An electrical stimulator (ESPURGE, Ito Co., Ltd., Tokyo, Japan) was used to apply PES. One pair of electrodes was attached to each deltoid and wrist extensor of the left upper limb. The stimulation frequency was modulated at 20 to 100 Hz, the pulse width was 250 µs, and the stimulation intensity was set to the motor threshold. We chose 20 to 100 Hz as the stimulation frequency because 20 to 50 Hz is a commonly used frequency for PES, 28 and a 100 Hz frequency is more effective in eliciting central activation. 29 PES was performed during tDCS as much as possible, and this was defined as combined stimulation. The exercises performed during the stimulation included grasping and lifting a towel or ball, with which the patient experienced difficulty. To monitor the safety of stimulation, we measured the patient’s vital signs before and after training and periodically asked the patient whether any discomfort or headaches occurred during stimulation.
Results
The left upper limb BBT before the first session of combined stimulation is shown in Supplemental Video 1. The patient could grasp the cube; however, he had difficulty holding the wrist joint in dorsiflexion and raising the upper limb, and the BBT result was 0, even after using the compensatory movement of leaning the body to the side. The left upper limb BBT immediately after the first session of combined stimulation is shown in Supplemental Video 2. Immediately after stimulation, the patient could hold the wrist in dorsiflexion and raise the upper limb slightly, with a BBT result of 6. The left upper limb function, which had not changed from the time of injury, showed a slight improvement immediately after combined stimulation for 20 minutes.
The numbers of displaced cubes in the left upper limb BBT before and after the four sessions of combined stimulation are shown in Figure 3. In the second combined stimulation session, there was no immediate change in the BBT score between before and after stimulation; however, the score increased by five cubes in the third stimulation session and eight cubes in the fourth stimulation session. Furthermore, the number of cubes in the BBT before combined stimulation showed an increasing trend over time with the number of sessions, indicating improved upper limb function.
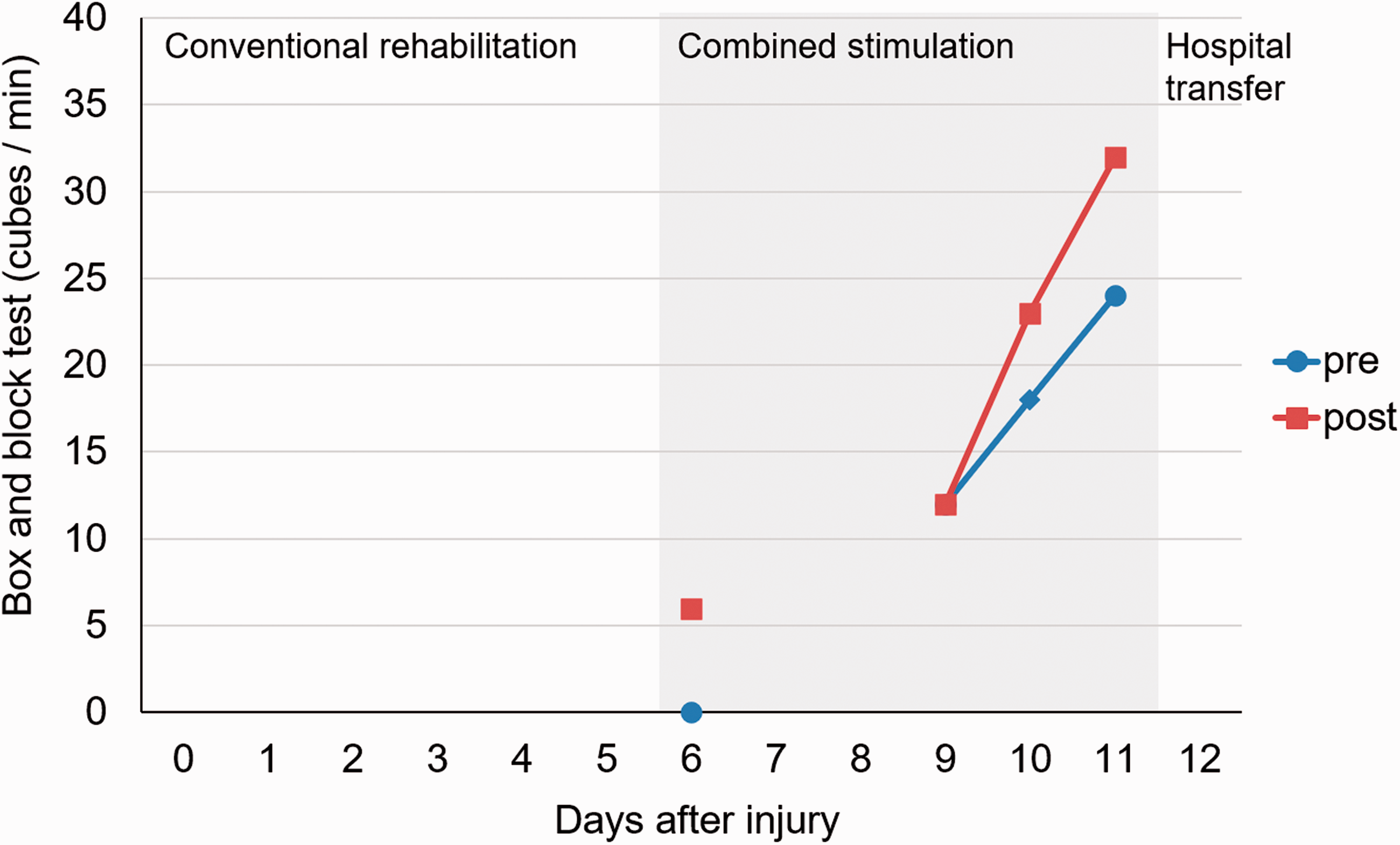
Changes in Box and Block Test results before (blue line) and after (red line) combined transcranial direct current stimulation and peripheral electrical stimulation. The x-axis shows the number of days after the date of injury, and the y-axis shows the performance on the Box and Block Test (number of cubes per minute).
The BBT after the fourth combined stimulation session is shown in Supplemental Video 3. The patient could grasp a cube in a functional limb position with the wrist joint held in mild dorsiflexion. In addition, the patient was able to raise the upper limb while grasping the cube and moving it into the contralateral box, resulting in a BBT score of 32. Thus, we observed the recovery of the deltoid and wrist extensor stimulated during the session and an improvement in the repetitively practiced grasping and lifting of objects during combined stimulation. Over the four sessions, there were no adverse effects associated with tDCS, such as itching, tingling, headache, or mood discomfort, as shown in previous systematic reviews. 30
After the fourth combined stimulation session, the patient's upper limb MMT score improved, as shown in Table 1. The patient's ISNCSCI upper limb motor score improved to 21 points for the right side and 16 points for the left side. As a result of this improvement, the patient could hold a bowl with the left upper limb, use chopsticks with the right upper limb, and eat independently. In addition, the patient was able to use both of his upper limbs for dressing, and the amount of required assistance was reduced. Regarding the patient's ADL at the time of admission, he had a Functional Independence Measure (FIM) score of 66 and a motor FIM score of 31, but after four sessions of combined stimulation, these improved to 94 and 59, respectively (Figure 4). The day after the fourth combined stimulation session, 12 days after the injury, the patient was transferred to a rehabilitation hospital and then discharged 1 month after the injury. The patient's upper-limb function recovered to the point where he could perform daily activities, his FIM score and motor FIM score improved to 121 and 86 points, respectively, and he was able to return to work.

Radar chart of changes in Functional Independence Measure (FIM) scores at admission (blue line), discharge from the acute care hospital (red line), and discharge from the rehabilitation hospital (green line).
Discussion
In this case report, a patient with CCS with severe left upper limb motor dysfunction was trained using a combination of tDCS and PES, and his progress was observed. The patient's left upper limb did not improve, despite usual rehabilitation, until 6 days after the injury; however, 7 days after the injury, the left upper limb showed immediate improvement after training using combined tDCS and PES. Furthermore, training combined with tDCS and PES resulted in improved motor function over time for four sessions. The deltoid and wrist extensors treated with PES improved, and the patient was able to grasp an object and raise his upper limb while keeping the wrist in the dorsiflexed position. These left upper limb function improvements also seemed to improve the patient’s ability to perform self-care activities, such as eating and changing clothes.
Bilateral tDCS, in which an anodal electrode is attached on one side of the motor cortex and a cathodal electrode is attached to the opposite side, has been suggested to be more beneficial than unilateral anodal tDCS in improving motor performance. 31 –33 Additionally, the effects of bilateral tDCS have been reported to possibly be more sustained than those of unilateral anodal tDCS. 32 –34 Although there is growing interest in investigating the effects of tDCS in improving motor function after SCIs, there are few related studies. Yozbatiran et al. reported that 10 sessions of 2 mA anodic tDCS of the primary motor cortex combined with robot-assisted arm training in patients with chronic incomplete SCI showed a trend toward improved arm and hand performance compared with the sham tDCS group. 35 Potter-Baker et al. also reported that 10 sessions of 2 mA anodal tDCS of the primary motor cortex combined with upper limb training in patients with chronic incomplete SCI resulted in improved upper limb muscle strength and plastic changes in the upper limb motor-related cortex. 36 Cortes et al. investigated the effects of one session of 1 mA, 2 mA, or sham tDCS of the primary motor cortex on upper limb motor performance in patients with chronic cervical SCI. They found that a single session of 2 mA anodal tDCS resulted in subtle improvements in hand motor function that were not observed using functional clinical measures. 37 A recent meta-analysis including these studies reported that tDCS had a small but significant effect size in improving motor function in patients with incomplete SCIs, such as CCS. 38 However, most of the included studies were conducted on patients in the chronic disease phase, and the efficacy and safety of this procedure in the acute phase are unknown.
Celnik et al. 20 performed combined tDCS and PES in patients with chronic stroke and reported that combined stimulation was more effective than each type of stimulation alone in improving upper limb motor performance. Sattler et al. 21 also reported that combined tDCS and PES in patients with acute ischemic stroke accelerated the recovery of hand motor function compared with sham tDCS, and the effect persisted even after 1 month. Paired associative stimulation combining transcranial magnetic stimulation and PES, which is a different type of brain stimulation from tDCS, was also reported to have the potential to improve hand function and walking ability in patients with chronic SCI. 22,23
In patients with acute SCI, structural and functional changes seem to occur at the injury site and the brain regions more cranial to the injury site. Previous studies have reported that structural changes in the primary motor cortex of acute SCI patients include decreases in volume and cortical thickness, so-called injury-related atrophy. 39 –41 Jurkiewicz et al. 42 used functional magnetic resonance imaging to observe the functional changes in the brain in SCI patients from the time of injury until 1 year later and compared them with those of healthy subjects. The results showed decreased motor-related activity in the primary motor cortex during the acute phase within 1 month after injury, but an increase was observed as motor function recovered. 42 A similar study also reported that patients with motor function recovery after SCI had increased activity in the primary motor cortex during the first 3 months after injury. 43
The most crucial factor in the recovery of motor function after SCI is the amount of corticospinal tract remaining at the injured site. 39,44 However, in light of the studies showing cortical changes in patients with acute SCI and their recovery process, it seems logical that interventions attempting to activate the remaining primary motor cortex and corticospinal tracts in the acute rehabilitation of patients with incomplete SCIs, such as the present CCS case, may be a viable therapeutic option to promote motor function recovery. The left upper limb with severe motor deficits in the present case did not improve with conventional rehabilitation until 6 days after the injury. However, improvement was observed immediately after combined tDCS and PES on the 7th day after the injury. Furthermore, the combined stimulation was continued for four sessions, and improvement was observed in each session.
Several similar studies have conducted tDCS and PES in patients with chronic SCIs. 35 –37,45,46 Studies have reported that both tDCS and PES produce an immediate improvement in upper-limb performance and increased excitability of the primary motor cortex after one session of stimulation. 37,45,46 Potter-Baker et al. 36 reported a longitudinal study of a 2-week intervention combining tDCS and exercise that showed improvements in upper limb strength and findings indicative of multiple sites of cortical plasticity associated with one another. Recently, rehabilitation with tDCS was shown to accelerate the improvement of upper limb function and maintain long-term improvement in patients with acute stroke, who are similar to patients with acute SCI in terms of reduced output of the primary motor cortex to the injured nerve. 47 Thus, both tDCS and PES are independently effective, but some reports show that their combination is more beneficial than each method alone. 20,21
In addition to the increase in excitability of the primary motor cortex on the stimulus side because of unilateral anodal stimulation reported in previous studies, the bilateral stimulation employed in the present study has been reported to decrease interhemispheric inhibition. 48,49 As a result, bilateral stimulation has been suggested to produce a greater improvement in motor performance than that of unilateral tDCS in healthy subjects. 31 In this case report, bilateral tDCS was performed by targeting the right primary motor cortex, thereby innervating the left upper limb; however, the function of the limb was not improved by this technique, and training was performed on the severely paralyzed muscle using PES. We could not determine whether this montage worked additively per the mechanism presented in previous studies because this was not investigated. However, we hypothesize that the respective mechanisms of bilateral tDCS and PES may have been the basis for the present improvement. In addition, because this is a case report and no controlled trial exists, the efficacy of the treatment cannot be stated definitively. However, in this case, it is important to note that although no change was observed during conventional rehabilitation, improvement in upper limb function was observed immediately after combined tDCS and PES, suggesting that the effect was related to the intervention.
Prior to stimulation, this patient was unable to grasp and move the cubes with his left upper limb because of decreased strength in the deltoid and wrist extensors. Therefore, during combined tDCS and PES, the deltoid and wrist extensors were stimulated with PES, and the patient repeatedly practiced the grasping movement with the wrist in an extended position. As a result, the functions of the deltoid and wrist extensors improved, and the patient could grasp cubes with the wrist dorsiflexed and moved by raising the upper limb. A previous study of patients with chronic stroke reported that the combination of high-frequency repetitive transcranial magnetic stimulation of the motor cortex of the affected hemisphere and training of paralyzed wrist extensors using electrical stimulation significantly improved wrist extensor function and produced use-dependent plasticity in the primary motor cortex. 50 In addition, Potter-Becker et al. confirmed that combining training targeting the impaired muscle with tDCS for 2 weeks in patients with chronic SCI resulted in improved strength of the impaired muscle and plastic changes in the motor cortex and that both results were associated. 36 As suggested by the effectiveness observed in these reports, the combination of tDCS and exercises using PES targeting the strongly impaired muscle may have been beneficial in the present case. We suggest that this treatment strategy is beneficial. However, further confirmation by a randomized controlled trial with multiple cases and neurophysiological studies is needed to confirm this finding.
Many tDCS studies have reported the safety of tDCS, and no serious adverse effects have been reported. 51 However, there are still few studies on the safety of tDCS for patients in the acute phase of SCI. In this case, we did not observe any adverse effects related to tDCS, in accordance with previous systematic reviews; 30 therefore, the safety of tDCS was considered to be ensured. One of the most devastating aspects of cervical SCI is the impairment of upper limb and hand functions, which is a high priority for improvement and significantly impacts ADLs. 52 The rapid improvement of upper limb function by combined tDCS and PES observed in this case report, which led to improvement in self-care activities such as eating and dressing, may help to improve upper limb function in the acute phase.
There are several limitations of this case report. In patients with acute SCI, primary mechanical injuries are followed by secondary injuries that expand the inflammatory response at the lesion site. 53,54 Adaptation/minimization of secondary injuries occurring after SCI is considered essential for maintaining residual corticospinal tracts at the injury site, a critical factor in the recovery of motor function. 53,54 Secondary injury during the acute phase of SCI might have led to the limited improvement of the poor upper limb function up to the sixth day after injury in this patient. It is also unclear whether the present training with combined tDCS and PES positively affected the inflammatory response secondary to the acute phase of SCI, and this is a major limitation that needs to be investigated in the future. Furthermore, the critical limitation of this study is that the results were obtained from a limited outcome measure in only one patient; therefore, the results cannot be generalized. The most important limitation is that we could not exclude the possibility of spontaneous recovery of motor function in the acute phase. Furthermore, we could not provide evidence that training with only four combined tDCS and PES sessions would lead to long-term recovery. However, the improvement of the patient's left upper limb function immediately after combined tDCS and PES despite the poor recovery in the early phase of injury seems to suggest the effectiveness of combined stimulation. Additional studies with crossover designs and randomized controlled trials, including neurophysiological evaluations, are needed to verify this hypothesis.
Supplemental Material
sj-pdf-4-imr-10.1177_03000605221083248 - Supplemental material for Combining transcranial direct current stimulation and peripheral electrical stimulation to improve upper limb function in a patient with acute central cord syndrome: a case report
Supplemental material, sj-pdf-4-imr-10.1177_03000605221083248 for Combining transcranial direct current stimulation and peripheral electrical stimulation to improve upper limb function in a patient with acute central cord syndrome: a case report by Hideaki Matsuo, Masafumi Kubota, Yasue Hori, Yuya Izubuchi, Ai Takahashi, Shuji Watanabe, Hideaki Nakajima and Akihiko Matsumine in Journal of International Medical Research
Footnotes
Acknowledgements
The authors would like to thank Mr. Hiroaki Naruse, Mr. Kazuki Shoji, and Mr. Ryona Yagi from the Division of Physical Therapy and Rehabilitation Medicine, University of Fukui Hospital, Fukui, Japan, for their great help in data collection and interpretation. We would also like to thank Mr. Seiichiro Shimada, our chief physical therapist, for providing the environment to present this case report. We would like to thank Editage (![]() ) for English language editing.
) for English language editing.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by JSPS KAKENHI [grant nos. 16K01502 and 19K19829].
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.