
Abstract
Dizziness is an atypical symptom of the nervous system. Many neurological disorders can manifest as dizziness. When patients have multiple neurological disorders, the most obvious diagnosis is often considered, and diseases that are potentially more deadly are overlooked. Here, we report the case of a man aged in his early 50s with dizziness who was found to have four neurological disorders. A series of treatments failed to resolve the condition. A review of this case highlights that when a patient’s symptoms are not typical, a comprehensive examination and evaluation is required to determine the etiology, and imaging may reveal further minor problems.
Keywords
Introduction
Glioblastoma multiforme (GBM) is a highly aggressive subtype of glioma and the most common malignant brain tumor of the central nervous system. 1 GBM is characterized by a high growth rate, invasiveness, and recurrence. Although the global annual incidence of GBM is fewer than 10 of every 100,000 people, the fatality rate within 2 years of diagnosis is considerably high, even with therapeutic intervention. 2 Therefore, early diagnosis of gliomas is important. In the case reported here, treatment of glioma was delayed for various reasons, and we discuss the outcome of this particular patient with glioma to assist physicians in clinical practice.
Case report
On 12 January 2018 in the Spinal Surgery Outpatient Department of our hospital, a man aged in his early 50s complained of experiencing dizziness for the previous month. The man’s work required him to bow his head, and dizziness was his only symptom. Physical therapy and massage helped his dizziness, and the outpatient doctors suspected cervical spondylosis between the fourth and fifth cervical vertebra. A magnetic resonance imaging (MRI) scan of the neck was performed, which revealed probable mild posterior herniation of four to five cervical discs (Figure 1). However, the neck MRI results also included the sella, and likely space-occupying lesions were incidentally found in the saddle area (Figure 1a). Because the patient had atypical dizziness symptoms and a mild disc bulge, the dizziness was considered to be related to the saddle area lesions.

Imaging examinations from 12 January to 2 February 2018. (a) A T1-weighted magnetic resonance image of the neck (12 January 2018) shows probable mild posterior herniation of four to five cervical discs with suspicious space-occupying lesions in the saddle area of the sella turcica. (b) Enhanced magnetic resonance image (15 January 2018) of the saddle region displays a probable Rathke cleft cyst, which was confirmed by the postoperative pathology results. (c) Initial postoperative head computed tomography (CT) (17 January 2018) shows a small high-density shadow in the right lateral cleft of the saddle area. (d) Head CT (2 February 2018) shows a high-density shadow on the right temporal lobe.
The patient was admitted to the Neurosurgery Department on 15 January 2018 for further treatment. Enhanced MRI of the saddle region was performed, which revealed a probable Rathke cleft cyst in the pituitary gland (Figure 1b). The cyst was removed via neuroendoscopy. The postoperative pathology results suggested a Rathke cyst (Figure 2a).

Postoperative pathology examinations from 15 January 2018 to December 2019. (a) Rathke cyst (15 January 2018). (b) Grade II glioma (14 September 2018). (c) Glioblastoma (December 2019).
The initial postoperative head computed tomography (CT) results reviewed on 17 January 2018 showed a small high-density shadow in the right lateral cleft of the saddle area (Figure 1c). The patient’s dizziness remained. A head CT scan reviewed on 2 February 2018 showed a high-density shadow on the right temporal lobe (Figure 1d) and a thick and large vascular shadow in the right frontal area. There was no change in the high-density shadow on the right temporal lobe, and thus the vascular shadow redirected our attention. Therefore, a head CT angiography plus CT venography examination was arranged for the patient, which indicated a right frontal vascular malformation. The imaging physician suggested performing digital subtraction angiography (Figure 3a, b, c). The improved imaging results from digital subtraction angiography indicated a dural arteriovenous fistula of the right forehead (Figure 3d).
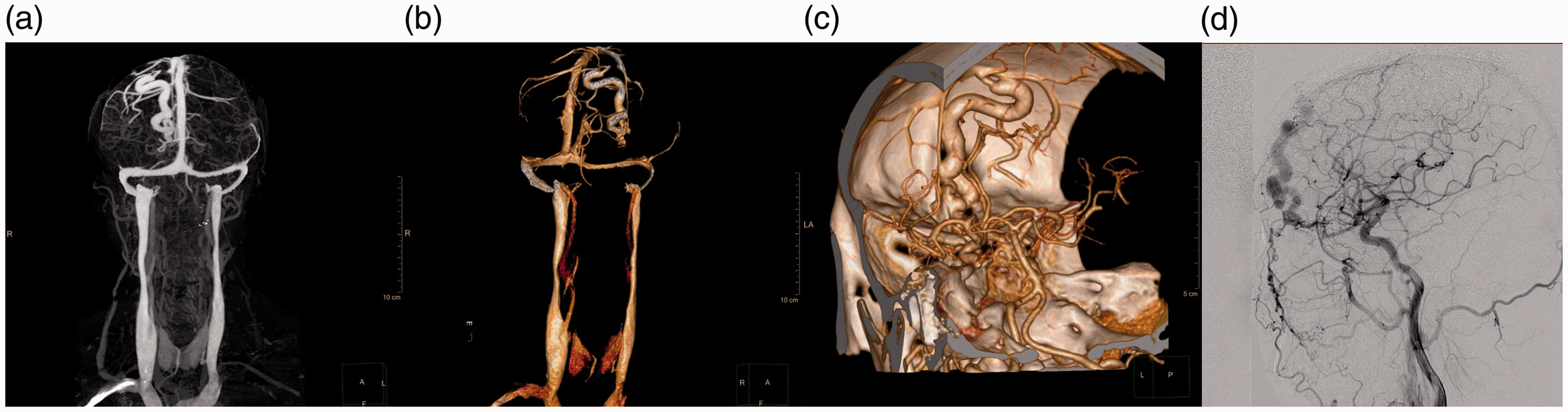
Images of the dural arteriovenous fistula. (a, b) Head computed tomography (CT) angiography. (c) CT venography indicates a right frontal malformation. (d) Digital subtraction angiography displays a dural arteriovenous fistula of the right forehead.
Neurosurgery was repeated to clamp the dural arteriovenous fistula. The postoperative review concluded that the patient's arteriovenous malformation was cured, and he was discharged. On 14 September 2018, the patient suffered a sudden severe headache and visited the emergency department of our hospital. The patient was examined via head CT, which suggested a right frontal and temporal lobe hemorrhage of approximately 20 mL (Figure 4a). The previous temporal lobe lesions had become larger and more characteristic of tumors.

The temporal lesion was found. (a) 14 September 2018; head computed tomography led to suspicion of a right frontal and temporal lobe hemorrhage of approximately 20 mL. The previous temporal lobe lesions had expanded and were now more characteristic of tumors. (b, c, d) Cranial enhanced magnetic resonance imaging plus magnetic resonance spectroscopy. (b) T1-weighted magnetic resonance image of the head. (c) T2-weighted image. (d) Fluid-attenuated inversion recovery. (e) Enhanced T1 weighted image.
Considering the possibility of tumor, a cranial enhanced MRI plus magnetic resonance spectroscopy examination was conducted and indicated occupancy of the right frontal lobe, temporal lobe, insular lobe, and basal node area (Figure 4b, c, d, e). The tumor was determined to be large, and another surgery was scheduled. An intraoperative frozen section pathological examination suggested high-grade glioma; the postoperative pathology results indicated grade II glioma (Figure 2b).
The tumor was almost entirely excised, and the patient and his family refused a genetic analysis. However, temozolomide was used for chemotherapy. Radiotherapy was not considered by the family members. The patient had significantly improved postoperative symptoms and was discharged.
In December 2019, the patient’s condition deteriorated, and he visited the neurosurgery clinic. An enhanced MRI scan of the head showed an irregular mass shadow in the right lateral posterior ventricle, thalamus area, and temporal lobe, and glioma recurrence with edema was considered (Figure 5). After glioblastoma was surgically confirmed (Figure 2c), the family refused further treatment (radiotherapy, chemotherapy, or repeat surgery), and the patient died in September 2020. In the final operation, we removed most of the tumor but did not achieve complete resection.

Image of glioma recurrence. (a) A second T1-weighted enhanced magnetic resonance image of the head. (b) T2-weighted image. (c) Fluid-attenuated inversion recovery. (d) Enhanced T1 weighted image.
The reporting of this study conforms to the CARE guidelines. 3 The patient and his family granted consent for all treatments received.
Discussion
Glioma is the most common primary intracranial tumor. It is derived from neuroepithelial tissue and classified as grades I to IV. 4 Calcification occurs in 70% to 90% of oligodendrogliomas. The calcified portion of an oligodendrocytoma often lines the vessel wall of the gyrus or the surrounding tumor tissue and thus often is present in typical curved bands or shaped as a gyrus. It can also present as a plaque and can be observed as a mass shadow. Combined with CT, MRI of a relevant area is helpful for early differential diagnosis. 5
The present case is consistent with the above description. Early imaging showed isolated right intracranial plaque calcification with no significant edema in the surrounding brain tissue, and no obvious clinical signs or seizures were observed. The focus with abnormal density was detected early, and the lesion was small. The patient had recently undergone a craniotomy, and the site resembled a simple subarachnoid hemorrhage. In short, various signs had not been considered. This case emphasizes that early glioma may appear as simple isolated small calcifications in the brain parenchyma on imaging, and insufficient attention will allow glioblastoma to progress.
Intracranial calcification refers to sites of intracranial deposition of calcium, salt, and other substances. Calcified regions exhibit a high-density appearance on cranial CT, while the MRI signals are diverse. Many diseases can lead to intracranial pathological calcification because of their complicated and diverse causes, and this diversity is reflected by imaging manifestations. Such diseases include the following (with examples given): common tumors (meningioma, oligodendroglioma, craniopharyngioma); intracranial infections (cerebral cyst, brain tuberculosis); endocrine and metabolic diseases (hypoparathyroidism); congenital familial genetic diseases (nodular sclerosis); and vascular diseases (arteriovenous malformation, spongiform hemangioma). A lesion can be small, yet its identification may be confusing. 6 In the present case, pathological calcification was mistaken for a simple subarachnoid hemorrhage.
There are few reports of a missed glioma diagnosis, but one such report is described by ZhangWei et al. 7 A combination of multiple neurological diseases that result in the omission of low-grade glioma, as in the present case, is rarely reported. This case highlights that, when a variety of neurological diseases is encountered (or for that matter, systemic disease), a comprehensive examination and analysis is required because a disease cannot be treated if it is not found. Because of the popularity of head CT and MRI, the detection rate of intracranial calcification is very high. When unexplained calcifications are encountered, the imaging analysis should include CT and MRI combined with medical records and, if necessary, craniotomy or stereotactic biopsies. This is especially important because an early clear diagnosis will help in planning a strategy and improving the prognosis.7,8
Conclusion
When a patient’s symptoms are atypical, comprehensive examination and evaluation are needed to determine the etiology of the disease, and imaging may reveal further minor problems. Small foci cannot be ignored, and further examination is necessary when the diagnosis is difficult.
Footnotes
Acknowledgement
We thank Medjaden Inc. for scientific editing of this manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics statement
Written consent was obtained from the patient’s son to publish this case. The manuscript does not disclose the patient’s personal information. Ethics committee approval was not required because this is an individual case report.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.