
Abstract
Objective
To determine the intravenous (i.v.) dose of esmolol needed to attenuate blood loss in patients undergoing posterior lumbar internal fixation (PLIF) surgery.
Methods
This study randomized patients to either the E5 or E10 group. Patients in the E5 group received a 0.25 mg/kg i.v. loading dose of esmolol before anaesthesia, followed by an infusion of 5 µg/kg/min throughout the operation. Patients in the E10 group received a 0.5 mg/kg i.v. loading dose of esmolol before anaesthesia, followed by an infusion of 10 µg/kg/min throughout the operation.
Results
The study analysed 33 patients: 16 in the E5 group and 17 in the E10 group. The mean ± SD blood loss at the end of surgery was significantly greater in the E5 than E10 group (586.3 ± 160.1 versus 347.7 ± 138.0 ml, respectively). The total amount of patient-controlled analgesia (PCA) used was significantly higher in the E5 than E10 group at 8 (26.1 ± 12.0 versus 17.5 ± 8.3 ml, respectively), 24 (58.4 ± 21.3 versus 44.1 ± 16.2 ml, respectively) and 48 h after surgery (90.0 ± 22.5 versus 69.3 ± 22.1 ml, respectively).
Conclusion
A continuous infusion of 10 µg/kg/min of esmolol can safely reduce blood loss during PLIF surgery. It was also shown to reduce postoperative PCA consumption.
Introduction
Controlled hypotension (CH), defined as a reduction in systolic blood pressure (SBP) to 80–90 mmHg or a 30% reduction of the baseline blood pressure (BP), 1 is an anaesthesia technique that has been used for many years to reduce intraoperative bleeding, which enhances surgical field exposure and shortens the surgery time. 2 Therefore, CH is frequently applied in various types of surgery, including spine surgery.2 –4 However, there is some concern about hypoperfusion of the tissue due to reduced blood flow. For example, CH can impair the perfusion of vital organs, leading to complications such as cerebral stroke, renal ischaemia and even, although rare, myocardial ischaemia.3,5 –8 Therefore, agents for CH must be easy to administer, have a short onset time, an effect that disappears quickly when administration is discontinued, a rapid elimination time without toxic metabolites, negligible effects on vital organs and a predictable and dose-dependent effect. 1
Sodium nitroprusside (SNP), nitroglycerine (NTG), nicardipine, milrinone and esmolol are commonly used for CH.1,3,9,10 Among these, esmolol is an ultra-short-acting β−1 antagonist with a rapid onset (2–3 min) and offset of effect (mean half-life = 9 min). 11 Esmolol is often used to stabilize the cardiovascular responses that may occur during tracheal intubation or surgical incision.12,13 Updated recommendations have addressed the perioperative use of β−1 antagonists; perioperative use of β−1 antagonists has been reported to have beneficial effects in patients at risk of myocardial infarction.14,15 Previous studies have revealed the effectiveness of esmolol for attenuating blood loss in CH.16 –18 When used as an adjunct, esmolol has been shown to improve postoperative recovery by reducing postoperative pain intensity and intraoperative anaesthetic and opioid requirements, as well as preventing opioid-induced hyperalgesia.19 –21
However, controversy remains regarding the optimal intravenous (i.v.) concentration of esmolol. The primary aim of this study was to determine the i.v. concentration of esmolol infusion needed to attenuate blood loss in patients undergoing posterior lumbar internal fixation (PLIF) surgery. The secondary aim was to determine the effects of the i.v. concentration of esmolol on haemodynamic parameters. In addition, the effects of esmolol infusion on postoperative pain and patient-controlled analgesia (PCA) consumption were investigated.
Patients and methods
Study population and ethical approval
This prospective randomized study enrolled adult patients (aged 19–80 years) scheduled for PLIF surgery (2–3 levels) in the Department of Anaesthesiology and Pain Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea between August 2019 and May 2020. The inclusion criteria were as follows: (i) patients with no medical history; (ii) patients that had hypertension and diabetes mellitus without any complications. The exclusion criteria were as follows: (i) myocardial infarction or coronary artery disease; (ii) preoperative bradycardia (heart rate [HR] < 50 bpm) and arrhythmia; (iii) lung diseases (e.g. asthma or chronic obstructive pulmonary disease); (iv) a medical history of hypersensitivity to esmolol.
The study protocol was approved by the Institutional Review Board of Seoul St. Mary’s Hospital, The Catholic University of Korea (approval no. KC19MESI0360) and it has been registered with the Clinical Research Information Service of Korea National Institute of Health (identification number: KCT0005133). Each patient provided written and verbal informed consent. The study protocol adheres to the CONSORT guidelines.
Anaesthetic management
A preoperative evaluation was performed in the preoperative clinic 1 week before surgery to optimize comorbid diseases and to refer to other specialists if needed. In the case of patients with hypertension and diabetes mellitus, they were referred to the relevant specialists for perioperative management, including medication. The patients were not premedicated. Upon arrival at the operating theatre, patients were allocated to the Esmolol 5 (E5) or Esmolol 10 (E10) group through computerized block randomization. This study was conducted as a single-blind study, where only the patients did not know the concentration of esmolol to be administered to them. Since elderly patients were included, two anaesthesiologists were involved in this study to ensure careful attention to managing the depth of anaesthesia and haemodynamic parameters. Basic monitoring, including electrocardiogram, noninvasive blood pressure, pulse oximetry and bispectral index (BIS), was applied before induction of anaesthesia. A 200-mg dose of esmolol, one of the standard drugs used with nicardipine (the usage of which is at the discretion of the anaesthesiologist; bolus or continuous infusion as and when needed throughout the surgery) to induce CH in our institution, mixed with normal saline in a 50 ml syringe was prepared for both groups.
Anaesthesia was induced by tracheal intubation 1–2 min after i.v. administration of propofol (1–2 mg/kg), rocuronium (0.6–1 mg/kg) and remifentanil (0.05–1 µg/kg/min). Simultaneously, patients in the E5 group received a 0.25 mg/kg i.v. loading dose of esmolol at induction of anaesthesia, followed by an infusion of 5 µg/kg/min throughout the operation. Meanwhile, patients in the E10 group received a 0.5 mg/kg i.v. loading dose of esmolol at induction of anaesthesia, followed by an infusion of 10 µg/kg/min throughout the operation. After tracheal intubation, anaesthesia was maintained with sevoflurane, remifentanil and O2/air (FiO2 0.4) to keep the BIS between 40 and 60. In particular, the concentration of sevoflurane and remifentanil were carefully controlled with cautious monitoring to the depth of anaesthesia. The left or right radial artery was cannulated with a 22-gauge angiocatheter and the arterial BP, cardiac output (CO) and cardiac index (CI) were continuously monitored using a FloTrac™ sensor (Edwards Lifesciences, Irvine, CA, USA). A target haemoglobin concentration of 10 g/dl, and BP and HR of around 20% of the respective baseline values, were attained with appropriate fluid therapy and transfusion at the discretion of the anaesthesiologist. In patients with SBP <80 mmHg despite adequate blood transfusion and fluid therapy, dopamine was administered and the patient was excluded from the data analysis. To maintain consistency in the anaesthetic technique, only two designated anaesthesiologists were involved in anaesthetic management. After the surgery had been completed, anaesthetics and esmolol infusion were discontinued. Sugammadex (2.0–4.0 mg/kg) was administered to reverse the muscle relaxant effect, and ramosetron (0.3 mg) was administered to prevent postoperative nausea and vomiting; and the arterial line was also removed. Extubation was carried out when the patient’s spontaneous breathing had returned sufficiently and the patient was then moved to the postanaesthesia care unit (PACU). Upon arrival at the PACU, PCA was applied as 1 mg of fentanyl and 0.3 mg of ramosetron in 100 ml of normal saline; and administered using an AutoMed 3200 pump (AutoMed 3000 Series® Ambulatory Infusion Pump; ACE Medical, Seoul, Korea) at a background rate of 1 ml/h and bolus dose of 1 ml (lockout interval = 10 min).
At the end of the surgery, blood loss, the amount of blood transfused, the amount of fluid administered, urine output, the duration of surgery and anaesthesia and the amount of remifentanil consumed were recorded. The amount of blood loss was calculated by adding up the value obtained by subtracting the irrigation solution from the blood collected in the suction bottle and the value from the gauze assuming that fully saturated 10 * 10 gauze contains a blood volume of 12 ml. SBP, diastolic blood pressure (DBP) and HR were recorded before induction of anaesthesia (T0), just before surgical incision (T1), 1 h after surgical incision (T2), 2 h after surgical incision (T3) and at the end of surgery (T4). CO and CI were recorded from T1 to T4. The frequency of measurement for haemodynamic parameters was determined from a pilot study. A visual analogue scale (VAS) pain score and total PCA consumption were recorded at the time of discharge from the PACU (P0), and at 2 (P2), 8 (P8), 24 (P24) and 48 h (P48) after transfer to the general ward.
Statistical analyses
A pilot study was performed to calculate the sample size. Based on a 300-ml difference in the mean value between groups and an SD of 280, the sample size required at a significance level of 5% (two-sided α = 0.05) and power of 80% (1 − β = 0.8) was 18 patients per group, assuming a 10% dropout rate.
All statistical analyses were performed using the SPSS® statistical package, version 18.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Demographic data are presented as mean ± SD for continuous data or n of patients (%) for categorical data and compared using Student’s t-test or χ2-test as appropriate. The remifentanil consumption, blood loss, fluid administered, urine output, VAS score and total PCA consumption were compared using Student’s t-test. Repeated-measures analysis of variance was performed to compare haemodynamic variables (SBP, DBP, HR, CO, and CI) between the groups, with group and time point as the independent variables, after confirming the normality of the data distribution with the Shapiro–Wilk test (P > 0.05). Bonferroni’s correction was applied for multiple comparisons. In all analyses, a P-value <0.05 was considered statistically significant.
Results
This prospective randomized study enrolled 36 patients. Of these, three were excluded from the data analyses (two in the E5 group and one in the E10 group) due to low BP during surgery and loss to follow-up (Figure 1). The demographic and perioperative data are shown in Table 1. The amount of remifentanil administered was significantly higher in the E5 than the E10 group (P = 0.014). No patients required intensive care because of bleeding or hypotension. No patients complained of complications such as myocardial infarction and cerebral stroke during the patient hospital stays.
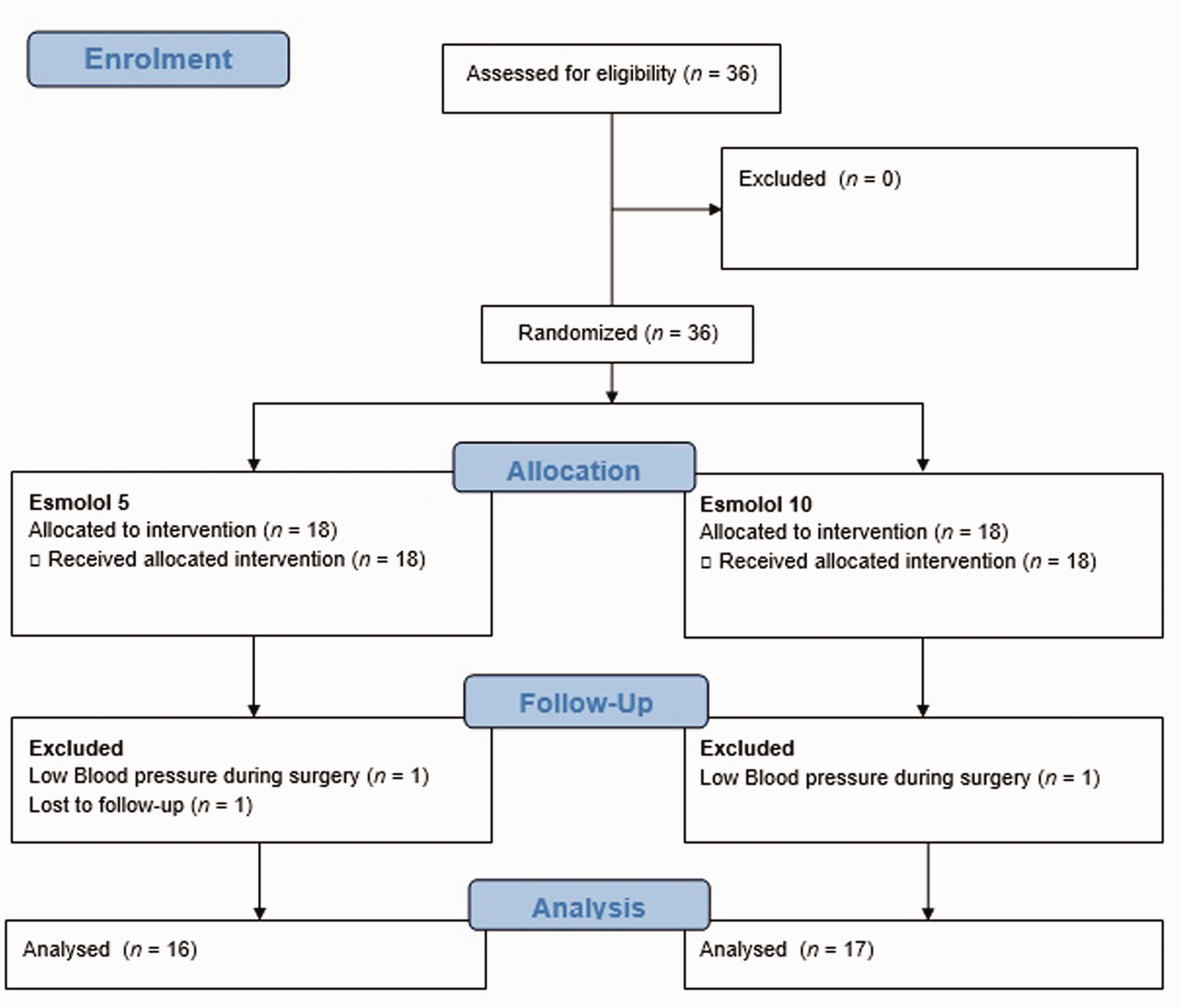
Flow diagram showing the progress through enrolment, randomization and analysis of adult patients (n = 36) scheduled for posterior lumbar internal fixation surgery (2–3 levels) that were enrolled in a study investigating the optimal intravenous concentration of esmolol.
Demographic and perioperative data of adult patients (n = 33) scheduled for posterior lumbar internal fixation surgery (2–3 levels) that were enrolled in a study investigating the optimal intravenous concentration of esmolol.

Data presented as mean ± SD or n of patient.
aContinuous data were compared using Student’s t-test and categorical data were compared using χ2-test; NS, no significant between-group difference (P ≥ 0.05).
The amount of blood loss at the end of surgery was significantly higher in the E5 than E10 group (P = 0.049) (Table 2). However, the transfusion volume, crystalloid and colloid volumes and the urine output were not significantly different between the two groups.
Blood loss and related data of adult patients (n = 33) scheduled for posterior lumbar internal fixation surgery (2–3 levels) that were enrolled in a study investigating the optimal intravenous concentration of esmolol.

Data presented as mean ± SD.
aContinuous data were compared using Student’s t-test; NS, no significant between-group difference (P ≥ 0.05).
There were no significant differences in the baseline (T0) mean ± SD SBP, DBP and HR between the E5 and E10 groups (151.3 ± 24.9 versus 145.4 ± 21.3 mmHg; 82.9 ± 15.3 versus 76.5 ± 12.3 mmHg; 71.3 ± 9.9 versus 68.5 ± 15.7 bpm; respectively). SBP was slightly lower at T2 and T3 in the E10 group than the E5 group, but the differences were not significant (Figure 2A). DBP and HR did not show significant changes at any time points (T1–T4) (Figures 2B and 2C). There were no significant differences in the mean ± SD CO and CI just before surgical incision (T1) between the two groups (4.1 ± 1.1 versus 4.2 ± 1.2 ml/min; 2.6 ± 0.5 versus 2.6 ± 0.6 ml/min/m2; respectively). CO and CI did not show significant changes from baseline values at any time point in either group (T2–T4) (Figure 3).

Changes in vital signs of adult patients (n = 33) scheduled for posterior lumbar internal fixation surgery (2–3 levels) that were enrolled in a study investigating the optimal intravenous concentration of esmolol. Data presented as mean ± SD. SBP, systolic blood pressure; T0, baseline; T1, just before surgical incision; T2, 1 h after surgical incision; T3, 2 h after surgical incision; T4, at the end of surgery; DBP, diastolic blood pressure; HR, heart rate, bpm, beats per min.

Changes in cardiac parameters of adult patients (n = 33) scheduled for posterior lumbar internal fixation surgery (2–3 levels) that were enrolled in a study investigating the optimal intravenous concentration of esmolol. Data presented as mean ± SD. CO, cardiac output; T1, just before surgical incision; T2, 1 h after surgical incision; T3, 2 h after surgical incision; T4, at the end of surgery; CI, cardiac index.
The mean ± SD VAS pain score in the E5 group was significantly higher at P0 than in the E10 group (5.2 ± 2.6 versus 3.7 ± 1.0; P = 0.029) (Figure 4). The VAS pain score showed no significant differences between the two groups at any other time point (P8–P48). The mean ± SD total volume of PCA used was significantly higher in the E5 than E10 group at P8 (26.1 ± 12.0 versus 17.5 ± 8.3 ml; P < 0.05), P24 (58.4 ± 21.3 versus 44.1 ± 16.2 ml; P < 0.05) and P25 (90.0 ± 22.5 versus 69.3 ± 22.1 ml; P < 0.05).

Visual analogue scale (VAS) pain scores and analgesia infusion volumes of adult patients (n = 33) scheduled for posterior lumbar internal fixation surgery (2–3 levels) that were enrolled in a study investigating the optimal intravenous concentration of esmolol. Data presented as mean ± SD. P0, at the time of discharge from the postanaesthesia care unit; P2, 2 h after transfer to general ward; P8, 8 h after transfer to general ward; P24, 24 h after transfer to general ward; P48, 48 h after transfer to general ward; PCA, patient-controlled analgesia. *P < 0.05, between-group comparison; Student’s t-test.
Discussion
This prospective randomized study showed that continuous infusion of esmolol at a dose of 10 μg/kg/min was superior to 5 μg/kg/min for attenuating blood loss during PLIF surgery. There were no significant differences between the two concentrations in terms of haemodynamic parameters such as SBP, CO and CI, at any time point. Continuous infusion of esmolol at 10 μg/kg/min did not cause severe hypotension (and thus hypoperfusion into the tissues). These current results suggested that esmolol can be continuously infused at a dose of 10 μg/kg/min to safely induce CH during PLIF surgery without cardiovascular complications. Also, continuous infusion of esmolol at 10 μg/kg/min was superior for reducing postoperative pain during the PACU stay and postoperative PCA consumption from 8 to 48 h postoperatively. To the best of our knowledge, this is the first study to investigate the effects of different doses of continuous esmolol infusion on intraoperative bleeding and pain.
Intraoperative bleeding is a major concern in spine surgery. One of the most commonly used methods to lower blood loss is the induction of hypotension during surgery. The most commonly used vasodilators for CH are SNP and NTG. 1 SNP directly causes venous dilatation and reduces venous return, which subsequently produces arterial dilatation. 1 It has a very rapid onset time (<30 s) and short duration of action (<2 min). 1 However, it can cause tachyphylaxis, rebound hypotension, myocardial ischaemia, increased intracranial pressure and cyanide toxicity. 1 NTG has a direct vasodilatory effect on the venous capacitance vessels and an indirect effect on the arteries. 1 It has a short duration of action without clinically toxic metabolites or rebound hypertension. 1 However, NTG is less effective for producing hypotension and its effects onset more slowly compared with SNP. 1 NTG is also associated with tachycardia and increased cerebral blood flow; excessive hypotension may occur in patients with low blood volume, which in turn may compromise coronary blood flow. 1
Esmolol is an ultra-short-acting β−1 antagonist with a rapid onset time (2–3 min) and a short duration of action (mean half-life = 9 min). 11 It is hydrolysed by erythrocyte esterases and its elimination is independent of hepatic and renal function. 11 However, esmolol is known to reduce CO (by reducing HR) and increase peripheral vascular resistance, leading to a reduction in myocardial contractility; therefore, it should be used cautiously. 1 Esmolol can be continuously infused over a wide range of concentrations.21,22 A previous meta-analysis reported that low initial bolus doses of esmolol with a continuous infusion strategy resulted in fewer episodes of hypotension. 22 The meta-analysis also found that titration of esmolol to the haemodynamic endpoint was associated with a decreased incidence of myocardial ischaemia, suggesting that esmolol has the potential to safely and effectively prevent myocardial ischaemia in patients undergoing noncardiac surgery. 22 The current study cohort included elderly patients that are vulnerable to hypotension in the major organs. Considering its disadvantages, relatively low doses of esmolol were continuously infused in this current study. Only two patients suffered severe bradycardia and hypotension. This suggests that 10 µg/kg/min esmolol can be continuously infused safely in elderly patients without causing severe bradycardia or hypotension.
As a low concentration of esmolol was continuously infused in this current study, the SBP did not fall below 100 mmHg and HR was maintained at almost the preoperative value. SBP in the E10 group was slightly lower than in the E5 group at 1 and 2 h after surgery, but the differences were not statistically significant. As a result, CO and CI did not fluctuate during surgery. The haemodynamics were likely stable because the esmolol concentration was not sufficient tzo induce hypotension. The stable haemodynamics could also be attributed to the careful monitoring and adjustment of the anaesthetics by the anaesthesiologist. Although the difference in SBP was not large, blood loss in the E10 group was significantly lower than that in E5 group. The lack of any significant difference in the amount of blood transfused or fluid administered was thought to be because the difference in blood loss between the two groups was only approximately 200 ml. There have been studies on the effects of esmolol on intraoperative bleeding in patients undergoing mandibular or nasal surgery.13,16,18,23 –26 Moreover, there have been a few studies on the effects of esmolol on CH in patients undergoing spine surgery.27 –29 However, the dose of esmolol infusion was titrated in these studies, rather than being administered at a constant concentration. A previous study titrated esmolol to 10–200 µg/kg/min, 27 whereas another titrated it to 50–300 µg/kg/min. 29 In contrast, this current study examined the effects on hypotension and bleeding of continuous infusion of esmolol at two different concentrations. Even with continuous esmolol infusion at 10 µg/kg/min, the amount of bleeding decreased without hypotension and bradycardia. These observations suggested that haemodynamic stability can be maintained in patients undergoing spine surgery, including elderly patients, and that blood loss can be reduced even with continuous esmolol infusion at a dose of 10 µg/kg/min from the beginning of surgery.
In the current study, the patients in the E10 group experienced less pain on PACU discharge and required less PCA from 8 to 48 h postoperatively compared with the patients in the E5 group. Esmolol is also known to have antinociceptive and, consequently, opioid-sparing effects. 21 These effects were hypothesized to be mediated by the blockade of β-adrenoreceptors within the brainstem and by reducing neuronal inflow into the central nervous system. 21 Previous studies confirmed the antinociceptive and opioid-sparing effects of continuous infusion of esmolol at various concentrations.19 –21,30 –32 Continuous infusion of esmolol at 10 µg/kg/min was associated with less intraoperative remifentanil consumption in this current study, leading to lower postoperative PCA consumption. A previous study reported that continuous infusion of esmolol at 30 µg/kg/min decreased the requirements for intraoperative remifentanil and fentanyl in the PACU, as well as the pain scores in the PACU of patients undergoing gynaecological surgery. 30 Another study reported that using esmolol as an adjunct led to a decrease in remifentanil consumption, without any decrease in CO during controlled anaesthesia in patients undergoing septorhinoplasty, consistent with the results of this current study. 32 Unlike this current study, however, the previous study titrated the dose of esmolol from 100 to 300 µg/kg/min during total i.v. anaesthesia. 32 Numerous studies have suggested that, paradoxically, intraoperative remifentanil may enhance postoperative pain, and hence the opioid analgesic requirement, after 60–90 min of infusion.33 –35 Intraoperative esmolol continuous infusion at 10 µg/kg/min attenuated remifentanil consumption, consequently resulting in lower VAS pain scores in the PACU and reduced postoperative PCA consumption.
This current study had several limitations. First, it only investigated the effects of relatively low concentrations of esmolol on blood loss. Secondly, it did not investigate postoperative clinical complications such as myocardial infarction and cerebral stroke. Thirdly, the esmolol continuous infusion doses examined were low. However, as the current cohort included elderly patients that are vulnerable to tissue hypoperfusion, safety concerns prevented the infusion of a higher concentration of esmolol. In addition, the possibility of such complications after surgery was considered low, as an intraoperative SBP > 100 mmHg was maintained in most of the patients. Moreover, there was no report of any such complications during the patient hospital stays.
In conclusion, continuous infusion of esmolol at 10 µg/kg/min does not cause haemodynamic instability, even in elderly patients, and it can be used to reduce blood loss during PLIF surgery. Continuous infusion of 10 µg/kg/min esmolol was also shown to reduce intraoperative remifentanil consumption and postoperative PCA consumption.