
Abstract
Objective
To determine the prevalence of Helicobacter pylori infection in a Saudi Arabian population and its association with the body mass index (BMI) and serum 8-hydroxy deoxyguanine (8-OHdG) levels as biomarker for oxidative stress.
Methods
This cross-sectional study enrolled patients that had experienced epigastric discomfort or dyspepsia for > 1 month and had undergone diagnostic upper endoscopy. Patients with a body mass index (BMI) ≥30 kg/m2 were defined as obese. The presence of anti-H. pylori antibodies was confirmed using an H. pylori immunoglobulin G (IgG) antibody enzyme-linked immunosorbent assay. The levels of 8-OHdG were measured using a competitive inhibition enzyme immunoassay.
Results
A total of 298 patients were enrolled in the study. Of these, 186 (62.4%) patients were H. pylori-positive and 112 (37.6%) patients were H. pylori-negative. The mean ± SD age of the overall study cohort was 47.17 ± 9.27 years. The H. pylori-positive patients had significantly higher levels of H. pylori IgG antibodies than H. pylori-negative patients. H. pylori prevalence linearly correlated with BMI quantile. The 8-OHdG levels were strongly associated with the BMI of the patients in the H. pylori-positive group.
Conclusion
Obese individuals exhibited higher H. pylori prevalence than individuals with a lean BMI (BMI < 25.00 kg/m2).
Introduction
Obesity refers to elevation in body weight due to excessive fat accumulation. It is a multifactorial chronic disorder. 1 It is related to several adverse health conditions, including diabetes mellitus, hypertension, sleep apnoea, coronary heart disease and tumours. 2 Based on World Health Organization (WHO) guidelines, an individual with a body mass index (BMI) > 30 kg/m2 are considered to be obese and those with 25 < BMI < 30 kg/m2 are considered as overweight. 3 Elevation in BMI often leads to oxidative stress due to lipid peroxidation and reduced antioxidant activity, which in turn leads to DNA damage. 4 Such oxidative DNA damage is considered to be major cause of obesity-related disorders. 4
Helicobacter pylori is a microaerophilic gram-negative bacteria that resides in the gastric mucosa. It has been known to be a major aetiological factor for chronic gastritis, peptic ulcer, low-grade gastric mucosa-associated lymphoid tissue lymphoma and gastric cancer are all linked to H. pylori infection.5,6 In addition, H. pylori infection may play a role in metabolic disorders. 7 Obese individuals have been shown to exhibit a high prevalence of H. pylori infection and obesity is a risk factor for H. pylori infection. 7 However, some investigators have demonstrated a lower prevalence of H. pylori infection among obese individuals. 8 H. pylori infection has also been shown to accompany insulin resistance and obesity. 9 Previous studies from developed countries have also demonstrated a significant correlation between obesity and risk of H. pylori infection.2,10
Among the Middle Eastern countries, Saudi Arabia exhibits the highest prevalence of obese and overweight individuals, which might be attributed to several factors, such as adopting a western lifestyle. 11 It is estimated that only approximately 4% of the obese individuals live in the rural areas. 11 Among the urban areas, approximately 10% of the obese individuals live in the Western region and 14% in the Eastern region; and such high prevalence levels are attributed to poor food habits and a sedentary lifestyle. 12 In addition, a higher proportion of married individuals are obese or overweight. 12
Helicobacter pylori is hyperendemic in Saudi Arabia with a prevalence of 33–85%.7,12 Irrespective of the results of previous studies conducted in other settings, the studies in Saudi Arabia have shown an H. pylori infection prevalence rate of 88% among morbidly obese individuals that underwent upper endoscopy before bariatric surgery.7,13 If the human immune system does not eliminate H. pylori infection from the body, it leads to a persistent infection, chronic inflammation, oxidative stress and DNA damage.14,15 Hence, it is hypothesized that H. pylori prevalence is associated with obesity and obesity-related adverse health conditions. 10
The overproduction of reactive oxygen species (ROS) causes oxidative stress that triggers lipid peroxidation, DNA damage and protein modification, which leads to chronic inflammation, cancer and cardiovascular disorders.15,16 H. pylori infection and obesity also elevates ROS production via several mechanisms.14,17 ROS induces breaks, deletions and nucleoside modification in single and double-stranded DNA molecules.15,18 The most susceptible nucleotide to ROS is guanine.15,18 The hydroxyl radical within the ROS attacks the C-8 position of the guanine molecule of 2′-deoxyguanosine nucleoside and oxidizes it to 8-hydroxy deoxyguanine (8-OHdG).15,18 8-OHdG is the most potent marker of DNA damage, indicating cellular oxidative stress.15,18
The association between H. pylori infection and obesity remains controversial, although the incidence of both diseases is increasing worldwide. 19 The current study aimed to determine the prevalence of H. pylori and its correlation with BMI and 8-OHdG levels in a Saudi Arabian population.
Patients and methods
Study population
This cross-sectional study of the population of Makkah City, western Saudi Arabia, was undertaken at the Department of Biochemistry, Faculty of Medicine, Umm Al-Qura University, Makkah, Kingdom of Saudi Arabia and it enrolled consecutive patients that had experienced dyspepsia or epigastric discomfort for >1 month and had undergone diagnostic upper endoscopy. The recruitment period was between February 2019 and August 2020. The inclusion criteria were as follows: (i) patients that had complete anthropometric records; (ii) patients with a serodiagnosis of H. pylori test; (iii) patients with an 8-OHdG estimation. The exclusion criteria were as follows: (i) malignancy; (ii) chronic liver and renal failure; (iii) weakness; (iv) connective tissue disorders; (v) a history of eradication therapy.
All personal details of the patients have been de-identified. Each patient provided written informed consent and ethical approval was obtained from the Research Ethics Committee of the Faculty of Medicine, Umm Al Qura University, Makkah, Kingdom of Saudi Arabia (no. HAPO-02-K-012-2019-04-41). The reporting of this study conforms with STROBE guidelines. 20
Measuring obesity
In extensive epidemiological research studies, the BMI remains the most frequently used tool for estimating the prevalence of obesity at the population level. 21 BMI is calculated using the formula BMI = kg/m2 where kg is a person's weight in kilograms and m2 is their height in metres squared.3,21 BMI has been widely accepted and adopted as the most widely used method for assessing body composition on a global scale. The BMI (kg/m2) category definition was based on the WHO guidelines as follows: patients with a BMI ≥ 25 kg/m2 were overweight and those with a BMI ≥ 30 kg/m2 were obese. 3
Measurement of biochemical parameters
Blood samples were obtained following an overnight fasting period according to the diagnostic criteria of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. 22 Samples were withdrawn from a cubital vein into blood tubes and immediately serum was separated from the cells by centrifugation at 3000 rpm for 10 min at room temperature (IEC Centra CL2; Thermo Fisher Scientific, Rockford, IL, USA) and stored in refrigerator at 4°C until processed for lipid analysis and oxidative biomarkers (8-OHdG).
Triglycerides (TG), total cholesterol (TC) and high-density lipoprotein-cholesterol (HDL-C) were measured with an autoanalyser (COBAS INTEGRA® 400 plus analyzer; Roche Diagnostics, Mannheim, Germany) using commercially available kits. Serum LDL-C was calculated according to a computational formula previously published (LDL = TC – HDL – TG/5.0 mg/dl). 23 The Castelli index was used for determining the ratio between total cholesterol and HDL-C. 24 In addition, glycosylated haemoglobin (HbA1c) was measured according to a previous report. 25
Anti-H. pylori IgG ELISA
Helicobacter pylori-specific immunoglobulin G (IgG) antibodies were quantified using a human H. pylori IgG enzyme-linked immunosorbent assay (ELISA) kit according to the manufacturer’s instructions (Abcam®, Cambridge, MA, USA). Briefly, H. pylori antigen-precoated 96-well plates were bound to the cognate antibodies. Then, the test and control samples were added into the wells and the plates were incubated. Next, the plates were washed, and the wells were filled with anti-human IgG horseradish peroxidase (HRP)-conjugated secondary antibody. During the reaction, the interaction of tetramethylbenzidine and HRP yields a blue-coloured product. Later, an acid is added into the wells to terminate the reaction, which changes the colour of this product to yellow. The absorbance of the solution obtained after substrate addition into the wells was measured at 450 nm (SpectraMax M2; Molecular Devices, San Jose, CA, USA). The H. pylori IgG levels in the samples were directly proportional to the intensity of the yellow colour. The minimum detectable concentration was 1.39 IU/ml for anti-H.pylori IgG. Intra- and interassay coefficients of variation for the ELISA were 2.3% and 13.44%, respectively. A value <15 IU/ml was considered negative for the presence of detectable IgG antibody. The patients were stratified into two groups based on the H. pylori IgG antibody analysis: H. pylori-negative and H. pylori-positive.
Serum 8-OHdG measurement
The serum levels of 8-OHdG were quantified from the blood samples using a Cloud-Clone Corp 8-OHdG immunoassay kit according to the manufacturer’s instructions (USCN Life Science, Houston, TX, USA). Briefly, a microplate was pre-coated with an 8-OHdG specific monoclonal antibody. Next, the wells of the plate were filled with 8-OHdG samples with or without biotin labelling (standard or test samples) and incubated. Then, the plate was washed to remove the unbound conjugate. Next, HRP-conjugated avidin was added into the wells, followed by incubation at 37 °C for 30 min. The level of 8-OHdG was inversely proportional to bound HRP level. The absorbance of the solution obtained after substrate addition into the wells was measured at 450 nm (SpectraMax M2; Molecular Devices). 8-OHdG levels in the test samples were obtained using the standard curve obtained from the standard 8-OHdG solutions. The minimum detectable concentration was <26.81 pg/ml for 8-OHdG. Intra- and interassay coefficients of variation for the immunoassay were <10% and <12%, respectively.
Statistical analyses
According to the 2018 report issued by the Saudi General Authority for Statistics and Ministry of Health, the total percentage of obese Saudi in the Western region of the Kingdom of Saudi Arabia was 59% (714 719) from a total population in Makkah of 1 211 389. 26 The sample size was calculated using the Epi Info™ software and the minimum required sample size was 384 participants to achieve a study power of 95%, which represents a confidence level of 95% and 5% of the worst acceptable limit.27 To correct for any possible data loss, the total sample should be larger. 27
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY, USA). Continuous and categorical data are presented as mean ± SD and n of patients (%), respectively. The differences between the groups were evaluated using either χ2-test or Mann–Whitney U-test. Correlation between H. pylori infection and BMI was assessed using Pearson’s correlation coefficient. Correlation among H. pylori infection, BMI and 8-OHdG levels was evaluated using logistic regression analysis. A P-value ≤0.05 was considered statistically significant.
Results
A total of 298 patients were recruited in the study, of which 122 (40.9%) were males and 176 (59.1%) were females. The demographic and clinical characteristics of the study cohort are presented in Table 1. The mean ± SD age of the overall study cohort was 47.17 ± 9.27 years (range, 28–72 years). On the basis of the H. pylori IgG antibody results, 186 (62.4%) patients were H. pylori-positive and 112 (37.6%) patients were H. pylori-negative. There was a significant difference in terms of the mean IgG antibody levels between the two groups (81.13 ± 38.17 IU/ml versus 2.88 ± 1.96 IU/ml; P < 0.0001). There were significant differences between the two groups in terms of age, BMI, triglyceride, high-density lipoprotein cholesterol (HDL-C) and 8-OHdG levels (P < 0.05 for all comparisons). There were no significant differences between the two groups in terms of HbA1c levels, low-density lipoprotein cholesterol (LDL-C) and total cholesterol levels.
Demographic and clinical characteristics and biochemical markers of patients (n = 298) that had experienced dyspepsia or epigastric discomfort for >1 month and had undergone diagnostic upper endoscopy stratified according to their Helicobacter pylori infection status.
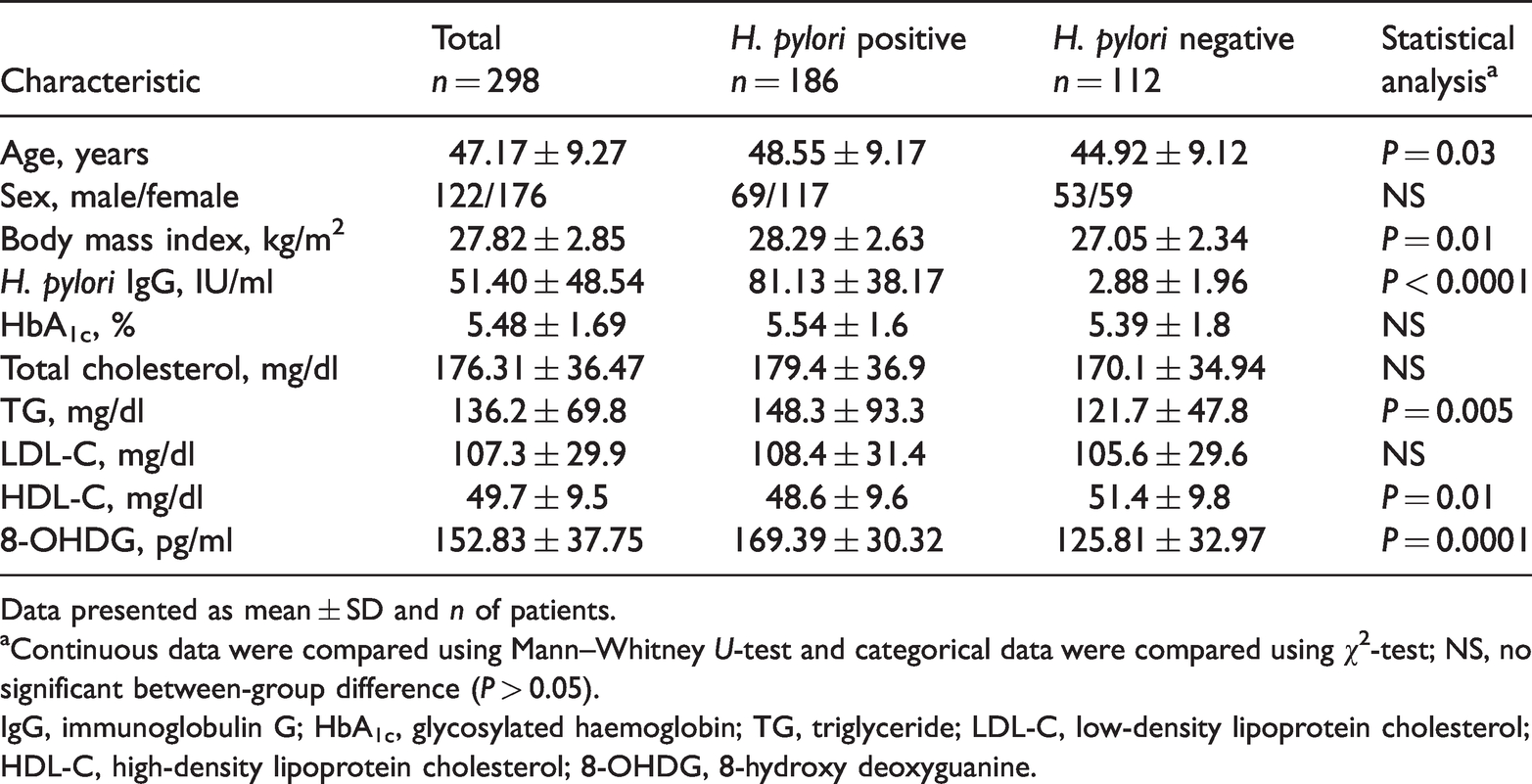
Data presented as mean ± SD and n of patients.
aContinuous data were compared using Mann–Whitney U-test and categorical data were compared using χ2-test; NS, no significant between-group difference (P > 0.05).
IgG, immunoglobulin G; HbA1c, glycosylated haemoglobin; TG, triglyceride; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; 8-OHDG, 8-hydroxy deoxyguanine.
The patients were further divided into three groups based on their BMI as follows: obese (BMI ≥ 30.00 kg/m2), overweight (BMI = 25 kg/m2 < BMI < 30 kg/m2) and lean (BMI < 25.00 kg/m2). As shown in Table 2, the obese patients exhibited the highest H. pylori prevalence (54 of 69 patients; 78.3%), followed by the overweight patients (123 of 194 patients; 63.4%) and the lean patients (nine of 35 patients; 25.7%). The three groups differed significantly on the basis of the prevalence of H. pylori infection (P = 0.008).
Analysis of the body mass index (BMI) category and the prevalence rate of Helicobacter pylori infection in patients (n = 298) that had experienced dyspepsia or epigastric discomfort for >1 month and had undergone diagnostic upper endoscopy.

To further elucidate the relationship between BMI and H. pylori prevalence, the patients were divided into five quintiles on the basis of their BMI where quintiles 1, 2, 3, 4 and 5 represented patients with a BMI ≤ 23.9 kg/m2, 24 kg/m2 < BMI< 25.9 kg/m2, 26 kg/m2 < BMI < 28.9 kg/m2, 29 kg/m2 < BMI < 30.9 kg/m2 and BMI ≥ 30.9 kg/m2, respectively. The prevalence of H. pylori infection in patients in quintiles 1, 2, 3, 4 and 5 were 24.0%, 27.3%, 63.6%, 70.6% and 78.3%, respectively (Table 3). The prevalence of H. pylori infection was significantly different among the patients in the five different quintiles and was found to be highly correlated with the BMI of the patients according to χ2 Pearson’s correlation analysis (χ2 = 52.2; P = 0.0001).
Analysis of the body mass index (BMI) quintiles and the prevalence rate of Helicobacter pylori infection in patients (n = 298) that had experienced dyspepsia or epigastric discomfort for >1 month and had undergone diagnostic upper endoscopy.

The mean ± SD 8-OHdG levels of the overall study cohort was 152.83 ± 37.75 pg/ml (Table 1) (range, 72.83–230.28 pg/ml). The H. pylori-positive group (mean ± SD, 169.39 ± 30.32 pg/ml; range, 120.19–230.28 pg/ml) had significantly higher 8-OHdG levels than the H. pylori-negative group (mean ± SD, 125.81 ± 32.97 pg/ml; range, 72.83–182.85 pg/ml) (P = 0.0001). As shown in Figure 1, the 8-OHdG levels were strongly associated with the BMI of the patients in the H. pylori-positive group (Pearson’s correlation coefficient r = 0.2; P = 0.003).

Correlation between body mass index (BMI) and 8-hydroxy deoxyguanine (8-OHdG) levels in patients (n = 186) with Helicobacter pylori infection. Pearson’s correlation coefficient r = 0.2, P = 0.003.
Discussion
It is still unclear if obesity is associated with H. pylori prevalence. This current study assessed the association between H. pylori infection prevalence and obesity as well as 8-OHdG levels. The results of the current study indicated that 62.4% of the overall study cohort were H. pylori-positive and in the obese BMI category the rate of H. pylori infection increased to 78.3%.
Obesity refers to the excessive or abnormal accumulation of fat that may lead to adverse health conditions. An individual may be classified as obese or overweight using the BMI measure. From 1975 to 2016, the global prevalence of obesity has almost tripled. 28 In 2016 alone, approximately 13% of the global adult population was obese. 21 Saudi Arabia is witnessing an increase in the levels of obesity each year, which might be attributed to several factors, such as environmental, lifestyle, genetic and social. 28 The change in dietary habits and a decrease in physical activity due to the recent economic transition of the country are thought to be the primary causes of the increase in the prevalence of obesity in Saudi Arabia. 28 The current findings demonstrated that in Makkah City, Kingdom of Saudi Arabia, 194 of 298 (65.1%) patients were overweight (BMI ≥ 25 kg/m2) and 69 of 298 (23.2%) patients were obese (BMI ≥ 30 kg/m2).
Helicobacter pylori infection is a highly prevalent chronic bacterial infection that primarily leads to severe gastric and extra-gastric ailments. 29 H. pylori IgG ELISA is the most widely used technique for H. pylori diagnosis. It not only reveals the status of the current infection, but also provides information regarding any previous H. pylori infection. It also leads to false-positive results, which might be interpreted as a high H. pylori infection rate. 5 The current findings demonstrated that the H. pylori-positive group had a significantly higher BMI and H. pylori IgG levels compared with the H. pylori-negative group. Furthermore, a significantly higher proportion of the obese/overweight patients were H. pylori-positive compared with the lean patients. There was also a strong linear correlation between H. pylori positivity and BMI according to Pearson’s correlation coefficient analysis (χ2 = 52.2; P = 0.0001). These findings suggest that there is a higher risk of H. pylori infection in individuals with a higher BMI. These findings were in agreement with the results of previous studies.2,29,30It is noteworthy that some researchers have reported that BMI does not correlate with H. pylori prevalence.9,31 Such inconsistent results might be attributed to sample size and technique of H. pylori diagnosis.
To date, the relationship between H. pylori infection and obesity remains controversial. Elevated BMI or obesity has previously been shown to impair adaptive a well as innate immunity. 32 It has also been shown that morbidly obese individuals exhibit reduced polymorphonuclear bactericidal capacity and monocyte maturation.33,34 Recent research has also shown significantly reduced natural killer cell activity in severely obese patients. 33 Such alterations in the immune system of obese individuals provide a favourable environment for the growth of H. pylori. Furthermore, H. pylori infection promotes the secretion of proinflammatory cytokines, such as tumour necrosis factor-a, interleukin (IL)-1b, IL-6 and IL-8, which leads to insulin resistance, lipid dysmetabolism and chronic inflammation.35,36Lipid dysmetabolism leads to a reduction in HDL-C and apolipoprotein A levels and an increase in LDL-C, insulin, triglyceride and apolipoprotien B levels. 35 These current results indicated no significant differences between the HbA1c, LDL-C and total cholesterol levels of H. pylori-positive and H. pylori-negative patients. However, the levels of HDL-C and triglycerides were significantly different between the two groups. The massive production of proinflammatory cytokines at the site of an infection is known to cause proinflammatory tissue damage and worsen disease conditions. 37 H. pylori is a pathogen that causes chronic infections in a specific way in order to ensure its survival. The regulation of the NOD-like receptor family, pyrin domain-containing 3 (NLRP3) inflammasome in microbial infections is an emerging area that requires further research. When immune cells, particularly macrophages and dendritic cells, become infected with H. pylori, the increased IL-1 production caused by activation of the NLRP3 inflammasome causes an inflammatory response such as neutrophil infiltration and decreased gastric acid secretion, allowing the bacteria to colonize and survive in the gastric tissue for an extended period of time.38,39 H. pylori infection triggers the release of the orexigenic hormone, ghrelin, which regulates the appetite. 36 Obese/overweight individuals have been shown to exhibit reduced circulating levels of ghrelin, indicating a potential association between ghrelin and obesity. 38 In addition, H. pylori-positive individuals have been shown to exhibit reduced serum levels of leptin.35,39 Reduced leptin levels induce appetite, which leads to overfeeding, resulting in overweight and obesity. 40
Reactive oxygen species production-mediated oxidative stress plays an important role in obesity and H. pylori infection pathogenesis. 14 8-OHdG is potentially the most useful oxidative DNA damage marker as a result of the DNA base modification caused by the oxidation of deoxyguanosine. 39 This lesion is both mutagenic and abundant, which makes it a critical DNA damage.14,41 This current study demonstrated a significant difference between serum 8-OHdG levels of the H. pylori-negative and H. pylori-positive groups. These current results agreed with those of a previous study that demonstrated a significant association between HbA1c and 8-OHdG levels in H. pylori-positive patients with type 2 diabetes mellitus. 41 The current study demonstrated that in patients with H. pylori infection, the 8-OHdG levels had a linear correlation with BMI. H. pylori-positive patients with a high BMI exhibited higher levels of 8-OHdG, which could be attributed to elevated ROS production.
This study had several limitations. First, the cross-sectional design limited causal inferences. Secondly, as the study was limited to the Makkah region, the findings cannot be generalized to all Saudi Arabian regions. Thirdly, the serology-based diagnosis of H. pylori infection has some inherent limitations, including the inability to distinguish current from previous infection. Despite this limitation, serodiagnosis is a suitable and reliable noninvasive technique that can be used as a first-line screening tool for the detection of H. pylori infection. Fourthly, when considering risk factors for being overweight or obese, various other sociodemographic characteristics, diet, physical activity and concomitant illnesses should be considered. Finally, the study did not assess the use of sex as factor in the association of H. pylori, obesity and 8-OHdG levels.
In conclusion, obese individuals in the current study exhibited higher H. pylori prevalence than individuals with a lean BMI. H. pylori infection in the study cohort was significantly associated with altered triglyceride and HDL-C levels, which indicates dyslipidaemia. Serum 8-OHdG is a useful indicator of disease severity or the degree of oxidative stress in H. pylori-positive obese individuals. Elevation in BMI increased the risk of H. pylori infection. These current results might be helpful in designing appropriate treatment modalities for H. pylori-positive patients with a high BMI.
Footnotes
Acknowledgements
The authors thank Atheer Abdulaziz Alzubedi, Haneen Salah Almasoudi, Aisha Abullah Alharbi, Alaa Ahmed Suliman, Razan Mohammed Sulimani, Afnan Ali Al-Yamani, Malak Hassan Alfaifi, Shatha Abdulaziz Haroun, Amjad Mashhour Nasser Altijani and Alaa Abdullah Abujbal for their efforts in collecting samples and recording their data.
Declaration of conflicting interest
All authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors.