
Abstract
Objective
Ozone is a colorless gas used as a disinfectant and to treat diseases by limiting the effects of bacteria, viruses, fungi, yeast, and protozoa. In this study, we investigated the clinical efficacy of ozonated water lavage and physiological saline irrigation combined with vacuum-sealed drainage (VSD) in the treatment of chronic osteomyelitis.
Methods
Eighteen patients (14 men and 4 women) with chronic osteomyelitis in the limbs (tibia: 13 cases; femur: 4 cases; humerus: 1 case) admitted to our hospital between April 2012 and October 2018 were selected. The patients were aged 9 to 52 years, with a mean age of 31 years. All patients underwent ozonated water lavage and physiological saline irrigation combined with VSD negative pressure closed drainage during hospitalization. The patients were followed up for 18 to 84 months, with a mean of 31 months.
Results
Osteomyelitis recurred in only one case of nonunion. The length of hospitalization was 18 to 29 days, with a mean of 21 days.
Conclusions
A combination of ozonated water lavage, physiological saline irrigation, and VSD provided good clinical effects in the treatment of chronic osteomyelitis, and thus, is recommended for such treatment.
Keywords
Introduction
Chronic osteomyelitis is considered one of the most stubborn diseases in the medical profession and is sometimes termed an “undead cancer.” Although the antibacterial activity of new-generation antibiotics is increasing, and surgical methods continue to improve, the recurrence rate of chronic osteomyelitis is still as high as 20% to 30%. 1 The treatment of chronic osteomyelitis is so difficult and long that patients suffer greatly both physically and psychologically. Moreover, the treatment carries a heavy economic burden for families and society.1–3 Therefore, in the treatment of chronic osteomyelitis, it is of important clinical and social significance to shorten the course of treatment, improve the cure rate, and reduce the disability rate. As an effective method of treating osteomyelitis, vacuum-sealed drainage (VSD) has been widely used clinically, but problems, such as infection and drain obstruction during treatment remain problematic. 4 Recently, researchers have found that ozone plays an important role in the treatment of skin wounds. European countries have been using medical ozone to treat diabetic foot ulcers, traumatic wounds, skin ulcers, and even stroke, ulcerative colitis, arthritis, and intervertebral disc herniation. 5 Ozonated water, which is formed by dissolving ozone in water, has a strong oxidizing effect and achieves its bactericidal activity by destroying microorganisms’ cell membranes. Upon sterilization, ozone self-decomposes and is reduced to oxygen without producing residual or secondary pollution; therefore, it is known as a “green element.” 6
Our hospital has used ozonated water lavage and physiological saline irrigation combined with VSD to treat chronic osteomyelitis and achieved good results, which we report below.
Materials and methods
Inclusion criteria: (1) patients with fracture site osteomyelitis after limb fracture surgery; or (2) patients with hematogenous osteomyelitis of the extremities advancing to chronic osteomyelitis; and who (3) failed to respond to conservative treatment, and (4) volunteered for the study. Exclusion criteria: (1) immunocompromised or recent glucocorticoid use; (2) patients with major organ or peripheral vascular neuropathy who were unable to tolerate surgery; (3) patients with poor glycemic control affecting wound healing; and (4) patients who were lost to follow-up.
General information
From April 2012 to October 2018, patients with chronic osteomyelitis of the limbs who were treated in our hospital were selected for this study. The research was approved by the Medical Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University (approval number: K202004-04), and the patients and their families gave written informed consent.
Samples of pus were taken from the deep part of the sinus cavity before surgery for bacterial culture and drug sensitivity testing. During the subsequent clinical treatment, antibiotics were used according to the drug sensitivity results. Each patient's X-ray and computed tomography (CT) images were analyzed preoperatively to understand the localized bone mass, dead bone, closed medullary cavity, and soft tissue involvement (Figure 1: A–F). For patients with long-term sinus discharge, further sinusography and methylene blue sinus staining were performed to reveal the sinus ostium, and the direction and scope of travel. To minimize errors owing to operator factors, all patients included in this study underwent operation by a single surgical team, and postoperative treatment and follow-up were also performed by the same team.

The patient was a 34-year-old man with a traumatic fracture. (a, b) The images show a complex open fracture of the right femur with a bone defect and an open fracture of the right tibia and fibula with vascular and nerve damage. The right tibia was amputated below the knee. (c, d) An osteotomy was performed to shorten the tibial amputation site, and part of the amputated tibia was used for mid-femoral bone grafting. X-ray images show the femur 16 months later. (e, f) After 17 months, traditional intramedullary canal irrigation and drainage was performed. X-ray images show the femur 18 months after the initial surgery.
VSD materials and devices
Commercially available VSD dressings were obtained from Wuhan VSD Medicine and Technology Co., Ltd. (Wuhan, China). The main component of the VSD dressing is polyethylene alcohol-hydrated seaweed salt foam, which contains multiple lateral drains. The materials are non-toxic, non-tissue-irritating, non-immunogenic, and cause no skin sensitization. The VSD system uses a portable vacuum device.
Preparation of the ozonated water
Ozonated water with a concentration of 10 mg/L was prepared using an ozone generator (Medozon standard pressure medical ozone treatment generator; Herrmann Apparatebau GmbH., Elsenfeld, Germany) at room temperature (20°C) by injecting double-distilled water into the water storage tank (capacity: approximately 2000 mL) of the ozone generator. The obtained ozonated water was used immediately.
Surgical procedure
An incision was made where the lesion could be removed easily, the soft tissue was in relatively good condition, and the position was good for wound coalescence. The osteomyelitis sinus was completely removed, and internal fixation devices were replaced with external fixation frames. Complete excisional debridement of all devitalized tissues, including skin, subcutaneous tissue, muscle, periosteum, and bone, was performed to achieve the goal of a healthy wound in preparation for ozone irrigation. During debridement, surgical fenestration was first created on one side of the bone cortex, with a width of 1.5 cm and effective exposure of the chronic osteomyelitis area. During bone cortex fenestration, an electric drill was used to drill holes in the cortical lesion in a strip shape and then a sharp osteotome was used to connect these holes to prevent fractures and to reveal the lesion in the medullary cavity.
While drilling, water was dripped over the drill bit with a syringe to lower the temperature to prevent damage to the bones and avoid affecting the blood supply with the heat from the drill. The granulation tissue in the lesion was thoroughly removed, as well as the dead bone and the surrounding sclerotic bone tissue, until fresh blood was seen. Cortical bleeding, described as the “paprika sign”, was accepted as an indication of vital osseous tissue. 7 A larger hole was drilled 2 cm away from the normal bone of the upper or lower end of the bone window and was used as the pouring hole, and the drip tube was placed inside the pouring hole through the healthy skin on the incision edges to run through the medullary cavity in the lesion area. Then a fine suture was used to help fix the tube to the skin to prevent it from sliding, and the drip tube was tightly sutured to the skin at the entrance to prevent the perfusion fluid from exuding. Afterwards, we drilled holes with a 3.0-mm drill bit into the bone cortex on both sides of the bone window, deep enough to reach the medullary cavity, controlling the temperature while drilling (Figure 2: A–C).
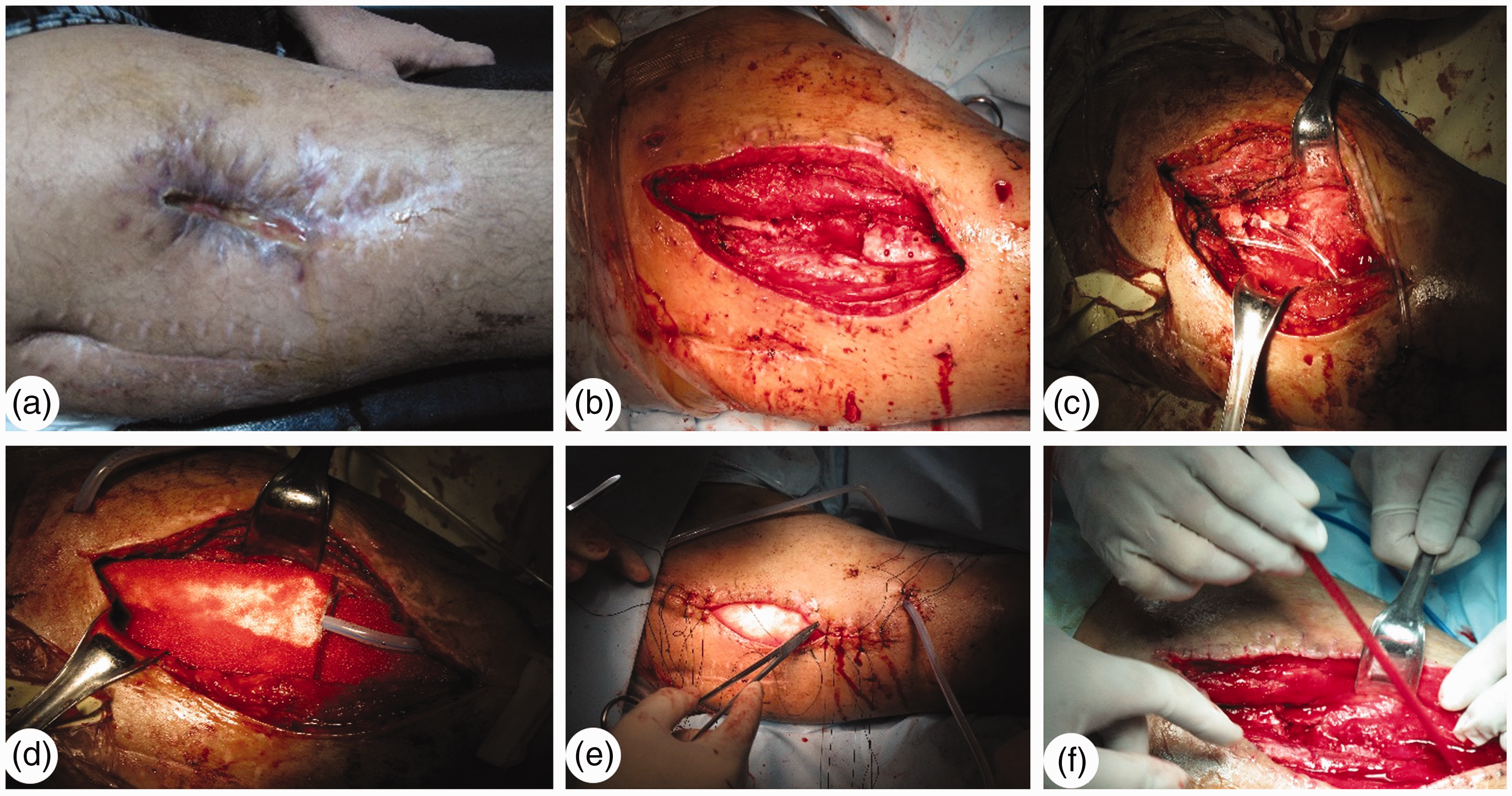
The same patient as in Figure 1, 19 months after injury. Ozonated water irrigation and physiological saline lavage were applied in combination with VSD treatment. (a–e) The first operation. (f) The fourth operation.
The medullary cavity was then lavaged repeatedly with physiological saline, and bone debris and blood clots were completely cleared to prevent luminal obstruction. A VSD dressing was placed in the medullary cavity of the lesion and on the cortical surface to completely fill the window to facilitate the drainage of fluid and promote the growth of fresh granulation tissue (Figure 2: D and E). If the lesion covered a large area, we sutured VSD dressings together and connected the silicone tubes in a Y shape. We cleaned and dried the skin around the wound twice using ethanol ointment and dry gauze, and then covered the entire wound with a biological semi-permeable membrane. The coverage exceeded the margin of the incision by ≥5 cm, and the irrigation tube was also sealed properly to the membrane to prevent exudation of the physiological saline. A sample was taken for bacterial culture and sensitivity testing before debridement and wound closure, to guide postoperative intravenous anti-inflammatory treatment.
Postoperative management
Upon return to the ward, the patient’s drip tube with the physiological saline bottle was connected immediately to a VSD suction device for continuous irrigation.
To facilitate control of the drip rate of the perfusion irrigation by the nursing staff or patients’ families, 500 mL isotonic saline was flushed hourly on the first day, every 2 hours on the second day, every 3 hours on the third day, and continuing to 500 mL every 8 hours on the seventh or eighth days. To increase the patients’ comfort and tolerance during physiological saline flushing, normal physiological saline was heated to 40°C to 45°C. Starting from the second day after surgery, ozonated water was freshly prepared at a concentration of 10 mg/L.8–10 The ozonated water was irrigated through the water inlet pipe, the negative-pressure drainage was turned off during the irrigation, the VSD material and the wound surface were immersed in the lavage solution for 3 minutes, and the negative-pressure drainage was then turned on for 1 minute. This cycle was repeated an additional three times over a 16-minute period, and the entire procedure was repeated 12 hours later. Thus, ozone lavage, and subsequent saline irrigation and VSD drainage was performed eight times per day. It should be emphasized that the area must be irrigated with ozonated water, not rinsed, and all wounds and VSD materials must be soaked. Before removing the VSD dressing, lavage and flushing was stopped, and the wound was allowed to continue to drain for l day under negative pressure to aspirate any residual liquid from the wound.
After the first 7 to 8 days of drip irrigation, ozone water irrigation, and VSD, another operation was needed to replace the VSD dressing. In the second operation, it was necessary to decide whether to continue to use normal saline irrigation combined with VSD negative-pressure suction or to use VSD material, negative-pressure suction, and ozone irrigation to treat the wounds according to each patient’s condition. In the second operation, 14 of the 18 patients were treated with ozone irrigation and VSD materials instead of normal saline irrigation; that is, the original function of the VSD materials was restored, and ozone water irrigation was continued. For the remaining four patients with severe illness, we used the same method as in the first operation and continued to flush with both saline and ozonated water. However, for these four patients, the daily volume of saline in the second round was generally controlled at approximately 2000 mL, rather than a large amount of irrigation, owing to better wound recovery after the first operation. During the third operation, four patients received VSD combined with ozonated water irrigation. Thus, the four patients with severe illness received an additional week of treatment with saline and ozonated water compared with the other patients.
For patients who underwent direct placement of the VSD, lavage with ozonated water and a small amount of saline solution four times a day were important to avoid obstruction of the VSD dressings and drains. After removing the VSD dressing (during a third operation in 14 patients and a fourth operation for the four more seriously ill patients), we found fresh, reddish granulation tissue in the wound, which was smooth and dense, with no trace of secretions indicating infection (Figure 2: F). The wound was sutured as directly as possible. For adult patients, 1 g of vancomycin hydrochloride was placed in the medullary cavity and surrounding soft tissues before suturing and placing a drain in the surgical area. The drain was not removed until the patient's local drainage volume was less than 30 mL. Before removing the drain, it was repeatedly vacuumed using a 30-mL syringe so that the drainage was complete, to avoid leaving any residual fluid in the wound. If direct suture was not possible, a flap was used to repair the wound, and the area of the flap was grafted with split-thickness skin grafting.
Results
The patients’ detailed demographic pre- and postoperative data are shown in Table 1. Fourteen patients were men and four were women ranging in age from 9 to 52 years, with a mean age of 31 years. Three cases developed from acute hematogenous osteomyelitis of the tibia, one case developed from acute hematogenous osteomyelitis of the femur, and the following developed from fractures: internal fixation of an open femoral fracture (n = 3), internal fixation of an open tibial fracture (n = 3), external fixation of an open tibial fracture (n = 4), internal fixation of a closed tibial fracture (n = 3), and internal fixation of a closed humeral fracture (n = 1). The disease course ranged from 5 to 110 months, with a mean of 14 months. Among the 18 patients, 11 had been treated with traditional intramedullary canal irrigation in other hospitals; some even underwent five successive operations. The patients’ main symptoms were local swelling and redness and sinus formation (part of the bone and internal fixation were exposed) accompanied by purulent exudation.
The patients’ detailed demographic data.

We did not change the VSD wound dressing during the entire period using VSD. Among the 18 cases, there were no instances of complications, such as deep venous thrombosis in the limbs, generalized or local toxicity, allergic reaction, hemorrhage, or other discomfort.
After removing the VSD dressing, one significant finding was that the medullary cavity and the soft tissue around it were filled with fresh granulation tissue, as was the soft tissue in the musculature around the bone. The wound was sutured directly or repaired using a skin flap graft. Among the 18 patients, seven wounds were sutured directly, six were covered by an adjacent double-pedicle skin flap, two were covered by the medial head of the gastrocnemius muscle, and three were covered by a sural neuro-lesser saphenous veno-fasciocutaneous compound flap.
All 18 patients were followed-up for 18 to 84 months, with a mean of 31 months (Figure 3: A–F). Except for one case of nonunion, there were no recurrences of osteomyelitis. The length of hospitalization was 18 to 29 days, with a mean of 21 days.

The same patient as in Figure 1 20 months (a, b), 3 years (c, d), and 7 years (e, f) after initial treatment.
Discussion
Chronic osteomyelitis recurs frequently, causing poor blood supply across long bones, and owing to stenosis or occlusion of the medullary cavity, it is extremely difficult to achieve penetration and saturation with antibiotics. Therefore, full debridement, removing dead bone, and debriding the medullary cavity, combined with irrigation is commonly used in clinical practice.11–13
Since the mid-1990s, when VSD technology was invented by Fleischmann et al.14,15 in Germany, the treatment of soft tissue defects and/or wound infection has achieved good outcomes. VSD treatment can provide a humid environment for the wound, which increases local blood flow, reduces bacterial growth, accelerates the growth of granulation tissue, narrows the wound, and promotes wound healing, as well as enhancing the quality of the wound healing.16,17 Kumar et al. 18 believe that VSD provides a new and effective method for the treatment of chronic osteomyelitis. Traditional medullary tube irrigation for osteomyelitis treatment has many limitations. The limited drainage range of the drain means that the lesion cannot be drained thoroughly, leading to residual irrigation fluid and secretions remaining in the wound. Because the drain is easily obstructed, it must be removed prematurely, which affects the treatment efficacy. If VSD material is used alone to treat osteomyelitis, the VSD material dries out quickly during treatment, which affects drainage efficacy. Clinically, the drainage effect of VSD materials is better under a properly humid environment. However, some studies have reported that sealing the wound with negative pressure may form an anoxic environment, promoting the reproduction of anaerobic bacteria, which is likely to cause mixed infection and aggravate the patient's condition. In addition, using negative pressure in ischemic or hypoxic wounds aggravates the wound tissue and may even cause vascular embolism in severe cases. 19
Medical ozone is a mixture of ozone and pure oxygen prepared from medical pure oxygen. Ozone is a strong oxidation agent and can quickly kill bacteria through redox reactions. It is also an effective and strong bactericide with a broad spectrum,6,20 acting by destroying microbial cell membranes through oxidation. Once dissolved in water, ozone has a stronger bactericidal disinfection and decomposition effect. Its broad spectrum enables it to quickly and effectively kill bacteria, fungi, and viruses, 21 especially when antibiotics fail to control multi-drug resistant bacteria, and it has a high bactericidal rate without inducing drug resistance or dependence.22–24 The metabolite of ozonated water is oxygen, which can improve the hypoxic state of a wound and increase aerobic metabolism, thereby promoting angiogenesis and granulation tissue formation, and providing sufficient energy for cell proliferation, further increasing the clinical effect. 25 Ozonated water irrigation can effectively increase the partial pressure of oxygen in the wound tissue, while oxygen can significantly inhibit bacterial reproduction while enhancing the activity of phagocytic cells, effectively improving the bacterial clearance rate.26,27
The concentration of ozonated water is controlled at 10 mg/L for the following reasons: (1) Ozonated water at concentrations of 10 to 20 mg/L is sufficient to kill most pathogenic bacteria. 8 (2) Animal studies 28 have shown that ozonated water with a concentration <33 mg/L will not cause bodily damage. (3) To ensure the safety of clinical applications, Jiang et al. 29 suggested when combining VSD to treat infectivity, a lower concentration of ozonated water should be chosen first, and depending on the irrigation effect, the ozonated water concentration and irrigation frequency can then be adjusted according to the clinical effect. Moreover, Ma et al. 30 confirmed that the combined application of VSD material and 10 mg/L ozonated water will not cause skin irritation and is biocompatible and safe. Yin et al. 31 also found that soaking the VSD material in ozonated water at a concentration of 10 mg/L for 20 minutes did not change its physical properties. Therefore, it is theoretically feasible to treat infected wounds using VSD technology combined with 10 mg/L ozonated water.
According to previous results, the combination of ozonated water lavage, physiological saline irrigation, and VSD can not only solve a series of problems associated with traditional tube irrigation, but also promote the growth of fresh granulation tissue and improve local blood circulation. Moreover, sterilization by ozonated water irrigation promotes angiogenesis and the formation of granulation tissue.
Opening the full length of a long bone could allow new healthy granulation tissue to fill the medullary cavity, thereby improving blood flow and nutritional conditions in the long bone. This approach can also further prevent recurrence and restore limb function. The width of the opening window is dependent on bone thickness, and generally should not exceed 1/3 of the bone circumference. After opening, the medullary cavity is completely exposed to ensure complete contact between the VSD dressing and the wound surface. After the lesion is cleared and the medullary cavity is penetrated, multiple holes must be drilled in the bone cortex near the opening to: (1) increase the effect of drainage and prevent the medullary cavity from closing again; 2) induce the growth of fresh granulation tissue and new capillaries from the drilled holes, thereby further improving blood flow to the local bone in chronic osteomyelitis lesions; and 3) permit transplanting bone grafts, especially for patients who develop osteomyelitis within a short period of time after bone fracture.
The shortcomings of this study are the following: (1) No control group (traditional treatment group as a cohort group) was established to compare with the treatment group (ozonated water treatment group). Having a control group may provide more valuable data regarding the effectiveness of the ozonated water treatment. (2) This was a retrospective study with a small sample size; therefore, statistical analysis was not feasible. A prospective case–control study will be performed in the future to better investigate the effectiveness of ozone therapy. (3) Future multicenter studies with larger sample sizes are required to compensate for the shortcomings of this study.
In summary, traditional saline lavage combined with ozonated water irrigation and VSD for chronic osteomyelitis can significantly improve the hypoxic and ischemic state of wound tissue, increase granulation tissue coverage and bacterial clearance, and reduce the possibility of an obstructed drain postoperatively. Thus, this combined treatment is recommended for the treatment of chronic osteomyelitis.
Footnotes
Author contributions
Tayierjiang Yasheng, Aini Mijiti, and Aihemaitijiang Yusufu designed the study and drafted the manuscript. Maimaiaili Yushan, Zhenhui Liu, and Yanshi Liu collected the data and performed the analyses. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.