
Abstract
Objective
To explore the diagnostic role of phosphatidylethanolamine binding protein 4 (PEBP4) in patients with chronic kidney disease (CKD) receiving nursing interventions.
Methods
ELISA was used to evaluate serum PEBP4 levels. Receiver-operating characteristic curve analysis was used to assess diagnostic accuracy. Spearman correlation analysis was used to assess the relationships between PEBP4 levels and biochemical indexes.
Results
Serum PEBP4 was high in CKD patients compared with healthy individuals. PEBP4 levels were positively correlated with pathological stage in CKD patients. PEBP4 had higher sensitivity for diagnosis of CKD than common indexes including blood urea nitrogen, creatinine and C-reactive protein. Among CKD patients treated with calcium channel blockers, serum PEBP4 levels declined notably and were associated with concentrations of K+, Na+, Cl− and Ca2+. Nursing interventions significantly decreased serum PEBP4 levels. A significant association between serum PEBP4 level and ionic concentration was observed in CKD patients receiving nursing interventions.
Conclusions
This prospective study demonstrated that PEBP4 level might represent an effective diagnostic biomarker in CKD patients. PEBP4 also acted as a valuable care compliance factor for determining the necessity for nursing interventions. Nursing interventions restored ion channel function and subsequently resulted in decreased PEBP4 levels and proteinuria.
Keywords
Introduction
Chronic kidney disease (CKD) is defined as the presence of kidney damage or kidney dysfunction for more than 3 months, irrespective of diagnosis. 1 CKD is a worldwide public health concern and seriously affects patient quality of life. 2 CKD can be divided into five stages based on estimated glomerular filtration rate (eGFR) or albuminuria. 3 Progression of CKD is highly variable and is affected by risk factors including sex, hypertension, diabetes, obesity and genetic factors. 4 CKD is associated with adverse outcomes such as kidney failure, cardiovascular disease, and premature death. 5 Current medical interventions for CKD are limited and are aimed at delaying progression and preventing negative outcomes. 6 Although treatment of early-stage CKD can delay progression and kidney failure, 7 there is a lack of sensitive and specific biomarkers for early diagnosis and treatment of CKD. 8 Therefore, identification of novel biomarkers to improve diagnostic efficiency, surveillance, and treatment of CKD is an urgent priority.
The most commonly used index of kidney function is eGFR. However, timeliness is a key constraint. 9 CKD clinical stage is classified according to eGFR and urine albumin-to-creatinine ratio. 10 Consequently, serum creatinine (CREA), cystatin C (CysC), and proteinuria are used to classify the different pathological stages of CKD. 11 However, there are a number of limitations to this strategy. Measurement of CREA requires stable kidney function and is not suitable for CKD patients with large muscle masses or elderly patients. 12 Compared with CREA, the clinical use of CysC detection remains very limited worldwide. 13 Because of persistently high blood urea nitrogen (BUN) levels after the successful resolution of kidney injury, measurement of BUN is not suited to distinguish the stages of CKD. 14 Optimal management of CKD is effective in reducing the burden of CKD. 15 Nursing interventions play a vital role in improving the symptoms of CKD patients by providing education, monitoring, and support. 16 Improvement in population understanding of CKD contributes to kidney disease prevention and improved quality of life. Culturally consistent care is beneficial for the recovery of patients with kidney disease. 17 Previous studies have indicated that phosphatidylethanolamines are correlated with the development of CKD. 18 Phosphatidylethanolamine binding protein 4 (PEBP4) is a member of the phosphatidylethanolamine binding protein family. 19 Overexpression of PEBP4 is related to the development, invasion, and metastasis of a variety of tumors, 20 suggesting that PEBP4 may represent a new diagnostic marker and therapeutic target. Upregulation of PEBP4 attenuated the anti-tumor effect of rituximab in lymphoma cells. 21 PEBP4 activation diminished the sensitivity of tumor cells to radiotherapy and chemotherapy by activating the PI3K/AKT signaling pathway. 20 Additionally, a recent study showed that urine PEBP4 levels were significantly increased in patients with IgA nephropathy, implying that PEBP4 is involved in the progression of kidney disease. 22 However, the clinical value of PEBP4 in CKD has yet to be explored.
Herein, we found that serum PEBP4 levels were elevated in CKD patients and could thus represent a specific marker for diagnosis of CKD. Meanwhile, calcium channel blockers and/or care compliance decreased serum PEBP4 levels with coincident changes in ion channel function. Collectively, our data indicated that PEBP4 may be a diagnostic and prognostic indicator in CKD patients.
Materials and methods
Guidelines
This study complied with STARD guidelines. 23 The study was approved by the ethics committee of Zhejiang Provincial People’s Hospital (20180810).
Subjects
This was a prospective clinical research study. CKD patients were enrolled and classified into five stages based on eGFR. To exclude patients with postoperative CKD and kidney transplantation, all patients were verified through blood cultures. Subjects with negative results were enrolled. Detailed information including recruitment date, number, age, gender, stage, and treatments received were recorded. Clinical information of subjects are presented in Table 1. Written informed consent as in the previous study 24 was obtained from each patient.
Demographic characteristics of patients.
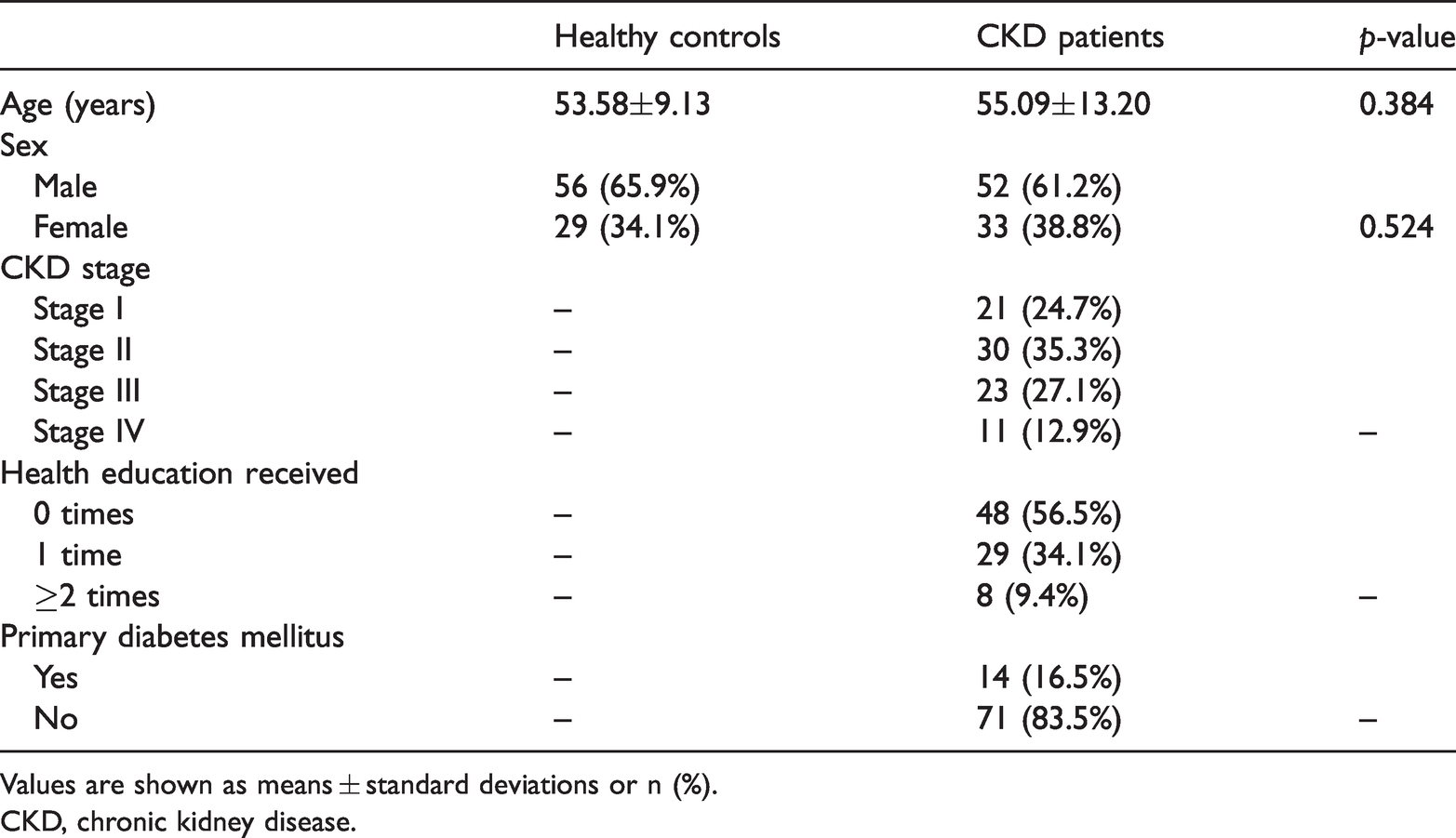
Values are shown as means ± standard deviations or n (%).
CKD, chronic kidney disease.
ELISA assay and biochemical analysis
Blood samples were collected in coagulant tubes and allowed to stand for 3 hours at room temperature. Serum was obtained by centrifugation at 1000 ×g for 2 minutes at 4°C. Levels of serum PEBP4 were measured using an ELISA kit (Cloud-Clone, Wuhan, China). The absorbance in each sample was measured at 450 nm using a microplate reader (Molecular Devices, San Jose, CA, USA). Levels of BUN, CREA, CysC and C-reactive protein (CRP) as well as concentrations of sodium (Na+), chloride (Cl−), calcium (Ca2+) and potassium (K+) were analyzed using a COBAS C501 chemistry analyzer (Roche Diagnostics, Risch-Rotkreuz, Switzerland).
Correlation analysis
After determining levels of PEBP4 and biochemical indexes, information was collected on care compliance among CKD patients. Spearman analysis was performed to explore correlations among PEBP4 levels, biochemical indexes, and care compliance. Spearman correlation coefficients of R>0 represented positive correlation and coefficients of R<0 represented negative correlations.
Receiver-operating characteristic (ROC) curve analysis
ROC curve analysis was used to assess the diagnostic relevance of PEBP4, CREA, BUN and CRP. Sensitivity was presented as the area under the curve (AUC) and was calculated using the rank sum test. Larger AUCs reflected higher diagnostic accuracy.
Intervention guidelines
Enrolled CKD patients were divided into two groups: routine care control and special care intervention group. Intervention guidelines were set out and observed regularly. Complete compliance, partial compliance and non-compliance were assessed, and the patient compliance rate was calculated. Differences in disease cognition, prescribed medications, medication times, and readmission rates in the two group were recorded and calculated. Correlations between PEBP4 and care compliance were analyzed using Spearman analysis.
Statistical analysis
All data were presented as means ± standard deviations. Statistical analyses were performed using SPSS version 20 (IBM, Armonk, NY, USA). Two-sided values of p<0.05 were considered significant and values of p<0.01 were considered significant. We did not perform a sample size calculation, and the limited number of samples may have affected the statistical significance of the results.
Results
PEBP4 level is positively correlated with inflammatory indexes and clinical stage in CKD patients
Expression of PEBP4 was explored in 85 healthy and 85 CKD patients. Healthy subjects included 56 men and 29 women with a mean±SD age of 53.58±9.13 years. The CKD patients included 52 men and 33 women with a mean±SD age of 55.09±13.20 years. There were no differences in age or gender between healthy controls and CKD patients (Table 1). Among CKD patients, 48 did not receive health education, 29 received health education once and eight patients received health education two or more times. Fourteen CKD patients were diagnosed with primary diabetes mellitus.
Levels of BUN, CREA, CysC and CRP in CKD patients were significantly increased by three-fold (23.20±13.23 mmol/L vs 7.00±6.33 mmol/L, p<0.001), six-fold (607.16±531.45 µmol/L vs 98.26±103.95 µmol/L, p<0.001), four-fold (4.33±2.30 ng/mL vs 0.90±0.83 ng/mL, p<0.001) and 2.7-fold (17.39±9.36 ng/mL vs 6.43±6.42 ng/mL, p<0.001), respectively (Fig. S1 and Table S1). Interestingly, ELISA results showed that serum PEBP4 levels in CKD patients were significantly higher than those of healthy controls (p<0.001) (Figure 1a). Correlations between PEBP4 and BUN, CREA, CysC, and CRP levels were significant (p<0.001) yielding Spearman correlation coefficients of 0.511, 0.550, 0.544, and 0.464, respectively (Figure 1b–e). The mean levels of PEBP4 according to pathological stage were as follows: pathological stage I, 537.76±218.69 ng/mL (n=21); pathological stage II, 824.46±149.29 ng/mL (n=30); pathological stage III, 910.49±248.39 ng/mL (n=23); and pathological stage IV, 1063.51±324.15 ng/mL (n=11). Combined with Pearson’s analysis, this result shows that levels of PEBP4 were positively correlated with advancing pathological stage of CKD patients (p<0.01) Table 2. Thus, serum PEBP4 might act as a potential prognostic indicator for CKD in addition to common detection indexes (BUN/CREA/CysC/CRP).
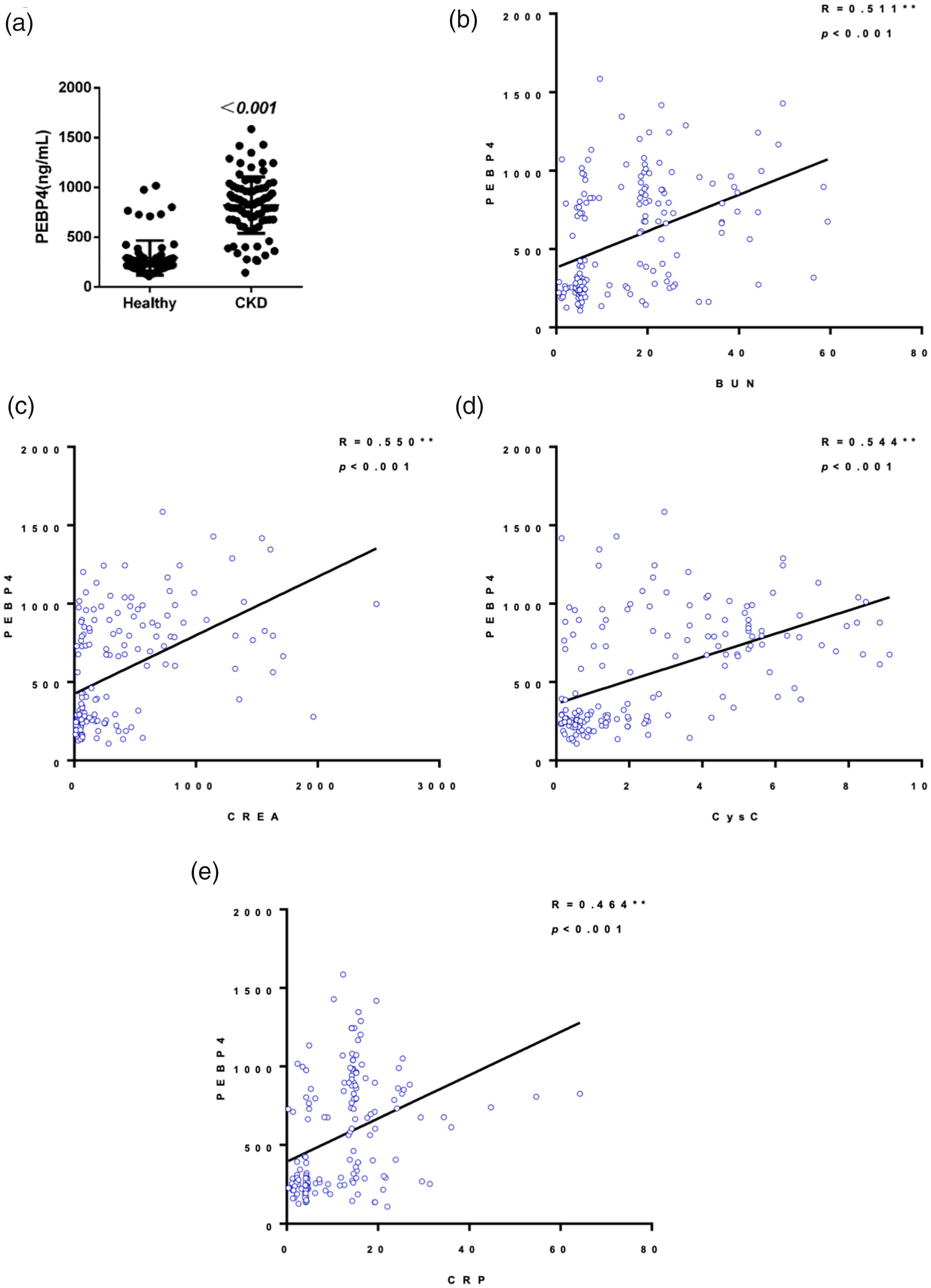
Association between serum PEBP4 levels and biochemical indexes in CKD patients and healthy controls. (a) Serum PEBP4 levels were measured by ELISA in advanced CKD patients and healthy controls. Correlations between PEBP4 and BUN (b), PEBP4 level and CREA (c), PEBP4 and CysC (d), and PEBP4 and CRP (e) were analyzed using Spearman’s method. The blue circles represent healthy controls and the green circles represent CKD patients.
PEBP4 levels in patients with CKD.

**Significant.
CKD, chronic kidney disease; SD, standard deviation.
High diagnostic sensitivity of PEBP4 in CKD patients
Measurement of serum BUN, CREA and CRP levels can be used to diagnose CKD. Next, we assessed the potential diagnostic value of PEBP4 levels in CKD patients using ROC curve analysis. ROC curve analyses of the common diagnostic biomarkers BUN, CREA and CRP were also conducted as a reference. As shown in Figure 2, the AUC value for PEBP4 was significantly greater than that for CRP (0.938 vs 0.875, p<0.001) (Figure 2a). The AUC values for BUN and CREA were only 0.894 and 0.887, respectively (Figure 2b,c). Thus, the specificity of PEBP4 for diagnosis of advanced CKD patients was higher than those of common indexes including BUN, CREA and CRP.

ROC curve analysis of PEBP4 and other CKD biomarkers. (a) Differences in the ROC curves for PEBP4 and CRP. (b) Differences in the ROC curves for PEBP4 and BUN. (c) Differences in the ROC curves for PEBP4 and CREA. The green lines represents the ROC curves for CRP, BUN and CREA, respectively. The blue line represents the ROC curve for PEBP4. The yellow line represents the reference line.
Calcium channel blocker treatment decreases serum PEBP4 levels
Nifedipine, a calcium channel blocker, is used to treat patients with CKD. In CKD patients, levels of K+ were increased by 10% (4.40±1.45 mmol/L vs 3.94±1.49 mmol/L, p=0.044). Similarly, levels of Na+, Cl−, and Ca2+ were decreased by approximately 5% (137.39±6.10 mmol/L vs 142.57±16.83 mmol/L, p=0.008; 100.81±6.11 mmol/L vs 105.99±7.39 mmol/L, p<0.001; 2.30±0.66 mmol/L vs 2.58±1.06 mmol/L, p=0.040, respectively) (Figure 3a–d and Table S1). Following treatment with nifedipine, decreased levels of K+, Na+, Cl− and Ca2+ were restored (Figure 3a–d). Increased levels of serum PEBP4 in CKD cohorts were also inhibited by administration of calcium channel blockers (Figure 3e). Correlational analysis indicated that serum PEBP4 level was significantly positively correlated with K+, but negatively associated with Na+, Cl− and Ca2+ (p<0.001) (Figure 3f–i). These data confirmed the therapeutic relevance of serum PEBP4 in CKD patients treated with nifedipine.

Correlation between serum PEBP4 levels and ion channel function in CKD patients treated with calcium channel blocker. Levels of K+ (a), Na+ (b), Cl− (c) and Ca2+ (d) in healthy controls, CKD patients, and CKD patients treated with calcium channel blockers. (e) Serum PEBP4 levels in healthy controls, CKD patients, and CKD patients receiving calcium channel blockers. Correlations between PEBP4 levels and K+ (f), between PEBP4 levels and Na+ (g), between PEBP4 levels and Cl− (h) and between PEBP4 levels and Ca2+ (i) were analyzed using Spearman’s method. The blue circles represent healthy controls and the green circles represent CKD patients.
Care compliance reduces serum PEBP4 levels in CKD patients
Next, the relationship between PEBP4 and care compliance was assessed. Forty-three patients received nursing interventions while the remaining patients received usual care. Nursing interventions robustly reduced levels of BUN, CREA, CysC and CRP compared with CKD patients treated with usual care (Figure 4a–d). A significant decline in serum PEBP4 level was also observed in patients receiving nursing interventions compared with CKD patients given usual care (Figure 4e). The disease cognition rate was 83.4% (36/43) in the nursing intervention group compared with only 64.3% (27/42) in the control group (p=0.041). The rate of prescribed medication administration in the intervention group was 86.0% (36/43), significantly higher compared with the control group (57.1%, 24/42) (p=0.003). Medication times and readmission rates were 90.7% (39/43) and 95.3% (41/43), respectively, in the intervention group, significantly higher compared with the control group (64.3%, 27/42 and 54.8%, 23/42, respectively; p=0.003 and p<0.05, respectively) (Table 3). Using Spearman correlation analysis, we found a significant inverse correlation between PEBP4 levels and care compliance in CKD patients (R=−0.366, p<0.001) (Figure 4f). These data imply that PEBP4 levels may be a key index for CKD patients receiving nursing care.
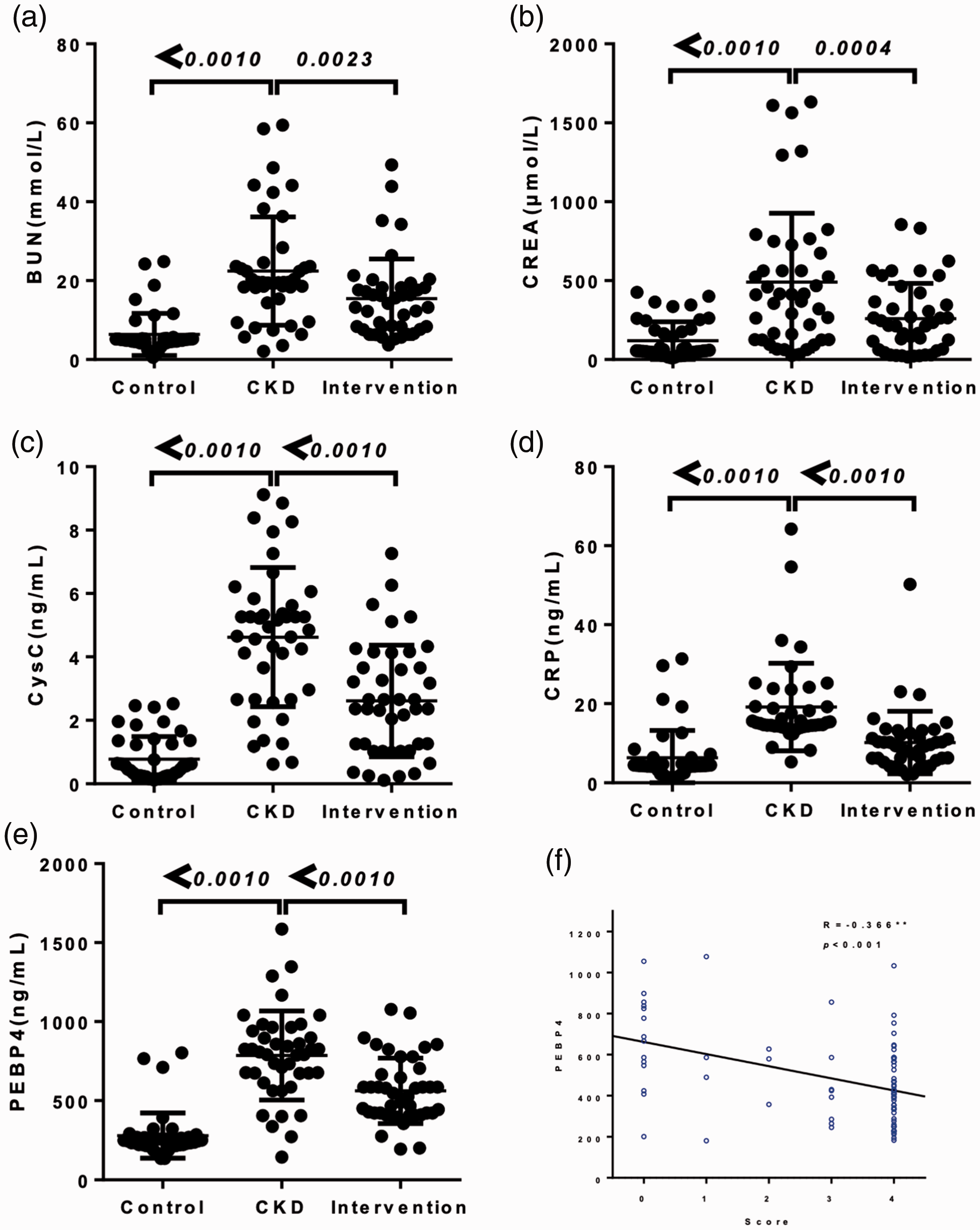
Effect of care compliance on serum PEBP4 levels in CKD patients. Levels of BUN (a), CREA (b), CysC (c), CRP (d) and serum PEBP4 (e) in healthy controls, CKD patients, and CKD patients receiving nursing interventions. (f) Correlations between PEBP4 levels and care compliance using Spearman analysis in healthy controls, CKD patients, and CKD patients receiving nursing interventions. The green circles represent the intervention group and the blue circles represent the control group.
Medication compliance rates in CKD patients in the control and intervention groups.
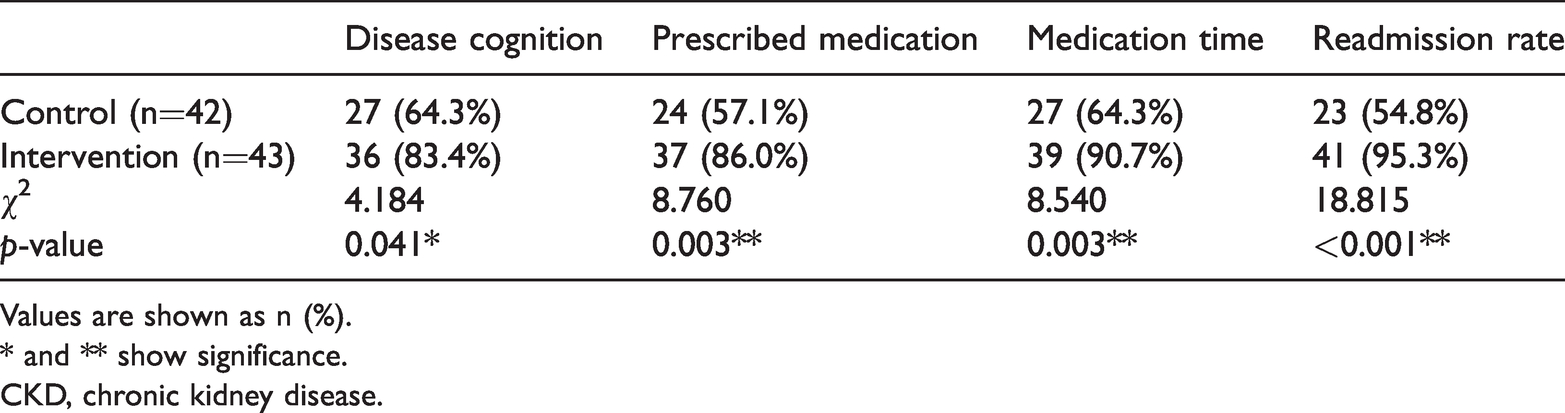
Values are shown as n (%).
* and ** show significance.
CKD, chronic kidney disease.
Association of serum PEBP4 levels and ion channel function in CKD patients received nursing care
Interestingly, in CKD patients receiving nursing interventions, declines in K+ and increases of Na+, Cl− and Ca2+ were observed compared with patients receiving the usual care (Figure 5a–d). This finding implied that care compliance had a similar therapeutic effect to calcium channel blockers. To investigate the underlying mechanisms, the association between serum PEBP4 levels and ion channel function was assessed. Following nursing interventions, PEBP4 levels were obviously decreased. Changes in serum PEBP4 levels were positively associated with K+ level, but negatively associated with Na+, Cl− and Ca2+ levels (Figure 5e–h). Thus, nursing interventions were associated with restoration of ionic concentration and declines in serum PEBP4 levels.

Correlations between serum PEBP4 levels and ion channel function in CKD patients receiving nursing interventions. Levels of K+ (a), Na+ (b), Cl− (c) and Ca2+ (d) in healthy controls, CKD patients, and CKD patients receiving nursing interventions. Correlations between PEBP4 levels and K+ (e), between PEBP4 levels and Na+ (f), between PEBP4 levels and Cl− (g) and between PEBP4 levels and Ca2+ (h) were analyzed using Spearman’s method. The blue circles represent healthy controls and the green circles represent CKD patients.
Discussion
Serum molecules are considered optimal biomarkers to assess the severity and prognosis of CKD. 25 Understanding the underlying roles and mechanisms of these biomarkers may help in the search for new diagnostic approaches for CKD. 26 In this study, we reported that PEBP4 was a novel diagnostic biomarker and that clinical nursing interventions for CKD patients potentially represented a new therapeutic strategy.
PEBP4 is aberrantly expressed in various malignancies. PEBP4 level is positively correlated with pathological stage in non-small cell lung cancer (NSCLC). Upregulation of PEBP4 promotes the proliferation and metastasis of NSCLC. 27 PEBP4 also promotes tumorigenesis in NSCLC by modulating the epithelial-mesenchymal transition and regulating the Shh signaling pathway. 28 Knockdown of PEBP4 inhibits cell growth and invasion of human glioma by regulating the ERK1/2 signaling pathway. 29 PEBP4 may also be a potential marker of semen quality and fertility. 30 PEBP4 regulates renal function and is a novel IgA nephropathy-related protein. 22 In the present study, serum PEBP4 levels were found to be elevated in advanced CKD patients compared with healthy subjects. Our data suggests that serum PEBP4 may participate in the progression of CKD.
Several biochemical indexes change along with progression of renal dysfunction. 31 Serum CysC is a more sensitive predictor of renal outcome and an independent biomarker related to the renal resistive index in CKD patients. 32 Serum sclerostin is a novel biomarker for heart valve calcification in CKD patients along with BUN and CRP. 33 In our study, we observed that PEBP4 levels were positively associated with BUN, CREA, CRP and CysC levels in patients with advanced CKD. Increasing proteinuria is associated with the pathological stage of CKD. 34 Moreover, CysC level showed a linear association with clinical pathological stage of CKD. 35 Our data illustrated that PEBP4 level was significantly positively correlated with clinical stage of CKD. Collectively, these data showed that PEBP4 could represent an effective diagnostic biomarker of advanced CKD. Serum CREA concentration is the main diagnosis marker of CKD. However, the cut-off value for urine CREA concentration is affected by urine specific gravity, making it prone to overestimation or underestimation. 36 As a marker of kidney function, CysC is more tightly correlated and has greater ROC AUC identity than CREA. 37 Our results indicated that the sensitivity of PEBP4 for diagnosis of advanced CKD was higher than that of common diagnostic biomarker of CKD including CREA, BUN and CRP. Thus, PEBP4 might have clinical value for diagnosis of advanced CKD.
Ion channels are critical for kidney function, and their dysregulation leads to several kidney diseases. Serum CREA, proteinuria and levels of ions such as Na+ and K+ are reduced in CKD patients. 38 Use of calcium channel blockers contributes to improvement of renal hemodynamics, enabling decreases in proteinuria. 39 We measured serum PEBP4 levels in patients treated with nifedipine, a calcium channel blocker. Interestingly, nifedipine notably reduced serum PEBP4 levels in CKD patients with concurrent changes in levels of Na+, K+, Ca2+ and Cl−. Some associations are known between serum PEBP4 levels and ion channel function in CKD patients. Ion channels regulate the homeostasis of endocytosis and exocytosis. As a secreted protein, PEBP4 can regulate cellular events and be transported into the extracellular matrix via endocytosis similarly to BUN, CREA, CysC and CRP. 40 Therefore, we speculate that the associations between PEBP4, BUN, CREA, CysC and CRP were linked through ion channels.
A previous study indicated that nursing interventions contributed to improved self-management of CKD patients. 41 Nursing care setting not only contributes to the identification and management of these patients, 42 but also promotes improved chronic care.43,44 Care interventions may result in decreased proteinuria. 45 However, the detailed mechanisms of care intervention-mediated decreases in proteinuria remain unclear. In the present study, we found that levels of PEBP4 were decreased in advanced CKD patients receiving nursing interventions and that PEBP4 level was negatively association with care compliance of CKD patients. Nursing interventions also altered ion channel function as well as levels of serum PEBP4. Significant associations were observed between these factors in CKD patients receiving nursing interventions, like those seen in patients receiving calcium channel blockers. These results showed the potential bridging effects of serum PEBP4 in nursing interventions for CKD patients. However, the connection between PEBP4 levels and ion channel function in CKD patients requires further study. In addition, the limited number of samples in our study may have affected the statistical significance of the results. A larger number of samples should be used to explore the clinical value of PEBP4 in CKD patients.
Conclusion
Serum PEBP4 levels were significantly elevated and were positively correlated with common diagnostic markers in advanced CKD patients. PEBP4 might be used as a diagnostic biomarker because of its high specificity for diagnosing advanced CKD patients. The negative association between PEBP4 and care compliance implied that it had potential as a nursing index for advanced CKD patients. Mechanistically, the restoration of ion channel function was probably the first event. The decline of serum PEBP4 was the second event following nursing interventions in CKD patients. Decreased serum PEBP4 was associated with decreased proteinuria in CKD patients. However, the role of serum PEPB4 in the decline of proteinuria in CKD patients need to be further explored.
Footnotes
Consent to participate
Written informed consent to participate in the study was obtained from all participants.
Consent for publication
We have obtained written informed consent from individuals to publish their data prior to submitting this paper to a journal.
Authors' contributions
HJ conceived the idea and drafted the manuscript; PP and HJ designed and performed the experiments; CL analyzed the data and designed the figures; PP and CL collected the clinical data. All authors discussed the results and edited the manuscript.
Availability of data and material
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Project of the Health and Family Planning Commission of Zhejiang Province (2019KY074) and the Project of the Zhejiang Provincial Public Welfare and Technology Application Research (LGF19H050005).