
Abstract
We present a case of a 43-year-old man with advanced hepatocellular carcinoma (HCC) with portal vein tumour thrombus. Initially, transcatheter arterial chemoembolization (TACE) was performed. Although alpha-fetoprotein (AFP) levels decreased, circulating tumour DNA (ctDNA) levels showed an upward trend, and abdominal magnetic resonance imaging (MRI) showed that tumours in the portal vein had increased. Based on ctDNA profiling, apatinib and anti-programmed cell death protein 1 (anti-PD-1) antibodies and were sequentially administered. Approximately three months later, intrahepatic tumours had significantly diminished and AFP and ctDNA levels had reduced. The response was sustained at the 23-month follow-up and the patient was in good health. Combination treatment of TACE, apatinib and anti-PD-1 antibodies was effective, and profiling of ctDNA fragmentation may be beneficial in the therapeutic management of patients with HCC.
Keywords
Introduction
Worldwide, liver cancer was the sixth most commonly diagnosed cancer and the fourth leading cause of cancer death in 2018, with an estimated 841,000 new cases and 782,000 deaths annually. 1 The most common form of liver cancer is hepatocellular carcinoma (HCC) which accounts for 75%-85% of cases. 1 Patients often present with unresectable, recurrent, or metastatic HCC, for which systemic chemotherapies are ineffective. 3 While European guidelines recommend systemic therapy (i.e., sorafenib) as the only anticancer treatment option for advanced HCC, Asian clinical practice guidelines recommend systemic therapy, radiotherapy and trans-arterial chemoembolization (TACE).4–6 Although TACE is regarded as a palliative treatment option for advanced HCC, some studies in patients with HCC and portal vein invasion have shown that TACE produced survival benefits.7,8
Increased expression of vascular endothelial growth factor (VEGF) has been shown to be associated with HCC progression. 9 Moreover, apatinib, a VEGF receptor (R)-2 tyrosine kinase inhibitor, has been shown to inhibit tumour growth, reduce angiogenesis and induce apoptosis in HCC cells. 10 Interestingly, one study in advanced HCC found that the long-term curative effects of TACE combined with apatinib were greater than TACE used alone. 11 In addition, immune checkpoint inhibitors, targeting the programmed cell death protein 1 (PD-1), have been studied in patients with advanced HCC.12,13 Among these novel treatment options, nivolumab has been approved by the US regulatory bodies as an adjunct treatment for patients who have failed treatment with sorafenib. 14
We report here a case of advanced HCC with portal vein tumour thrombus that was initially treated with TACE followed by apatinib and anti-PD-1 antibody therapy.
Case report
A 43-year-old man presented to our outpatient department with a four-week history of abdominal distention. The patient had tested positive for hepatitis B some 20 years previously and had been receiving entecavir for the past 12 months.
Contrast enhanced abdominal computed tomography (CT) scans showed a large heterogeneous irregular mass within the left hepatic lobe. Abdominal magnetic resonance imaging (MRI) showed multiple masses in the liver and partial portal vein tumour thrombus (Figure 1A). On admission, laboratory tests showed serum alpha-fetoprotein (AFP) levels were elevated at 9033 ug/l (normal levels, <10 ug/l) (Figure 2A). Plasma tumour circulating DNA (ctDNA) levels as assessed by an ultrasensitive chromosomal aneuploidy detector were 5.8% (Figure 2A).
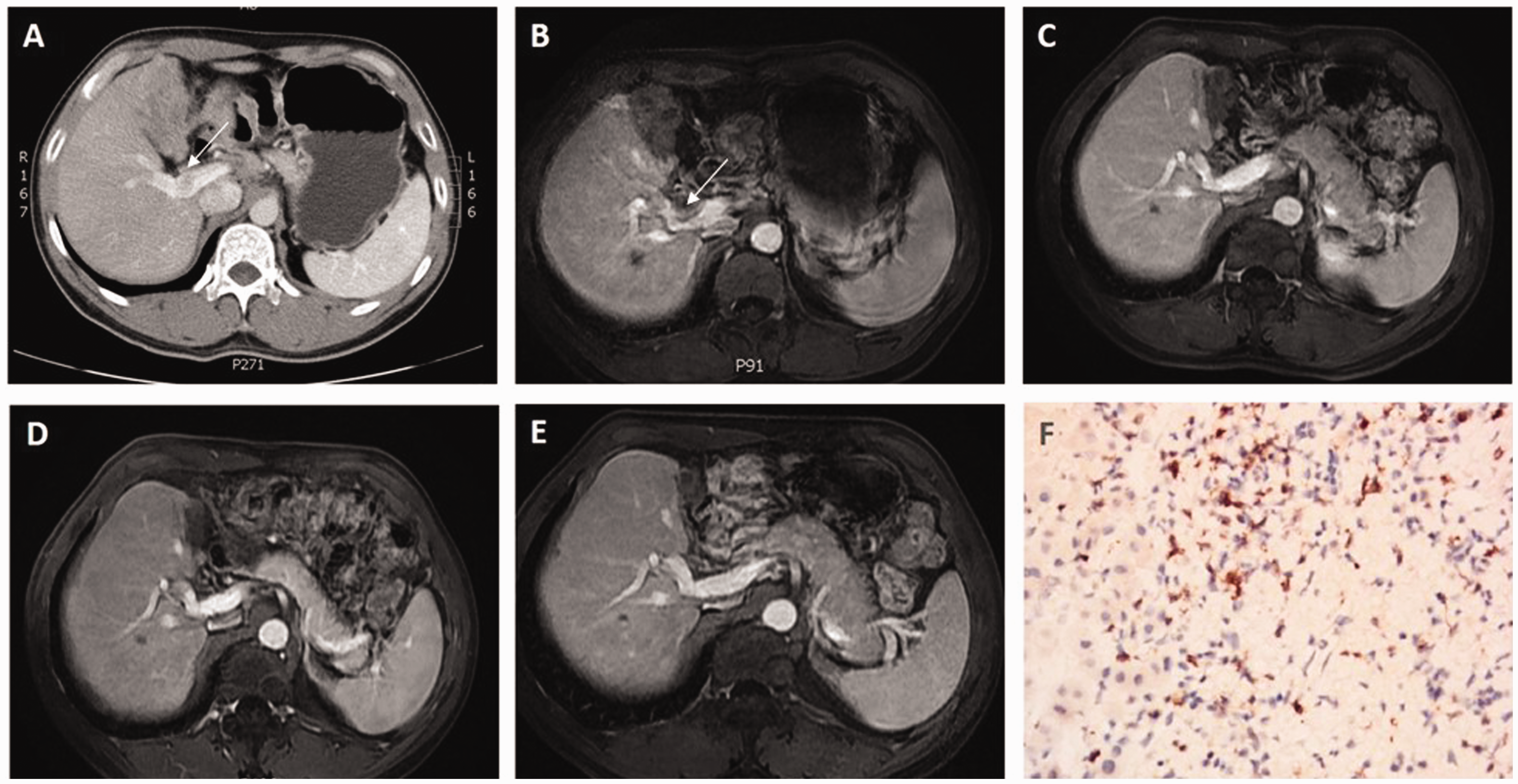
Abdominal magnetic resonance imaging (MRI) and immunohistochemistry with programmed cell death protein 1 (PD-1) antibody.

(A) Graph showing changes in serum alpha-fetoprotein (AFP) levels and plasma tumour circulating DNA (ctDNA) levels over time.
The profile of genetic alterations in ctDNA fragmentation was broad and included single nucleotide variations of TP53 and TERT; indels of TP53 and ARID1A; and amplifications of VEGFR, FGFR, and MYC. Histological examination using PD-1 antibodies showed that tumour cells accounted for 20% of the total number of cells and PD-1 was highly expressed (30%; Figure 1F).
According to his performance status (PS) test score (0) and Child-Pugh score (5), the patient was categorised as Barcelona Clinic Liver Cancer (BCLC) stage C. Having presented with advanced HCC, the patient had missed the opportunity to undergo surgery as a treatment option and underwent TACE four days after admission.
Approximately one month after TACE, the patient’s AFP levels had decreased, but ctDNA levels showed an upward trend and an abdominal MRI showed that portal vein tumour thrombus had increased (Figures 1B and 2A). Moreover, new lesions were found in the liver (Figure 3A). The patient underwent a second TACE treatment and 12 days later received apatinib 250 mg orally once daily, followed two days later by nivolumab 3 mg/kg intravenously every 2 weeks. Approximately one month after the combination treatment had started, his AFP levels had decreased to 1180 µg/l and ctDNA levels had decreased to 0.08% (Figure 2A).

Abdominal magnetic resonance imaging (MRI) following treatment.
Approximately three months after the start of combination treatment, an MRI showed that the intrahepatic tumours and portal vein tumour thrombus were significantly diminished (Figure 1C, Figure 3B). In addition, AFP levels had returned to normal levels and ctDNA levels had fallen to 0.06% (Figure 2A). While the profile of genetic alterations in plasma tumour ctDNA was significant at the beginning of treatment, no genetic alterations were detected after three months (Figure 2B). After approximately five months, and due to cost issues, nivolumab was changed to another anti-PD-1 antibody, SHR-1210 (camrelizumab). Camrelizumab has been shown to have a high efficacy and acceptable toxicity in pre-treated Chinese patients with advanced HCC. 13
Approximately 13 months after the start of combination therapy, the patient’s AFP levels were within normal range and his ctDNA levels were low (Figure 2A). Hepatic tumour sizes and portal vein tumour thrombus were reduced and unchanged from the previous clinic visit confirming a sustained response to the combination therapy (Figure 1D, Figure 3C).
At the last follow-up visit, approximately 21 months after the start of combination therapy, the patient was in good health and MRIs confirmed a sustained response (Figure 1E, Figure 3D). Laboratory tests showed, serum AFP levels 3.5 µg/l, total bilirubin 26 µmol/l, albumin 44 g/l, prothrombin time (PT) 14.2 sec. There was no evidence of hepatic encephalopathy or ascites and the patient’s Child-Pugh score was 5. Profiling of ctDNA fragmentation remained at a low level, without evidence of disease progression (Figure 2A, Figure 2B).
The main toxicities of treatment were a low-grade rash that was localized to both lower limbs and grade 2 hypertension. No other adverse events occurred during the 23-month treatment period.
Informed written consent was obtained from the patient prior to publication of this report and ethical approval was provided by Ethics Committee of Changzheng Hospital.
Discussion
HCC is one of the most widespread malignant tumours globally. 1 For patients with advanced disease there are few treatment options. 3 Our case report shows that the combination treatment of TACE, apatinib and anti-PD-1 antibodies had excellent anti-tumour effects in advanced HCC with portal vein tumour thrombus. In addition, we suggest that analysing ctDNA fragmentation may be a useful strategy in deciding treatment options for HCC. In this respect, our findings are similar to those of other studies which have shown that ctDNA can be used as a biomarker to track tumour progression.15,16
Although AFP measurement is one of the commonly used blood testing approaches for HCC screening, AFP levels have poor sensitivity and specificity. 15 ctDNA is released from necrotic or apoptotic tumour cells, which contain tumour-specific genomic alterations, including those in HCC.17,18 Indeed, in patients with HCC, the number of ctDNA mutations, maximal variant allele frequency of ctDNA and concentration of ctDNA have been shown to be linearly correlated with tumour size. 19 It has been suggested that the detection and characterization of ctDNA will enable. early detection of disease, monitoring of tumour heterogeneity, identification of therapeutic targets, real-time therapeutic response, early detection of tumour relapse, and dynamic assessment of drug resistance development. 20 In our case study, we recorded ctDNA levels over 23 months and these data helped us monitor the patient’s progression and ensured that he received appropriate treatment.
Initially, our patient received TACE and although his AFP levels decreased, his ctDNA levels showed an upward trend and his portal vein tumour thrombus had increased. Therefore, apatinib and anti-PD-1 antibody treatment were sequentially administered. We found that the combination therapy improved the patient’s outcome. These findings are consistent with those from a previous study that showed the beneficial additive effect of apatinib to TACE therapy 11 and another study that showed the addition of anti-PD-1 antibody treatment to apatinib resulted in improved potent antitumor activity. 21
While our data are from only one patient, the combination therapy of TACE, apatinib and anti-PD-1 antibodies shows promise in the treatment of advanced HCC with portal vein tumour thrombus. In addition, the profiling of ctDNA fragmentation may be beneficial in the therapeutic management of patients with HCC.
Footnotes
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by the Shanghai Committee of Science and Technology, China (Grant No. 17411972300).