
Abstract
Objective
To compare the characteristics, surgical complications, and overall survival between patients undergoing laparoscopy versus laparotomy for treatment of early-stage cervical stump carcinoma.
Methods
Patients with International Federation of Gynecology and Obstetrics (FIGO, 2009) stage IA2 to IIA2 cervical stump carcinoma who underwent laparoscopy or laparotomy in the Obstetrics and Gynecology Hospital of Fudan University from January 2000 to June 2018 were retrospectively reviewed. All patients’ clinical characteristics, pathological features, complications, and follow-up data were retrieved.
Results
Seventy-two patients were included in the analysis; 58 underwent laparoscopy and 14 underwent laparotomy. With respect to surgical complications, laparoscopy was associated with a significantly lower complication rate, less blood loss, a shorter operative time, and a higher hospitalization fee than laparotomy. Survival was not significantly different between the laparoscopy and laparotomy groups.
Conclusions
Although survival was not significantly different between the two surgical approaches, the rate of surgical complications was much lower in the laparoscopy than laparotomy group.
Introduction
Carcinoma of the cervical stump sometimes occurs in patients who have previously undergone supracervical hysterectomy, and it accounts for 2% to 5% of all cases of cervical cancer worldwide.1–3 The mainstream treatments for cervical stump carcinoma are radiotherapy and radical trachelectomy by either an abdominal or laparoscopic approach.4,5 Radiotherapy can frequently result in severe radiation injuries due to the lack of proper protection of important organs.6–8 Thus, surgical treatment is usually recommended. However, the modified anatomy caused by previous supracervical hysterectomy can cause great difficulty in performing radical trachelectomy and can increase the incidence of surgical complications. Therefore, in the present study, we retrospectively analyzed the clinicopathologic characteristics, complications, and follow-up data of patients with stage IA2 to IIA2 cervical stump carcinoma. Major surgical complications were also compared between abdominal and laparoscopic approaches.
Materials and methods
This study was approved by the Institutional Ethics Committee of Fudan University Obstetrics and Gynecology Hospital (2019-87). All patients provided written informed consent. The study population comprised patients who underwent surgical treatment of 2009 International Federation of Gynecology and Obstetrics (FIGO) stage IA2 to IIA2 cervical stump cancer from January 2000 to June 2018. All medical records were reviewed to obtain the patients’ clinical characteristics, pathological data, complications, and follow-up results. The patients underwent a preoperative workup and regular follow-up in accordance with the National Comprehensive Cancer Network (NCCN) guidelines at the time. 9 All patients were followed up every 3 months for the first 2 years postoperatively, then every 6 months thereafter. The median follow-up time was 50.5 months (range, 9–171 months).
Continuous variables are described as mean and interquartile range, and categorical variables are described as number and proportion. Selected characteristics were compared between the laparoscopy and laparotomy groups using the χ2 test for categorical variables and the t test for continuous variables. The Kaplan–Meier method with the log-rank test was used to compare survival outcomes. The statistical software package used for analyses was IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp., Armonk, NY, USA). All tests were two-sided, and a P value of <0.05 was considered statistically significant.
Results
Patients’ characteristics
Seventy-two patients with stage IA2 to IIA2 cervical stump carcinoma were included in this study; 58 underwent laparoscopy and 14 underwent laparotomy. As shown in Table 1, all 72 patients had previously undergone supracervical hysterectomy for the following reasons: uterine fibroids in 60 (83.3%) patients, adenomyosis in 7 (9.7%), abnormal uterine bleeding in 1 (1.4%), and hemorrhage during cesarean section in 4 (5.6%). Of the 72 patients, 70 supracervical hysterectomies were performed by laparotomy and 2 were performed by a laparoscopic approach. With respect to postoperative follow-up, only 19 (26.4%) patients underwent regular cervical screening; the remaining 53 (73.6%) patients lacked efficient follow-up screening. Most patients (84.7%) sought medical help because of clinical symptoms such as abnormal vaginal bleeding (n = 51, 70.8%) and discharge (n = 10, 13.9%). The mean interval between supracervical hysterectomy and the diagnosis of cervical stump carcinoma was 10.5 years (range, 1–35 years).
Clinical characteristics of patients with cervical stump cancer.

Data are presented as n (%) or mean (interquartile range).
SHT, supracervical hysterectomy; FIGO, International Federation of Gynecology and Obstetrics; LVSI, lymphovascular space invasion.
Table 1 shows the clinicopathologic characteristics of the 72 patients who were diagnosed with stage IA2 to IIA2 cervical stump carcinoma and underwent radical trachelectomy and pelvic lymphadenectomy. The patients’ mean age was 50.5 years. Most patients (n = 49, 68.1%) had stage IB1 cancer, and the most common histologic type was squamous cell carcinoma (n = 64, 88.9%). With respect to adjuvant treatment, 38 (52.8%) patients received concurrent chemoradiotherapy after surgery and 4 (2 with IB2 cancer and 2 with IIA2 cancer) received neoadjuvant chemotherapy before surgery. In terms of the surgical approach, 58 (80.6%) patients were treated by laparoscopic radical trachelectomy and 14 (19.4%) underwent laparotomy.
Comparison of characteristics and outcomes between laparoscopy and laparotomy groups
Comparison of the perioperative data between the laparoscopy and laparotomy groups revealed that laparoscopy was associated with significantly less blood loss (300.9 vs. 925 mL, respectively; P < 0.01), a shorter operative time (216.6 vs. 262.1 minutes, respectively; P = 0.01), and a higher hospitalization fee (4690.6 vs. 2874.7 USD, respectively; P < 0.001). However, there was no significant difference in the mean age (51.4 vs. 49.3 years) or duration of hospitalization (15.5 vs 17.1 days) between the two groups.
Next, comparison of surgical complications showed that the complication rate was significantly lower in the laparoscopy than laparotomy group (19.0% vs. 64.3%, respectively; P = 0.002). Fourteen complications occurred among 11 patients who underwent laparoscopy, including 10 intraoperative complications (1, 3, and 6 cases of bladder injury, ureter injury, and transfusion, respectively) and 4 postoperative complications (1 case each of ureterovaginal fistula, ureteral fistula, ureteral obstruction, and secondary infection of pelvic hematoma). These 11 women constituted 19% of the patients in the laparoscopy group. In the laparotomy group, however, 11 complications occurred among 9 patients, including 7 intraoperative complications (1 and 6 cases of bladder injury and transfusion, respectively) and 4 postoperative complications (2 cases each of adynamic ileus and delayed incision healing).
In the comparison of survival, the median survival time was not shown in either the laparoscopy or laparotomy group because the minimum survival rate in each group was 0.862 and 0.917, respectively (P > 0.05) (Figure 1).
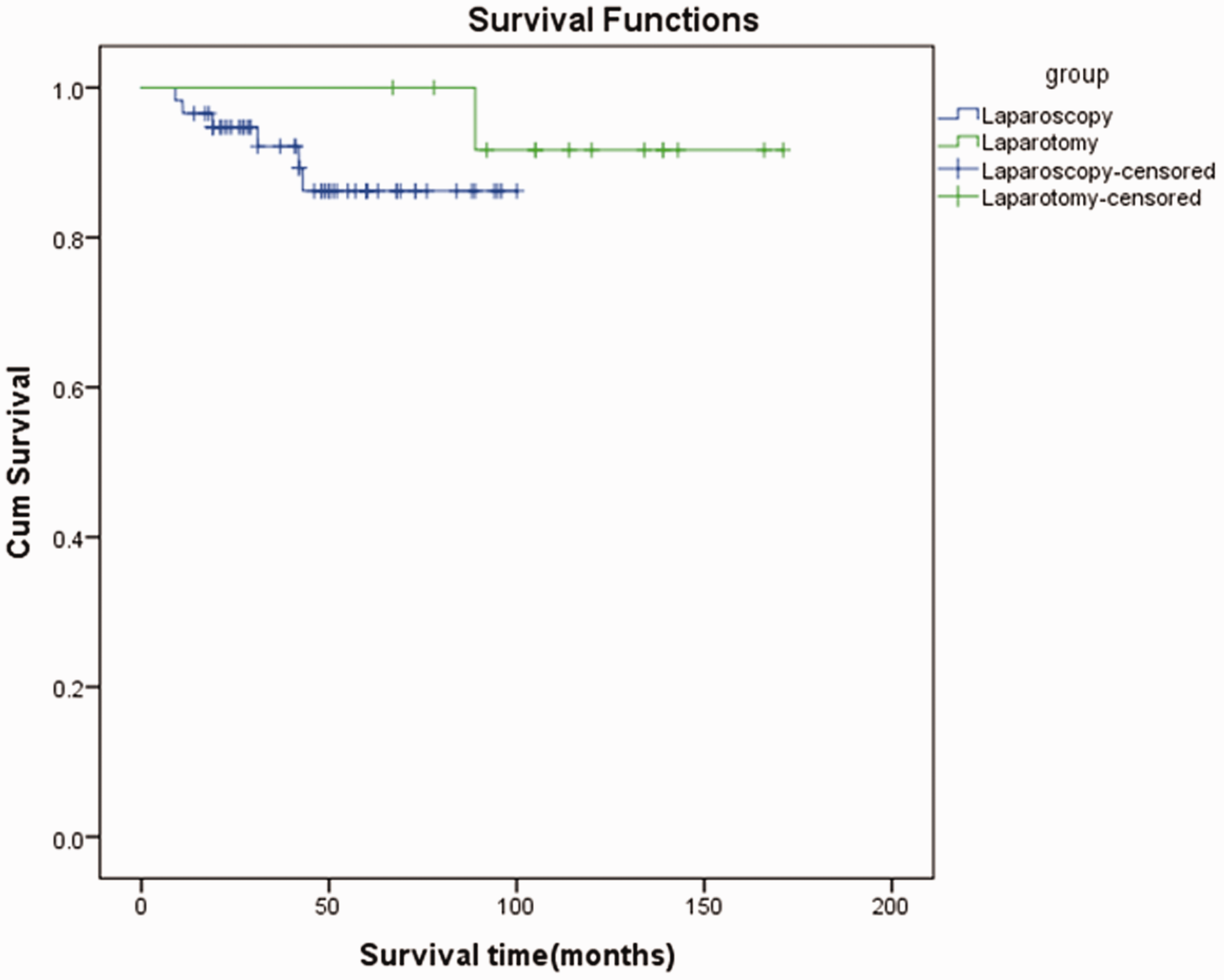
Kaplan–Meier survival curve in laparoscopy and laparotomy groups (log-rank 0.292)
Discussion
Although supracervical hysterectomy is being gradually abandoned, it is still performed in some remote areas with poor medical care in China. Most patients in less developed areas lack regular follow-up screening for cervical cancer and seek medical help only after the appearance of clinical symptoms such as abnormal vaginal bleeding and vaginal discharge. Thus, in the present study, the cervical stump carcinoma was diagnosed at an advanced stage in most cases. The major treatments for cervical stump carcinoma are radiotherapy and radical trachelectomy. Because radiotherapy is associated with severe radiation injuries, surgical treatment is usually recommended.
In this study, the rate of major surgical complications was much lower in the laparoscopy than laparotomy group. Two possible reasons for this difference are as follows. First, the anatomic change caused by subtotal hysterectomy increases the difficulty of radical trachelectomy. However, laparoscopy can help to more clearly identify the ureter, and fewer injuries occur during the operation. Second, compared with laparotomy, laparoscopy has a shorter recovery time, a shorter hospital stay, and fewer postoperative complications because it is a minimally invasive surgical operation. In this regard, laparoscopic surgery is a viable and safe procedure.
Before publication of the Laparoscopic Approach to Cervical Cancer (LACC) trial, 10 minimally invasive surgery was consistently shown to produce survival outcomes similar to those of laparotomy but with a shorter hospital stay and more rapid patient recovery. At the same time, a great many international guidelines recommended minimally invasive surgery as a routine approach. However, the results of the LACC trial upended the previous consensus. Both the LACC study and another high-quality retrospective study showed that minimally invasive surgery is inferior to open surgery in terms of tumor-free survival and overall survival in patients with early cervical cancer.10,11 In the present study, the median survival time was not shown in the two groups, which may have been because the minimum survival rates had a P value of >0.05. In addition, this was a small-sample study from a single institution, which may have also affected the statistical outcome. Therefore, a longer follow-up time is needed to determine whether traditional open surgery or minimally invasive surgery is better for cervical stump carcinoma.
This study had two main limitations. First, although we strictly adhered to the inclusion and exclusion criteria, bias might still exist because of the retrospective study design and large time span. Second, the relatively small number of patients limited our power to detect differences between the laparoscopy and laparotomy groups. Thus, stricter quality control measures, a larger sample size, and a longer follow-up time are needed. These limitations might be overcome in future prospective studies.
In conclusion, our study identified an association between laparoscopy and a lower rate of surgical complications compared with laparotomy in patients with stage IA2 to IIA2 cervical stump carcinoma. However, a longer follow-up period is needed to compare the survival outcome between laparoscopic surgery and traditional laparotomy.