
Abstract
Esophageal diverticulum with secondary bronchoesophageal fistula is a rare clinical entity that manifests as respiratory infections, coughing during eating or drinking, hemoptysis, and sometimes fatal complications. In the present study, we describe a case of bronchoesophageal fistula emanating from esophageal diverticulum in a 45-year-old man who presented with bronchiectasis. We summarize the characteristics of this rare condition based on a review of the relevant literature.
Keywords
Introduction
Fistulas between the esophagus and tracheobronchial tree are a common occurrence in adults with malignancies. However, benign tracheoesophageal or bronchoesophageal fistulas (BEF) resulting from tuberculosis, 1 trauma, surgical operation, 2 chemoradiotherapy, foreign body, and broncholithiasis or tracheal intubation balloon compression 3 are rare in adults. In fact, BEF secondary to esophageal diverticulum is extremely rare. Although it is a benign lesion, BEF causes recurrent pneumonia, pleural empyema, hemoptysis, and sometimes fatal complications.
In the present study, we report a case of BEF secondary to esophageal diverticulum, presenting as bronchiectasis with recurrent pneumonia and hemoptysis for 3 years in a 45-year-old man. We summarize and review the clinical characteristics, etiology, and treatment of this rare condition.
Case presentation
A 45-year-old man with a 3-year history of chronic cough and recurrent hemoptysis and fever was admitted to our hospital. The cough, which became productive, was exacerbated by swallowing of fluids. Fever and hemoptysis had recurred four times, necessitating antibiotic therapy. A chest computed tomography (CT) scan revealed left lower pulmonary bronchiectasis. Consequently, the patient was referred to us for further diagnosis, although his symptoms were relatively stable. Medical history revealed prior occurrence of hyperthyroidism and hypertension but no history of tuberculosis. Upon physical examination, we noted a few coarse rales in the left lower posterior lung but no finger clubbing. The rest of his physical examination was normal.
Medical examinations revealed normal blood, liver, kidney, and thyroid functions, as well as normal results for tumor markers. Results from sputum cultures and PCR to test for tuberculosis were negative. However, a chest CT revealed bronchial dilatation in the dorsal segment of the left lower lobe (LLL), with a chronic pulmonary abscess surrounding it. The CT indicated the presence of a fistula between the mid-esophagus and the left intermediate bronchus without mediastinitis or lymphadenopathy (Figure 1). Bronchoscopy revealed mucosal hyperemia and swelling in the dorsal segment bronchus of the LLL, without purulent secretions and no obvious endobronchial lesions or BEF outlet opening. Histopathological analysis of the bronchial mucosa revealed a normal columnar epithelium, with no inflammation, granuloma, or carcinoma. In addition, iodine contrast examination revealed a medium-sized diverticulum at the left lateral aspect of the esophagus, which had developed a fistulous connection with the LLL bronchus (Figure 2). Esophagoscopy revealed the diverticulum to be 33 cm from the incisors, with a 3-mm fistulous orifice arising from its apex (Figure 3). Therefore, the etiology of the bronchiectasis and chronic lung abscess was determined to be BEF secondary to esophageal diverticulum. After multidisciplinary consultation, video-assisted thoracic surgery was suggested as the first choice of treatment and endoscopic therapy as the second choice. The patient refused further treatment because of the potential risks and was subsequently discharged. At the 4-month follow-up, the patient again developed pulmonary infection but improved after treatment with antibiotics.

Computed tomography scan revealed bronchial dilatation in the dorsal segment of the left lower lobe with chronic pulmonary abscess surrounding it. A suspected fistulous communication between the middle esophagus and the left intermediate bronchus was indicated. There was no mediastinitis or lymphadenopathy.

A Lipiodol (iodine) swallow revealed a medium-sized diverticulum at the left lateral aspect of the esophagus, which had developed a fistulous connection with the left lower lobe bronchus.
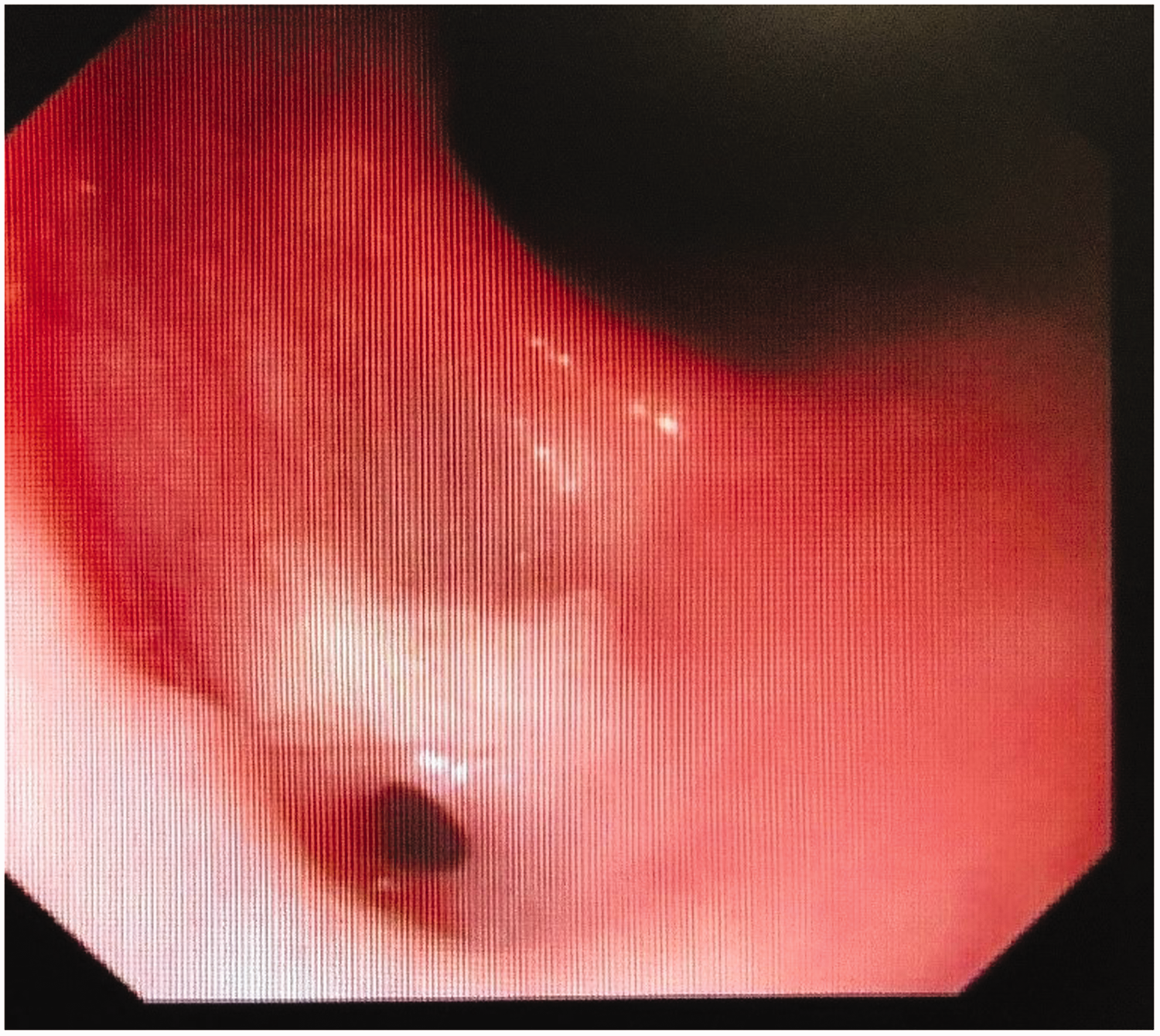
Esophagoscopy showed the diverticulum 33 cm from the upper incisors, with a 3-mm fistulous orifice arising from its apex.
Discussion
We performed a literature review to summarize the characteristics of this rare condition. To identify relevant literature, we searched the PubMed, Embase, and Cochrane library databases, and retrieved articles published in English until March 2020. We used the following terms for article identification: “esophageal diverticulum” or “esophageal diverticulitis” or “esophageal diverticula” and “esophagobronchial fistula” or “bronchoesophageal fistula.” Articles describing congenital BEF in children or acquired BEF including tumor, tuberculosis, broncholithiasis, trauma, surgical treatment, chemoradiotherapy, granulomatous disease, foreign body, or tracheal intubation balloon compression were excluded. We reviewed abstracts and accessed full texts of the selected articles. Finally, 13 articles describing BEF secondary to esophageal diverticulum were included; all of these were case reports. A summary of features across those cases is outlined in Table 1.4–16 Briefly, participants’ ages ranged from 52 to 80 years (median: 63 years), and the ratio of female to male patients was 3:1. The median duration from onset to diagnosis was 36 months (from 1 week to 20 years). Ten patients presented with postprandial cough; that is, a cough triggered by eating or drinking. Most of the esophageal diverticula (11/13) originated from the mid-esophagus, and the remaining cases were from the distal (1/13) or epiphrenic (1/13) esophagus. Chest CT showed inflammatory changes, bronchiectasis, abscess, or a normal status; only four cases demonstrated the fistula on chest CT. Esophagogram and esophagoscopy were the main methods of diagnosis. For treatment, surgery was reported in seven patients, whereas endoscopic treatment, using clips, histoacryl, or cardiac septal occluder devices, was performed in four patients. Generally, these approaches resulted in good outcomes. One patient reportedly died of severe hemoptysis before a definite diagnosis was made. Finally, etiology of the diverticulum was identified as nonspecific chronic inflammation, congenital, and unknown in four, two, and seven cases, respectively.
Clinical characteristics of patients with bronchoesophageal fistula secondary to esophageal diverticulum.

CT, computed tomography.
Previous studies have shown that most esophageal diverticula occur accidentally, during an endoscopic or radiologic examination. 17 In fact, their classification is based on anatomical location, including upper (Zenker or pharyngoesophageal), middle (traction), or lower (distal or epiphrenic) locations. 18 According to our analysis, diverticula emanating from BEF primarily originate from the mid-esophagus. The literature review showed that this condition originated from distal or epiphrenal diverticulum in 2 of 13 cases,9,12 one of which was a pulsion diverticulum due to achalasia. 12 However, there are differing opinions regarding the etiology of esophageal diverticula emanating from BEF. For example, in our literature review, diverticula in the middle of the esophagus with fistula were caused by chronic nonspecific inflammation (3/11), congenital (2/11), or had an unclear or idiopathic cause (6/11). Generally, acquired diverticulum is an external inflammatory reaction in the neighboring mediastinal space that adheres to the esophagus and retracts the wall in a manner that results in contraction and scars the tissue. Consequently, this provokes a traction or true diverticulum, implying that it has as many layers as the esophageal wall itself. 19 In the present case, chest imaging revealed enlarged or calcified periesophageal and mediastinal lymph nodes, whereas histopathology of a resectioned diverticulum indicated inflammatory infiltration. In addition, we excluded tuberculosis infection during our analysis; it is the main cause of BEF induced by suppurative infection. However, old tuberculosis may be the origin of traction diverticulum.
In recent years, many reports20,21 have emphasized the link between an underlying esophageal dynamic disorder and the presence of an esophageal diverticulum. In the 13 articles that we reviewed, Herbella and Del Grande 12 reported an epiphrenic diverticulum with achalasia tested by manometric studies, and Braghetto et al. 11 reported a case of middle esophageal diverticulum with nonspecific motor disorder. No other articles mentioned the patient’s esophageal manometry. It may be that the relationship between esophageal dynamic disorders and diverticulum was not previously recognized and manometric evaluation was not emphasized. Esophageal dynamic disorders are associated with the formation of diverticula. Achalasia has traditionally been considered the primary esophageal motility disorder associated with esophageal diverticula, and propagating peristalsis, often with hypercontractility, was the predominant motility pattern observed with high-resolution manometry 22 in patients with esophageal diverticula in recent studies. Surgery of the lower esophageal sphincter together with diverticulectomy 23 was recently reported in diverticulum with motor disorders to treat symptoms and prevent recurrence of the diverticulum. However, esophageal diverticulum with fistula is extremely rare, and manometric evaluation would be needed to explore the association between esophageal dynamics disorders and BEF secondary to esophageal diverticulum.
Congenital BEF is usually associated with esophageal atresia and is typically diagnosed during the neonatal period. Previous studies have shown that if it is not associated with esophageal atresia, it generally persists until adulthood before diagnosis. 24 Braimbridge and Keith 25 classified congenital BEF into four types. Type 1 is mainly associated with a diverticulum of the esophagus, which might become inflamed due to stasis within the dependent tip of the diverticulum. Diverticular inflammation leads to its erosion and perforation into the bronchus. Although this type of fistula is congenital, its clinical presentation and manifestation are secondary to the underlying inflammatory changes. Therefore, it might be difficult to differentiate between a congenital and an acquired form, especially following the existence of advanced pulmonary disease. We reviewed two cases of Braimbridge type 1 congenital BEF. Generally, the criteria for diagnosing a fistula include the following:6,10 (1) no past surrounding inflammation; (2) no adhesion of lymph node observed in the fistula; (3) presence of mucosa and definite muscularis mucosa; and (4) transition of the epithelial lining of the fistula from squamous (esophageal) to columnar (respiratory). In our case, we found no evidence of mediastinal inflammation, based on CT or histopathological analysis of inflammatory infiltration of bronchial mucosa. Consequently, Braimbridge type 1 congenital BEF might be the most likely etiology, although histopathological confirmation of fistula is essential.
Diagnosing BEF secondary to esophageal diverticulum is challenging, because of its insidious clinical course. In our literature review, the median duration from onset to diagnosis was 36 months, with the longest period being 20 years. In addition, the most specific and prominent symptom was cough triggered by eating or drinking, although in older people, cough triggered by swallowing is often confused with a swallowing disorder. According to the reviewed studies, CT confirmed inflammatory infiltration, bronchiectasis, abscess, and mediastinal lymphadenopathy, but only identified four cases of esophageal diverticulum or fistula. In fact, the most sensitive and definitive diagnostic tool is upper gastrointestinal radiography. 11 Although esophagography can effectively confirm diverticulum and the orifice, bronchoscopy does not detect small or distal lesions.
Several articles in our literature review speculated on the reasons for the lengthy asymptomatic interval:26,27 (1) mid-esophageal diverticula, which had unusual small lesions with a wide base that were frequently asymptomatic; (2) presence of a membrane overlying the fistula, which subsequently ruptured; (3) presence of a proximal fold of the esophageal mucosa overlapping the orifice, which subsequently became less mobile; (4) antigravitational or upward extension of the fistulous tract from the esophagus, which could close during swallowing; and (5) presence of spasm at the smooth muscle in the fistula wall. Although the initial symptoms were silent, they were capable of inducing fatal complications. In our case, the patient had suffered from recurrent respiratory infections and hemoptysis. In contrast, Svane et al. 7 reported that an 80-year-old woman died of massive hemoptysis and fistula, which were diagnosed at autopsy. Overall, these findings indicate that timely detection and diagnosis are essential for managing BEF through esophageal diverticulum.
The recommended therapy for treating esophagorespiratory fistula is surgery, which involves division of the fistula and excision of any permanently damaged lung segment. 11 However, some patients avoid surgery because of the poor conditions caused by severe, recurrent, aspirated pneumonia and malnutrition. The other treatment option is endoscopic therapy, 28 which involves the use of an endo-stapler, histoacryl, clips, suturing, 29 or cardiac septal occluder device.30,31 Although favorable short-term benefits for this approach have been reported, the long-term prognosis remains unclear.
In conclusion, we described a case of BEF emanating from an esophageal diverticulum and reviewed the relevant literature. Although BEF secondary to esophageal diverticulum is very rare, it has been reported in several previous cases. To our knowledge, this is the first article to systematically summarize the clinical manifestations, possible etiology, treatment, and prognosis of this rare disorder. This report may provide a fuller picture of the disease so that it can be accurately diagnosed and promptly treated.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060521992234 - Supplemental material for Bronchoesophageal fistula secondary to esophageal diverticulum in an adult: a case report and literature review
Supplemental material, sj-pdf-1-imr-10.1177_0300060521992234 for Bronchoesophageal fistula secondary to esophageal diverticulum in an adult: a case report and literature review by Xiaolin Zhang, Hongmei Jiao and Xinmin Liu in Journal of International Medical Research
Supplemental Material
sj-jpg-2-imr-10.1177_0300060521992234 - Supplemental material for Bronchoesophageal fistula secondary to esophageal diverticulum in an adult: a case report and literature review
Supplemental material, sj-jpg-2-imr-10.1177_0300060521992234 for Bronchoesophageal fistula secondary to esophageal diverticulum in an adult: a case report and literature review by Xiaolin Zhang, Hongmei Jiao and Xinmin Liu in Journal of International Medical Research
Supplemental Material
sj-jpg-3-imr-10.1177_0300060521992234 - Supplemental material for Bronchoesophageal fistula secondary to esophageal diverticulum in an adult: a case report and literature review
Supplemental material, sj-jpg-3-imr-10.1177_0300060521992234 for Bronchoesophageal fistula secondary to esophageal diverticulum in an adult: a case report and literature review by Xiaolin Zhang, Hongmei Jiao and Xinmin Liu in Journal of International Medical Research
Supplemental Material
sj-jpg-4-imr-10.1177_0300060521992234 - Supplemental material for Bronchoesophageal fistula secondary to esophageal diverticulum in an adult: a case report and literature review
Supplemental material, sj-jpg-4-imr-10.1177_0300060521992234 for Bronchoesophageal fistula secondary to esophageal diverticulum in an adult: a case report and literature review by Xiaolin Zhang, Hongmei Jiao and Xinmin Liu in Journal of International Medical Research
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics and consent
The study was approved by the Ethics Board of Peking University First Hospital. We obtained informed consent from the patient authorizing publication of this article and have removed any identifying information.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this work was received from the Interdisciplinary Clinical Research Project of Peking University First Hospital (2019CR40) and China Central Health Research Fund (W2013BJ29).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.