
Abstract
Tuberculous bronchoesophageal fistula is a rare complication of tuberculosis. Herein, we report the case of a woman in her late 60s with a choking cough for more than 1 month. Iohexol esophagography revealed a fistulous communication between the esophagus and the right principal bronchus, and gastroscopy documented a fistulous orifice in the esophagus. Endoscopic closure with metal clips failed, and other treatment options, such as extended conservative treatment, covered self-expandable metal stents, and over-the-scope clips were rejected by the patient. Therefore, a combined therapy, endoscopic submucosal dissection-based suture combined with medical adhesive, was performed. Follow-up iohexol esophagography and gastroscopy confirmed fistula closure. During 1 year of follow-up after discharge, the bronchoesophageal fistula did not recur. Endoscopic submucosal dissection-based suture combined with medical adhesive appears to be a practical and feasible solution to complicated tuberculous bronchoesophageal fistula.
Keywords
Introduction
Bronchoesophageal fistula is caused by malignant tumors, infections, trauma, and rare conditions, such as esophageal diverticulum and tuberculosis.1–2 Tuberculous bronchoesophageal fistula is an infrequent tuberculosis complication that significantly decreases patients’ quality of life and prolongs hospitalizations. Optimal therapeutic options for tuberculous bronchoesophageal fistula may differ considerably and involve treatments such as antituberculosis medication, endoscopic intervention, and surgery.3–4 In addition to controlling infections and improving nutritional status, limiting fistula output is considered critical in the management of gastrointestinal fistulas. 5 Endoscopic interventions to limit fistula output comprise clips, metal stents, medical adhesives, the OverStitch system (Apollo Endosurgery, Austin, TX, USA), and over-the-scope clips (OTSC).6–7 When the effects of these treatments are unsatisfactory or these options are not accepted by the patient, subsequent treatment may be challenging. Herein, we report a complicated case of tuberculous bronchoesophageal fistula successfully managed by combined therapy with endoscopic submucosal dissection (ESD)-based suture and medical adhesive.
Case report
The reporting of this study conforms to the CARE guidelines. 8 All patient details have been de-identified, and the patient provided written informed consent for treatment. In our institution, case reports do not require ethics review board approval. A woman in her late 60s was admitted to our hospital with a complaint of a choking cough for more than 1 month. She was diagnosed with pulmonary and endobronchial tuberculosis at her local hospital 9 months earlier, and neoplastic lesions were excluded. She had taken antituberculosis drugs regularly since then. The general physical examination findings were unremarkable. Iohexol esophagography revealed a fistulous communication between the right principal bronchus and the esophagus (Figure 1a), and gastroscopy documented a fistulous orifice in the esophagus (Figure 1b). Bronchoscopic techniques failed to treat the fistula. Although she endured another 3 months of gastric tube feeding and continued to take rifampicin, isoniazid, pyrazinamide, and ethambutol, regularly, her choking cough had not been relieved as expected. Therefore, she refused to continue conservative treatment and requested endoscopic interventions. However, she firmly refused fully-covered self-expandable metal stents (SEMS) owing to concerns regarding stent migration. Moreover, she declined the OTSC option because of economic concerns. Endoscopic closure of the bronchoesophageal fistula was then performed with an electrosurgical knife (Olympus Medical Systems, Co., Ltd., Tokyo, Japan) (Figure 2a) and multiple clips (Micro-Tech (Nanjing) Co., Ltd., Nanjing, China) (Figure 2b); however, this treatment was ineffective. Therefore, a combined therapy, ESD-based suture combined with medical adhesive, was recommended after multidisciplinary consultation. The subsequent endoscopic procedures were as follows: in the first step, ESD around the esophageal fistulous orifice was performed with electrosurgical knives (Olympus) (Figure 3a). The mucosal defect was closed in the subsequent step with a nylon loop (Olympus) and metal clips (MicroTech) (Figure 3b). Next, the medical adhesive (spray type, Beijing Compont Medical Devices Co., Ltd., Beijing, China) was sprayed onto the surface of the postoperative area (Figure 3c). No airway adverse events occurred after the endoscopic procedures. Antituberculosis drugs comprised oral isoniazid (0.3 g, once per day), rifampicin (0.45 g, once per day), pyrazinamide (1.5 g, once per day), and ethambutol (0.75 g, once per day). After 6 additional weeks of treatment, repeat iohexol esophagography revealed no contrast agent extravasation, and gastroscopy detected closure of the bronchoesophageal fistula and postoperative hyperplastic mucosal changes in the esophagus (Figure 3d). Compared with patients treated with OTSCs in our institution, we estimated the total cost of ESD-based suture and medical adhesive as one-third the cost of OTSCs. During 1 year of follow-up, the patient’s bronchoesophageal fistula and choking cough did not recur, and she was satisfied with the effect of the combined therapy.

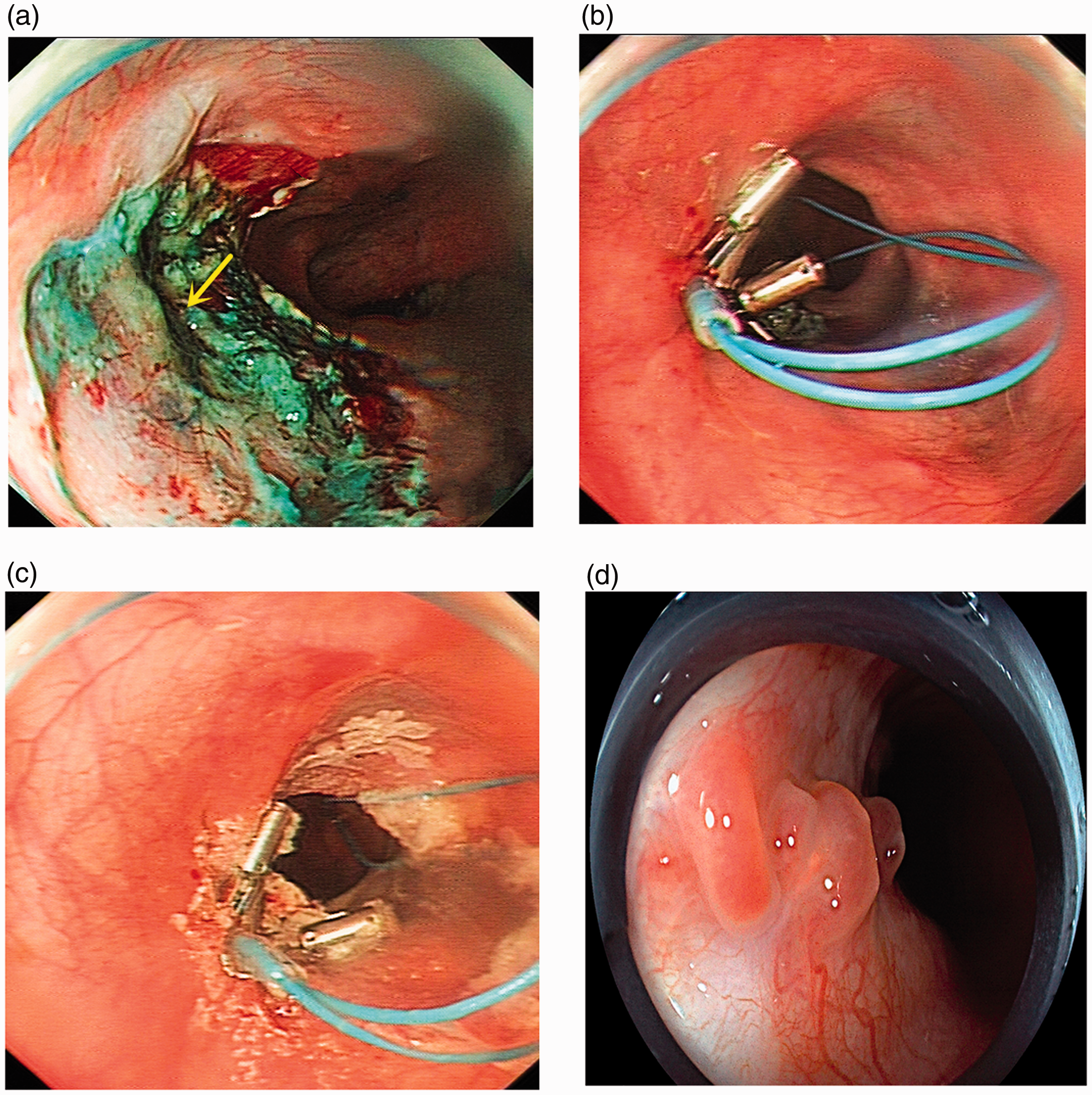
(a) Fistulous communication (yellow arrow) between the right principal bronchus and the esophagus detected by iohexol esophagography. (b) Fistulous orifice in the esophagus detected by gastroscopy.

(a) The mucosa around the fistula orifice was preprocessed with an electrosurgical knife. (b) The fistula was sealed with multiple clips.
(a) Endoscopic submucosal dissection with electrosurgical knives around the fistula orifice (yellow arrow). (b) Mucosal closure with a nylon loop and metal clips. (c) Medical adhesive (spray type) sprayed on the postoperative mucosal surface. (d) The fistula closure and postoperative hyperplastic mucosal changes detected by follow-up gastroscopy.
Discussion
The development of tuberculous bronchoesophageal fistula is associated with periesophagitis, peritracheitis, and local abscess due to rupture of caseonecrotic lymph nodes. 9 The possibility of fistula formation should be considered when tuberculosis patients develop a choking cough related to eating or drinking. Further gastroscopy, bronchoscopy, and iohexol esophagography will help make the diagnosis. In this case, the patient developed a choking cough during her continuation treatment phase, and a bronchoesophageal fistula was diagnosed by gastroscopy and iohexol esophagography. This case enriched our understanding of tuberculous bronchoesophageal fistula, showing that even patients taking antituberculosis medications may develop fistulas.
Endoscopic closure of tuberculous bronchoesophageal fistula remains a challenge. Standard suture methods with metal clips may lead to incomplete closure and failed treatment, as in this case and in similar cases in our institution. Moreover, concerns regarding medical adhesives comprise the risk of airway inflammation and glue leakage through the fistula. 10 Although OTSC closure is easy to perform and has a high technical success rate in patients with gastrointestinal fistula, its relatively low clinical success rate and high cost are still unsatisfactory. 5 Additionally, OTSC is still unavailable or unaffordable for many patients in China and other developing countries. Therefore, many patients with bronchoesophageal fistula had undergone previous failed endoscopic repair attempts. 5 Although several articles reported that tuberculous bronchoesophageal fistula could be cured by antituberculosis drugs alone, some patients in these articles had no medical history of tuberculosis or had not taken antituberculosis drugs regularly before the fistula formation. 11 Although the OverStitch endoscopic suturing system was a reported valid alternative to conventional therapy, 7 it is still unavailable or unaffordable for many patients in China. In the current case, the patient was taking antituberculosis medications regularly when her fistula occurred. After the fistula formed, she was treated successively with antituberculosis medication and endoscopic sutures with metal clips, but neither of these treatments was effective. Meanwhile, she rejected metal stents and OTSCs for economic reasons and because of concerns regarding stent migration. The patient's worries were not unreasonable. Despite previous reports of efficacy in patients with bronchoesophageal fistula, the primary concern with esophageal fully-covered SEMS is stent migration. Recently, although it has been reported that endoscopic suture fixation of esophageal SEMS could reduce stent migration, stent migration still occurred in nearly one-sixth of patients, and the overall endoscopic cost increased. 12
Combined endoscopic procedures may provide better results in challenging cases. 13 Mammana et al. reported that among 25 endoscopically-treated patients with bronchoesophageal fistula, 4 patients received combined endoscopic treatments, and the most common endoscopic tools were clips, stents, glue, and septal occluders. 14 Therefore, the combination of ESD-based suture and medical adhesive was proposed and implemented, in this case. Esophageal ESD around the fistulous orifice was intended to provide a larger mucosal defect for the subsequent endoscopic nylon loop suture.
Ours is the first report of using the ESD technique to treat tuberculous bronchoesophageal fistula. The innovative application of the ESD technique in patients with bronchoesophageal fistula also provides a promising and economical option in cases where stents, OTSCs, and the OverStitch suturing system are unavailable or unaffordable. Clips and nylon loops provided a tighter suture effect than clips alone, and subsequently, covering the postoperative area with a medical adhesive enhanced the sealing of the fistula without causing glue leakage. ESD-based endoscopic suturing and medical adhesive helped achieve fistula closure in our case, and the combination guaranteed better outcomes than either method alone. In this case, the patient with tuberculous bronchoesophageal fistula was finally cured without severe complications. During her 1-year follow-up, the fistula did not recur. It can be concluded that the clinical success rate of tuberculous bronchoesophageal fistula closure will be effectively improved by our technique. Therefore, ESD-based endoscopic suturing is worth verifying through more clinical use, especially when other therapeutic options are not available or acceptable.
In conclusion, tuberculous bronchoesophageal fistula is a rare but troublesome and severe complication. Although there are multiple treatment options, some planned treatments may fail, and patients may reject potentially effective therapies. Therefore, it is necessary to continuously improve endoscopic methods to meet the needs of different patients. To our knowledge, this is the first use of the ESD technique in a patient with a bronchoesophageal fistula, and the ESD-based suture technique combined with a medical adhesive successfully managed this complicated case. This report may provide new alternatives and practical ideas for patients with bronchoesophageal fistula or another complex gastrointestinal fistulas.