
Abstract
The placenta is a transitory organ indispensable for normal fetal maturation and growth. Recognition of abnormal placental variants is important in clinical practice, and a broader understanding of the significance of placental variants would help clinicians better manage affected pregnancies. Increased thickness of the placenta is reported to be a nonspecific finding but it is associated with many maternal and fetal abnormalities, including preeclampsia and abnormal fetal growth. In this review, we address the questions regarding the characteristics of placenta thickness and the relationship between thickened placenta and poor pregnancy outcomes.
Keywords
Introduction
The placenta is the interface between the mother and the fetus. It supports fetal development by providing oxygen and nutrients from maternal blood and excreting carbon dioxide and waste metabolic products during intrauterine life.1,2 It also protects the fetus from infections and noxious agents and secretes hormones into the maternal circulation.1,2 Abnormalities of the placenta can cause prenatal complications for both the mother and the fetus and affect the postnatal health profile of the newborn.
It is vitally important to recognize placental variants that might indicate potential problems for the mother or fetus. Placental thickness (PT) is a gross morphological parameter in prenatal programming, and changes in PT have been observed in association with many abnormal conditions. For instance, reduced PT can be found in fetal growth restriction and systemic vascular disorders,3,4 and increased PT can be observed in preeclampsia, gestational diabetes mellitus (GDM), maternal anemia, fetal hydrops, and antepartum infections.5–8 Previous studies suggest that abnormal PT may be a warning sign of prenatal complications.
Considering the indispensable role of the placenta in the optimal course of gestation, the current study aimed to summarize the characteristics of PT in singleton pregnancies and its reference values in prenatal health care.
Definitions
“Thick placenta” is generally a sonographic term. The cutoff value to define thick placenta varies with gestational age (GA), measurement approaches, and conditions of the mother and the fetus. Several studies have evaluated the applicability of sonographic screening of PT in different trimesters and shown a positive linear relationship between GA and PT (Table 1).6,9–20
Review of the literature on increased placental thickness
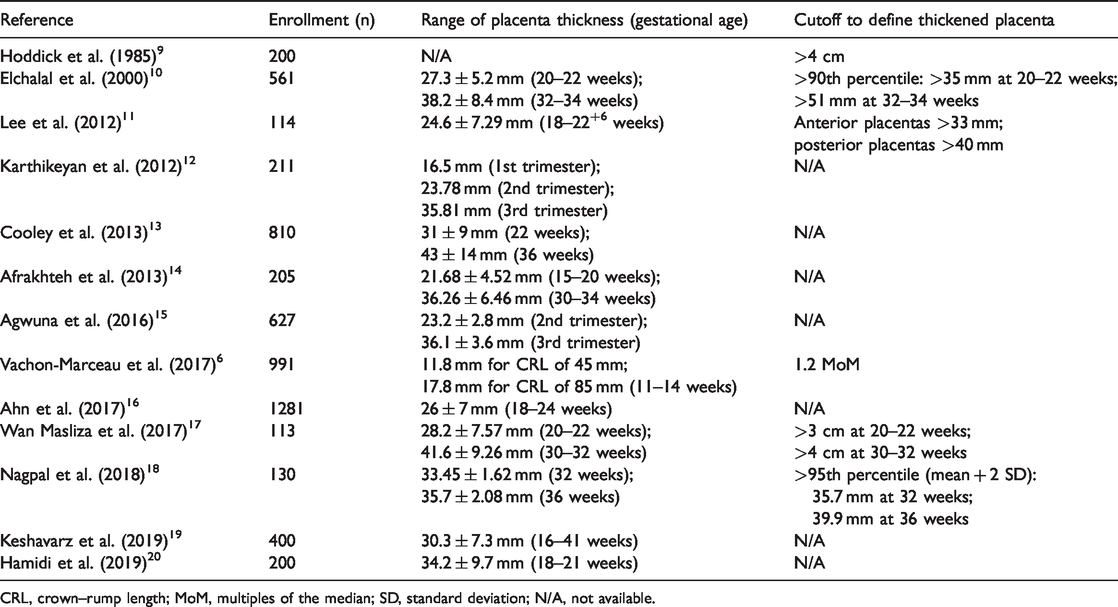
CRL, crown–rump length; MoM, multiples of the median; SD, standard deviation; N/A, not available.
Regarding published cutoff values of abnormal PT, Hoddick et al., La Torre et al., and Dombrowski et al. all state that PT should not exceed 40 mm at any stage of gestation.9,21,22 In the study of Elchalal et al., 10 thick placenta (above 90th percentile) was defined as a placenta thicker than 35 mm at 20 to 22 gestational weeks and thicker than 51 mm at 32 to 34 gestational weeks. The implantation site of the placenta may also affect PT. Lee et al. 11 indicated that anterior placentas were approximately 6 to 7 mm thinner than posterior or fundal placentas. They also suggested that an anterior placenta >33 mm and a posterior placenta >40 mm in the second trimester would be considered abnormally thick. Although there is no widely acknowledged definition of thickened placenta, clinicians should be alert and aware of the possibility of compromised perinatal outcome if the PT is >40 mm. In addition, if there is suspicion for thickened placenta, magnetic resonance imaging (MRI) can be useful in evaluating PT and associated abnormalities.
Ultrasound findings
Thickened placenta is usually identified by ultrasound, with a prevalence ranging from 0.6% to 7.8% according to in the literature.23,24 In most cases, sonographers measure PT in the sagittal view from the fetal side of the echogenic chorionic plate to the maternal side of the placental–myometrial interface in the area of the placental cord insertion if it is centric or <2 cm eccentric.9,10 When the placental cord insertion is marginal or velamentous, the maximum thickness may be calculated in a linear fashion in the placenta longitudinal plane. 10
Sonographic features of a thickened placenta reported in the literature include10,15,25,26 (1) “jelly-like” placenta with patchy decrease of echogenicity; (2) gigantic enlargement with multiple sonolucent spaces of different sizes and shapes (Swiss cheese); (3) placenta lakes with large sonolucent spaces surrounded by normal placental tissue; (4) placental masses of variable echogenicity; (5) and cord masses with central echo-dense zone and peripheral hypoechoic areas.
Risk factors
The placenta is a fetal organ developing from the chorionic villi at about the fifth week of gestation. 27 Placenta abnormalities can affect the health of the mother and the fetus; similarly, any pathological changes in mother and fetus can also have a great effect on the placenta. A few studies have identified some pathological characteristics of thickened placenta that might be a result of abnormal maternal, fetal, or placental conditions, such as placenta infarction, intervillous thrombosis, inflammation, perivillous fibrin deposition, or compensatory hyperplasia.28–31 Thickened placenta is not diagnostic of any specific fetal or maternal disorder but might be indicative of an at-risk pregnancy and warrants close management. 10
Maternal conditions
Several maternal complications can lead to sonographic abnormalities of PT, including preeclampsia, diabetes mellitus (DM), anemia, cytomegalovirus (CMV) infection, Toxoplasma gondii infection, or syphilis.31–39 Increased PT may be induced by preeclampsia via reactive changes in placenta villi to ischemia, along with increased secretion of trophoblast-derived proteins in maternal blood, such as human chorionic gonadotropin, activin, and inhibin. 30 Such changes might lead to an antiangiogenic state and reciprocally trigger preeclampsia. 31 A previous study showed a positive trend between PT and subsequent development of preeclampsia; thick placenta was a significant risk factor. A prospective cohort study with 991 participants showed that pregnancies that developed preeclampsia tended to have greater PT, with values >1.2 multiples of the median (MoM) in the first trimester. 6 Similar results were shown in another cohort study, in which pregnancies with preterm and term preeclampsia tended to have thicker placentas, with values of approximately 1.7 and 1.4 MoM, respectively. 32 Thus, when ultrasound indicates an abnormally thickened placenta, close monitoring of the blood pressure trend of the mother are recommended.
Maternal DM, including GDM and pregestational DM, is also associated with placentomegaly combined with edematous villous stroma, capillary proliferation, and insertion of newly formed vessels and increased surface area as a compensatory mechanism. 33 Additionally, maternal infection is a concerning problem during gestation. Viruses and bacteria can be transmitted into the fetus through the placenta, and pathogens in the placenta can destroy vascular remodeling and cause fibrosis and inflammatory response, resulting in placenta dysfunction.34,35 A study by Pomar et al. 36 showed that placentas infected by Zika virus were significantly thicker than uninfected placentas, and placentomegaly presented earlier in infected placentas. Among pregnancies with CMV infection, PT was increased in approximately 93.3% of the subjects. In conclusion, placentomegaly may be an early sign of maternal complications before clinical symptoms or other adverse outcomes become apparent, warranting enhanced prenatal follow-up of potentially affected pregnancies.
Fetal risk factors
Early detection of pregnancies with congenital anomalies is one of the current aims of fetal medicine. A few studies have suggested that the placenta might be a sentinel organ that can be affected by chromosomal abnormalities, immune and nonimmune hydrops fetalis, and Beckwith–Wiedemann syndrome.40–45 Homozygous α-thalassemia-1, also known as hemoglobin Bart’s (Hb Bart’s) disease, is a common cause of hydrops fetalis. Fetuses affected by Hb Bart’s disease develop severe anemia, leading to hydropic changes that cause thickened placenta and cardiomegaly.40,41 As Ghosh et al. 40 suggested, the increase in PT can occur as early as 10 weeks of gestation. A study by Tongsong et al. 41 found that the mean PT between 18 and 21 weeks in healthy pregnant women was 24.6 ± 5.2 mm, whereas that in women with Hb Bart’s disease was 34.5 ± 6.7 mm. The thickened placenta may also influence fetal outcomes. As Elchalal et al. noted, thick placenta may be associated with an increased incidence of either macrosomia or small-for-gestational-age infants at term, as well as increased perinatal mortality. 10 However, some studies did not show a significant association between PT and fetal outcomes. Hamidi et al. 20 indicated no association between PT and admission to the neonatal intensive care unit, low Apgar score, or medical comorbidities. Although the role of a thick placenta in fetal outcomes is controversial, measurement of PT may aid in the differentiation of normal and high-risk pregnancies, with the simple application of routine sonography.
Placental-related diseases
Placental-related diseases also contribute to sonographically thickened placenta, including placental chorioangioma, chorioangiomatosis, cord angiomyxoma, subamniotic hematomas, placental lakes, and placental abruption.25,26,46–50 Placenta abruption is one of the most serious complications of pregnancy, and it is commonly associated with premature labor and delivery and higher rates of perinatal death. Sonographic imaging shows retroplacental hematoma and increased PT.46,47 As Miwa et al. 47 reported, the prevalence of placental abruption is significantly higher in pregnancies with thickened placenta than in pregnancies with normal PT. The finding of placental lakes was reported to be six times more likely with a thick placenta (>3 cm) at 20 weeks’ gestation but was not associated with uteroplacental complications or adverse pregnancy outcomes. 24 Placental mesenchymal dysplasia (PMD) is a rare and oncologically benign anomaly of the placenta that closely resembles molar pregnancy on ultrasound but has no risk of malignant trophoblastic disease. PMD is characterized by placentomegaly with cystic vesicles, dilated chorionic blood vessels, and mesenchymal hyperplasia without trophoblastic proliferation.49,50 When a thick placenta is identified, placental-related abnormalities should be considered, especially when maternal and fetal abnormalities are ruled out.
Management
According to the above data, it is appropriate to consider pregnancies with thick placentas as being at risk and to perform a complete sonographic evaluation. Because of its higher contrast resolution and tissue-specific characterization, MRI may be beneficial to rule out coexistent anomalies. For obstetricians, it would be helpful to complete a full review of medical records, conduct a physical examination, and run blood tests such as a complete blood count, TORCH screen (toxoplasmosis, rubella, CMV, herpes simplex, and HIV), or HIV and syphilis testing. For instance, if ultrasound indicates a partially thickened placenta and the patient complains of abdominal pain or vaginal bleeding, placenta abruption should be strongly suspected. If placenta abruption is ruled out, then placental complications should be considered, such as placental chorioangioma, cord angiomyxoma, and subamniotic hematomas. When a diffused thickened placenta is identified sonographically, clinicians should be aware of maternal or fetal complications and perform a close follow-up.
Conclusion
Even though increased PT is not diagnostic of any specific disorders, it may be a potent predictor of high-risk pregnancies, including preeclampsia, GDM, and hydrops fetalis. Enhanced follow-up of patients with suspected placentomegaly should be performed. The significance of abnormal morphological findings of the placenta on ultrasound remains unclear because of scarce information on the pathophysiological and clinical effects of placentomegaly. Large-scale studies are needed to explore the clinical importance of abnormal placental thickness.