
Abstract
Retinal detachment caused by severe ocular trauma is a type of refractory vitreoretinal disease. Current treatment methods include vitrectomy combined with silicone oil tamponade. However, long-term use of silicone oil tamponade has various complications, including a risk of silicone oil dependence that eventually leads to eyeball atrophy and enucleation. Foldable capsular vitreous bodies (FCVBs) offer a good solution for these problems. However, FCVBs have not been used in large-scale clinical applications and few cases have been reported in the published literature. The main use of FCVBs, based on current evidence, is in the treatment of the relatively few (but important) patients whose eyes have no visual potential; the aim of treatment in these patients is globe preservation, rather than restoration of vision. Here, we describe two patients who underwent FCVB implantation. The findings in these patients indicated that FCVBs can effectively support the vitreous cavity and detached retina. FCVB implantation may thus offer a safe and effective method for treatment of severe retinal detachment, avoiding the inconvenience caused by silicone oil dependence and enucleation. To confirm its long-term usefulness in clinical applications, many additional case reports are needed.
Keywords
Introduction
Severe ocular trauma can lead to structural damage and atrophy of the eyeball. Retinal detachment caused by severe trauma reportedly has a 30% incidence and is associated with poor prognosis. 1 Because of the complex traumas experienced by many patients, pars plana vitrectomy with silicone oil (SO) tamponade is the primary surgical treatment approach. 2 SO tamponade can support the eyeball, but subsequent retinal detachment may occur. 3 Repeated retinal detachment will lead to SO dependence, 4 which requires extended maintenance of the prone position. Long-term SO tamponade can lead to complications such as corneal degeneration, emulsification, cataracts,5,6 early hypertension, and secondary glaucoma.7,8 Studies concerning the effects of long-term SO tamponade on intraocular pressure (IOP) have implied that this treatment may lead to reduced choroidal thickness;9–11 SO‐related retinal toxicity and visual loss have also been observed.6,12 SO emulsification is the most important limitation of long-term in situ SO tamponade because it is considered a fundamental source of SO-related complications. 5 Emulsification is associated with the development of keratopathy, delayed glaucoma, and optic neuropathy through mechanisms including emulsion oil droplet contact with the corneal endothelium, trabecular network inflammation, and direct SO infiltration into the atrial angular structure. Despite its complications, SO tamponade remains suitable for patients with severe ocular trauma. 13 The main alternative treatment option is enucleation, which causes extensive physical injury and mental distress. Thus, other novel vitreous substitutes are needed.
Foldable capsular vitreous bodies (FCVBs) are novel vitreous substitutes that can effectively maintain the eyeball appearance, avoid enucleation, preserve residual visual acuity, and prevent SO-related complications. FCVBs have been explored for clinical applications in China and several European countries; the preliminary findings have been good.14–19 The main indications for FCVBs are best-corrected visual acuity (BCVA) ≤0.05; intraocular axial length of 16 to 28 mm; severe unilateral retinal detachment that is untreatable with an existing vitreous replacement, presumably caused by severe trauma with complex retinal detachment and/or choroidal detachment; irreparable large posterior scleral laceration of the unilateral eyeball; and the inability to remove SO after long-term tamponade, with incomplete retinal reattachment. Patients with no light perception should be the first choice. To our knowledge, there have been few clinical reports of FCVBs in patients with severe ocular trauma. Here, we describe two patients with traumatic retinal detachment who received FCVB treatment; our findings may provide a basis for further clinical implementation of FCVB treatment.
Case reports
Case 1
A 31-year-old man was injured by direct impact with a hockey puck over the left eye and underwent vitrectomy with combined phacofragmentation in our hospital. Two months after the surgery, his left eye exhibited retinal detachment in the form of rigid folds with a large number of proliferative membranes. The patient was young and could not maintain the prone position for long periods because of work obligations, so he refused treatments of SO tamponade and enucleation; he requested FCVB implantation. At that time, his BCVA results were light perception in the left eye and 10/10 in the right eye. His IOP results were 10 mmHg in the left eye and 16 mmHg in the right eye. Anterior segment examination showed large organic membranes on the iris, while the lens was entirely absent. Fundoscopy, fundus photography (Figure 1), and B-scan ultrasound (Figure 2) examinations all showed extensive retinal detachment in the patient’s left eye. Therefore, the patient provided written informed consent to undergo SO-filled FCVB implantation in the left eye. The specific surgical treatment that the patient underwent is described in Figure 3.

Preoperative fundus photography. Color fundus photo depicting detached retina in the left eye of the patient in case 1, prior to surgical management.

Preoperative B-scan ultrasound. Scan shows retinal detachment and microphthalmos in the left eye of the patient in case 1, prior to surgical management.

Foldable capsular vitreous body (FCVB) implantation procedure. (a) Creation of approximately 4-mm-long scleral incision. (b) Folding of the FCVB, three times prior to insertion. (c) Manual implantation of the FCVB into the vitreous cavity. (d) Injection of silicone into the capsule to support the retina. (e) Fixation of the FCVB valve to the scleral surface. (f) Suturing of the conjunctiva to cover the FCVB.
On the first day postoperatively, BCVA in the patient’s left eye remained light perception, while the IOP was 15 mmHg. Fundoscopy showed that the FCVB was appropriately positioned and the retina was attached. At 3 months postoperatively, the cornea was slightly opaque and exhibited keratic precipitates. The FCVB remained appropriately positioned with respect to the retina and showed a firm connection to the inner scleral wall; the IOP at the time was 10 mmHg. Topical corticosteroids were administered as anti-inflammatory therapy. At 9 months postoperatively, as shown in Figure 4, persistent corneal opacity was evident with new-onset neovascularization and a thick anterior chamber exudative membrane; no other intraocular structures were visible. IOP in the patient’s left eye was 10 mmHg, while the BCVA remained light perception. B-scan ultrasound showed pseudo expansion of the eyeball with the FCVB appropriately spread in the vitreous cavity and no obvious abnormalities (Figure 5). In the postoperative period, the only complications were corneal opacity and anterior chamber exudative membrane. Overall, the patient was completely satisfied with the postoperative outcome. Because the patient resided far from our hospital and considered the outcome to be adequate, he declined any long-term follow-up treatment.

Anterior segment photography performed at 9 months after foldable capsular vitreous body implantation. Photos show opacification of the cornea with membrane material in the anterior chamber, precluding clinical examination of other intraocular structures in the patient in case 1.

B-scan ultrasound performed at 9 months postoperatively. Scans show the relative stability of the implanted foldable capsular vitreous body implant at 9 months postoperatively in the patient in case 1.
Case 2
A 34-year-old man was admitted to our hospital because of pain in the right eye that had been present for 1 month. The patient's right eye had been injured by an iron sheet 10 years prior and he had undergone right eye surgery in a local hospital at that time. Upon admission to our hospital, physical examination of the patient showed BCVA findings of no light perception in the right eye and 10/10 in the left eye. The IOP was moderately elevated in the patient’s right eye, as determined by finger palpation (corneal edema and turbidity prevented conventional tonometry assessment); it was 20 mmHg in the left eye. Anterior segment examination showed bulbar conjunctival hyperemia, corneal edema and opacity, and hyphema (Figure 6). Preoperative B-scan ultrasound showed that most of the iris was missing from the right eye; moreover, the lens was absent, the anterior chamber and vitreous exhibited hemorrhage, and retinal detachment was evident (Figure 7). Because the patient’s medical condition was serious, his postoperative prognosis was not good; therefore, we recommended observation and symptomatic treatment for IOP reduction, but no immediate surgical treatment. However, the patient insisted that surgery was necessary due to eye pain. Because of his young age, he and his family could not accept enucleation and refused SO tamponade; thus, the available treatment comprised intensive FCVB implantation. In accordance with the patient's preferences and surgical consent, vitrectomy combined with SO-filled FCVB implantation was performed.

Preoperative anterior segment photography. Photo shows bulbar conjunctival hyperemia, corneal edema and opacity, and hyphema in the patient in case 2.

Preoperative B-scan ultrasound. Scans show that most of the iris in the right eye is missing, lens is absent, anterior chamber and vitreous are hemorrhaged, and retina is detached in the patient in case 2.
The patient’s IOP was 16 mmHg in the right eye on the first day postoperatively; furthermore, the corneal endothelium was wrinkled, while hyphema and exudation were observed in the anterior chamber. At 8 days postoperatively, the IOP in the right eye was 11 mmHg, corneal endothelial folds were reduced, and the anterior chamber hyphema and exudation were diminished. At 1 month postoperatively, the anterior chamber hyphema and exudation were significantly reduced (Figure 8). The IOP in the right eye was 12 mmHg, while BCVA in the right eye remained no light perception. B-scan ultrasound examination indicated pseudo expansion of the eyeball, while the FCVB was suitably spread in the vitreous cavity (Figure 9). Fundus photography showed that the FCVB was transparent and appropriately positioned, while the retina was faintly visible without obvious wrinkles (Figure 10). Additionally, no obvious complications were observed at 1 month postoperatively. The treated eye had a good physical appearance and was symmetrical with the contralateral eye. The patient’s eyeball was preserved, thus avoiding the physical injury and mental distress caused by enucleation or SO dependence. The patient was completely satisfied with the postoperative outcome. Because the patient resided far from our hospital and considered the outcome to be adequate, he declined any long-term follow-up treatment.

Anterior segment photography performed at 1 month postoperatively. Photo shows that hyphema and exudation in the anterior chamber are significantly reduced in the patient in case 2.

B-scan ultrasound performed at 1 month postoperatively. Scans indicate that pseudo expansion of the eyeball, while the foldable capsular vitreous body has appropriately spread in the vitreous cavity in the patient in case 2.
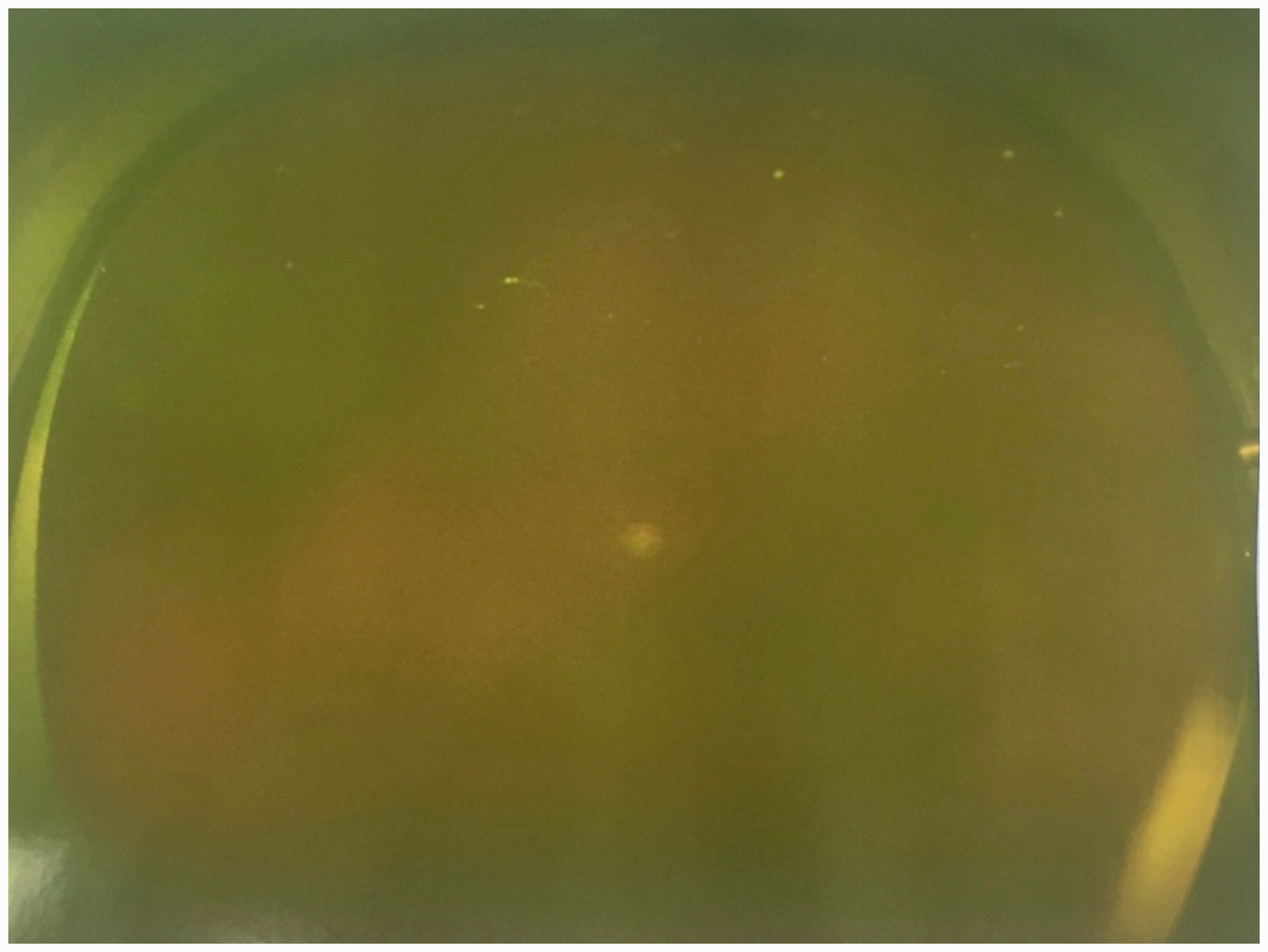
Fundus photography performed at 1 month postoperatively. Photo shows that the foldable capsular vitreous body is transparent and appropriately positioned, while the retina is faintly visible without obvious wrinkles in the patient in case 2.
Discussion
FCVBs are innovative vitreous substitutes developed in China. They consist of specially modified liquid silicone rubber with several features: a capsule, drainage tube, and drainage valve. 14 They can be filled with SO, balanced salt solution, or hydrogels after intraocular implantation.20–23 In contrast to the surface tension support provided by conventional vitreous substitutes (e.g., SO), FCVBs provide a 360-degree solid arc through their analogous solid strength, such that they can support retinal breaks and detachment in any direction. 15 Therefore, FCVBs can avoid the unique postoperative positioning requirements and alleviate the physical discomfort caused by use of the prone position. In addition, because of capsule membrane limitations, FCVBs can provide a cell barrier function, effectively avoiding SO emulsification and SO entry into the anterior chamber, as well as other complications.14–16,18,22 An FCVB device is depicted in Figure 11.
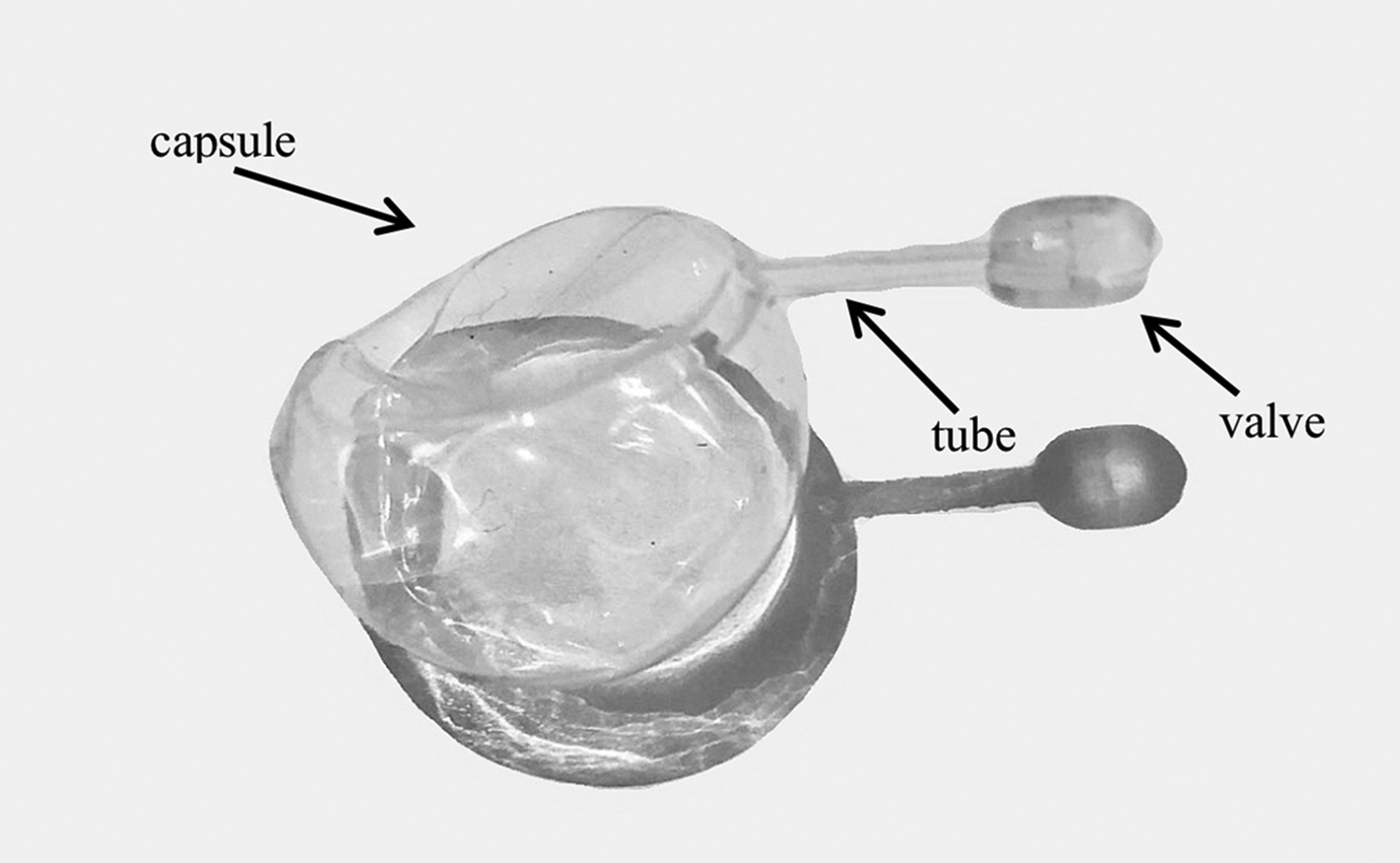
Illustration of human foldable capsular vitreous body. Photo shows that the foldable capsular vitreous body implant is composed of a capsule, drainage tube, and drainage valve.
In early in vivo, in vitro, and animal studies, FCVBs have shown good physical properties, optical properties, and biocompatibility.21,22,24 However, FCVBs have not been widely promoted in clinical practice. Thus far, FCVBs are emerging vitreous substitutes; evidence from basic and preliminary clinical research has shown that the most appropriate application is in the treatment of the relatively few (but important) patients with no visual potential in one or both eyes. 15 In those patients, the aim of treatment is globe preservation, rather than vision restoration. Because such conditions are generally rare, this treatment has not been widely used in clinical practice. To the best of our knowledge, there have been few reports concerning the clinical effects of FCVBs, with the exception of exploratory analyses of its early-stage clinical applications. Lin et al. 16 performed FCVB implantation in 11 patients with severe retinal detachment, then followed those patients for 3 months; the results indicated that FCVBs were flexible, effective, and safe vitreous substitutes. In addition, Lin et al. 16 reported that FCVBs could be easily removed from the vitreous cavity through a 2-mm scleral incision. A 1-year exploratory analysis of SO-filled FCVB treatment for severe retinal detachment showed that FCVBs had good efficacy and safety. 15 Furthermore, hydrolysis stability examination showed that SO-filled FCVBs were more inert and less corrosive than FCVBs filled with balanced salt solution. A 3-year analysis demonstrated the effectiveness and safety of SO-filled FCVBs as a vitreous substitute; 17 importantly, complications (e.g., SO emulsification and migration) could be effectively avoided.
In a recent study, Zhang et al. 18 performed vitrectomy combined with FCVB implantation in 20 patients with severe ocular trauma or SO-dependent eyes, then conducted 1-year follow-up observations in all patients. The results showed that FCVBs provided good support in all treated eyes; six treated eyes achieved retinal reattachment. After treatment, there was a statistically significant elevation of IOP (from 12.90 ± 7.06 mmHg preoperatively to 15.15 ± 3.36 mmHg postoperatively). While two eyes had complications of keratopathy (one eye) and intraocular inflammation (one eye), all other eyes had good postoperative results and maintained a satisfactory ocular appearance without severe ocular atrophy. In addition, no complications of SO emulsification or leakage were observed. However, postoperative BCVA was not improved, compared with preoperative BCVA, which was consistent with our findings in the current report. The study by Zhang et al. 18 also included three pediatric patients whose IOP was restored and eye appearance was preserved after FCVB implantation, thereby demonstrating the potential for use of FCVBs as ideal vitreous substitutes to restore eyeball structure and maintain the desired appearance and esthetic characteristics.
In addition, FCVB capsules have 300-nm holes, 25 providing a structural basis for their use in sustained release of drugs. A number of studies have successfully used FCVBs for sustained release of various drugs (e.g., dexamethasone 25 and levofloxacin26–28) and experimental molecules (e.g., small interfering RNA–protein kinase Cα 29 and 5-fluorouracil 30 ). Therefore, FCVBs may be useful in both drug sustained-release systems and vitreous substitutes, such that they can aid in the treatment of bacterial endophthalmitis and proliferative vitreous retinopathy. Notably, Chen et al. 23 found that the application of FCVBs could prolong the retention time of polyethylene glycol. Feng et al. 31 also showed that the application of FCVBs could extend the duration of intraocular polyvinylalcohol hydrogel tamponade use. Therefore, the combination of FCVBs with hydrogels may address the limitations of hydrogels as vitreous substitutes with high toxicity and rapid degradation, which may be an important direction for future investigations of vitreous substitutes.
Notably, no obvious complications occurred during short-term observation of either patient in this report, while longer-term observation of the patient in case 1 revealed the formation of a thick exudate membrane. We do not know whether this complication is related to the disease severity or individual differences in physical conditions, or whether it is associated with the increased intraocular stimulation caused by long-term FCVB implantation. Because of the small number of patients and short observation periods in this report, a longer follow-up study and additional clinical assessments are needed to confirm the efficacy of FCVBs in similar patients.
Our findings showed that FCVBs can support the eyeball, effectively maintaining eyeball appearance, while avoiding atrophy and enucleation. Furthermore, the use of FCVBs prevents the prone position requirement after surgery, greatly reducing pain in affected patients. The two patients who underwent FCVB implantation in this report were satisfied with their postoperative results. However, there are some limitations of this technique, in that it cannot improve vision and only provides stents for the eyeball; moreover, it can lead to the onset of postoperative exudation. Nonetheless, we found that FCVBs demonstrated good efficacy and safety in two patients with severe retinal detachment who wanted to preserve their eyeball appearance and avoid enucleation. FCVBs offer a potentially effective and safe treatment method, but their long-term clinical applications require further establishment via long-term analyses of a large number of patients.
Footnotes
Informed consent
Both patients provided written informed consent for the publication of this information and the accompanying images.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation (81970836), the International Cooperation Project of Science and Technology Department of Jilin Province (20190701044GH), the Training Program for Outstanding Young Teachers of Jilin University (419080520313), and the Natural Science Foundation Project of Science and Technology Department of Jilin Province (20200201360JC).