
Abstract
Objective
To begin to understand how to prevent deep vein thrombosis (DVT) after an innovative operation termed intracorporeal laparoscopic reconstruction of detenial sigmoid neobladder, we explored the factors that influence DVT following surgery, with the aim of constructing a model for predicting DVT occurrence.
Methods
This retrospective study included 151 bladder cancer patients who underwent intracorporeal laparoscopic reconstruction of detenial sigmoid neobladder. Data describing general clinical characteristics and other common parameters were collected and analyzed. Thereafter, we generated model evaluation curves and finally cross-validated their extrapolations.
Results
Age and body mass index were risk factors for DVT, whereas postoperative use of hemostatic agents and postoperative passive muscle massage were significant protective factors. Model evaluation curves showed that the model had high accuracy and little bias. Cross-validation affirmed the accuracy of our model.
Conclusion
The prediction model constructed herein was highly accurate and had little bias; thus, it can be used to predict the likelihood of developing DVT after surgery.
Keywords
Introduction
Bladder cancer is one of the most common malignancies of the urinary system and the fourth most common cancer type in men; bladder cancer is also common in women. 1 Radical cystectomy with appropriate urinary diversion is the gold standard treatment for patients with non-metastatic musculoinvasive bladder cancer who are eligible for surgery. This operation is favored by doctors and patients owing to its efficacy at improving quality of life after surgery.2,3
Previous studies have shown that most hospitals choose the ileum as the route of urinary diversion.2–4 In 2000, our center launched a new improvement, called laparoscopic reconstruction of detenial sigmoid neobladder, for bladder cancer treatment. The efficacy of laparoscopic reconstruction of detenial sigmoid neobladder at our hospital has already been documented. 5 However, the operation is an extreme stress that can necessitate interventions to prevent the development of postoperative deep vein thrombosis (DVT). These interventions require cooperation from the patient, nursing staff, and the doctor. 6 To date, approaches for preventing DVT development are limited. Therefore, we sought to identify risk and protective factors for DVT following laparoscopic reconstruction of detenial sigmoid neobladder to then construct a prediction model to guide clinical practice.
Materials and methods
Clinical data
The reporting of this study conforms to the STROBE guidelines. 7 This retrospective study included consecutive patients who underwent laparoscopic reconstruction of detenial sigmoid neobladder at our hospital since 2017, as previously described. 8 Owing to the relatively small sample size, all subjects were included in the analysis; there were no exclusion criteria. The endpoint was postoperative DVT development. Thrombosis was detected by color doppler ultrasound sonography, otherwise it was negative. This study was conducted according to guidelines approved by the Medical Ethics Committee of ZhuJiang Hospital, Southern Medical University (approval number: 20191114152431480, 14 November 2019). Given the retrospective nature of this work, an exemption for informed consent for this was study was approved by the hospital review board. All patient details have been de-identified.
Observation indexes
Data on general patient characteristics and disease variables were collected for all patients. The general characteristics included sex, body mass index (BMI), age at surgery, smoking history, DVT history, and family DVT history. Disease and related variables included postoperative use of hemostatic agents, anticoagulants, vasoconstrictors, and any other special treatment, postoperative intensive care unit (ICU) stay, preoperative presence of diseases, use of an artificial anal sphincter, presence of gastrointestinal decompression, use of postoperative oral lubricant guide, history of postoperative passive muscle massage, pressure treatment time, and activity level on the first postoperative day.
Statistical analysis
Patients were divided into two groups on the basis of final DVT outcomes: thrombosis or no thrombosis. The data were then subjected to logistic univariate analysis, which was performed using SPSS version 19.0 software (IBM Corp., Armonk, NY, USA). Apart from age, all other variables were compared using the independent t-test or R*C chi-square test, with P < 0.25 considered statistically significant. Because logistic univariate analysis is flexible in selecting target variables, it can select relevant factors that actually need to be studied in clinical research. 9 Statistically significant factors from the univariate analysis were selected and subjected to multivariate regression, at a significance level of P < 0.05. These factors were then used to construct a prediction model. The area under the receiver operating characteristic (ROC) curve (AUC) of each factor in the model and joint probability ROC curves were generated using GraphPad Prism 7.0 software (GraphPad Software, Inc., San Diego, CA, USA), while decision curve analysis (DCA), AUC, and validation of model accuracy were performed using packages in R version 3.6.1. In this study, we selected a 5-fold cross-validation on the basis of the sample size to determine the predictive performance of the model because this is the most common method for solving clinical problems based on machine learning.10–12 In the first step, the data were randomly divided into five parts, one of which was randomly selected as the test set, while the remaining four were used as the training set for model training. In the second step, the process of selecting different test sets and training sets was repeated five times, such that each subset had a chance to be a test set and the rest could be training sets. A model was obtained from each training set, and the AUC was calculated. Then the model was used to test on the corresponding test set, with the AUC of the test set being measured. The third step was to calculate the average AUC of the five training and test sets as a performance index to evaluate model accuracy. Meanwhile, we observed whether the AUC of the test set was significantly changed compared with that of the training set to judge the accuracy and extrapolation of the model.
Results
Univariate analysis
In total, 151 consecutive patients who underwent laparoscopic reconstruction of detenial sigmoid neobladder at our hospital since 2017 were recruited into this study. Univariate analysis revealed that surgical age, BMI (18.5–23.9), preoperative smoking history, postoperative use of hemostatic drugs, no preoperative disease, preoperative diabetes, preoperative toxic hepatitis, postoperative passive muscle massage, and activity level on the first day after surgery were significant risk factors for DVT (P < 0.25) (Table 1).
Univariate analysis of all factors.

The univariate analysis methods included the T test and chi-square test; the T test was used for age and the chi-square test was used for other factors.*P < 0.25.
DVT, deep vein thrombosis; BMI, body mass index; PICC, peripherally inserted central venous catheter; CVC, central venous catheter; ICU, intensive care unit.
Multivariate analysis
The R programming language (www.r-project.org) was used to analyze all the relevant factors at the same time, and it showed that there were significant differences in the prediction models formed by four factors. After logistic regression, the four statistically significant factors were age at surgery, BMI (18.5–23.9), postoperative use of hemostatic drugs, and passive muscle massage (P < 0.05). These were therefore used to construct the prediction model. Among them, age at surgery and BMI (18.5–23.9) were risk factors, whereas postoperative use of hemostatic drugs and passive muscle massage were protective factors (Table 2).
Multivariate analysis.

Multivariate analysis means logistic multi-factor regression analysis.
*P < 0.05.
OR, odds ratio; 95%CI, 95% confidence interval; BMI, body mass index.
Model evaluation
Model evaluation is a prerequisite for effective clinical use. Models independently constructed using the four factors resulted in different ROC values (Figure 1), with varying specificities and sensitivities low diagnostic power. However, combining the four factors during model construction resulted in a high ROC value and superior diagnostic efficiency of up to 84.38%, which met the criteria for applying the predictive model in clinical practice. When the cutoff value was 0.1781, the constructed model had a sensitivity and specificity of 75.00% and 85.85%, respectively (Figure 2). We also applied DCA to evaluate the model across different aspects. The resulting AUC value revealed that the model’s diagnostic efficiency had significantly improved compared with those derived from single factors, and the trend of the curve was significantly away from the two coordinate axes, indicating that the model was highly accurate at predicting DVT (Figure 3).

Evaluation of the prediction model – receiver operating characteristic (ROC) curves under the independent action of each factor. The area under the curve of each independent factor did not have high diagnostic efficiency. Sensitivity is on the horizontal axis, specificity on the vertical axis.

Evaluation of the prediction model – receiver operating characteristic (ROC) curves. Several variables were fitted to construct a new disease prediction model. The new model had high diagnostic efficiency. Sensitivity is on the horizontal axis, specificity on the vertical axis.

Evaluation of the prediction model – decision curve analysis (DCA). Compared with the single factor model, the area under the curve of the new model was significantly increased and had higher diagnostic efficiency. The curve of the new model was far away from the two sides of the coordinate axis, indicating high accuracy.
Model validation
Model validation is critical prior to application in clinical practice. In this study, we employed R packages for five-fold cross-validation of our model. The average AUCs of the five training sets and test sets are shown in Table 3. The AUC of the prediction model was 0.873, while that of the training set was 0.872. The AUC of the prediction model did not significantly decrease compared with the training set, indicating that the newly constructed prediction model has high accuracy and extrapolation.
Cross-validation.
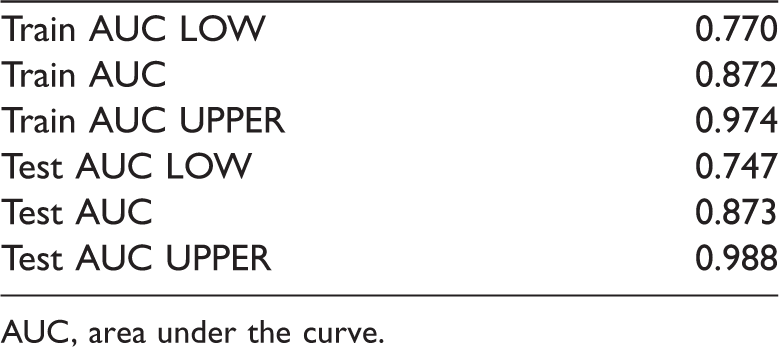
AUC, area under the curve.
Discussion
Because the laparoscopic reconstruction of detenial sigmoid neobladder operation was only launched at our hospital in 2000, many related postoperative nursing methods have not yet been defined, key among them being approaches on how to prevent DVT. In this study, we used logistic regression analysis to identify factors associated with DVT development. Our results showed that age, BMI (18.5–23.9), postoperative use of hemostatic drugs, and postoperative passive muscle massage were significantly correlated with thrombosis. Among them, age and BMI (18.5–23.9) were risk factors for occurrence, whereas use of postoperative hemostatic drugs and passive muscle massage were protective factors. We may be able to use these four factors to establish a model for predicting postoperative DVT development.
Age
Previous studies have shown that age is positively correlated with the incidence of DVT.13–16 Increased age is associated with loss of blood vessel elasticity, vascular wall damage, and other manifestations that contribute to the formation of thrombosis. 14 Previous data suggest that women over 55 and men over 65 years old are at a high risk of DVT. 14
The high DVT occurrence in older, relative to younger patients,14,17 may be attributed to factors such as blood stasis and hypercoagulability, which are rare in young patients.18–21 In younger patients, blood clots rarely develop on account of the well-functioning venous valve, a structure that prevents blood from flowing backwards, and normal regulation of the blood system. 15 Notably, our results revealed that age was still a risk factor for DVT under the new surgical procedure. Therefore, doctors are advised to pay attention to the postoperative care of older patients for effective disease management.
BMI
BMI is a commonly used clinical index to study the relationship between body weight and obesity. Numerous studies have shown that BMI is positively correlated with DVT, with obese patients exhibiting a significantly higher risk and severity of DVT relative to individuals with BMI in the normal range.22–24 A recent study showed that patients with BMI ≥30 have a significantly increased risk of DVT. 25 Conversely, our results showed that BMI in the normal range (18.5–23.9) was a risk factor for DVT after the aforementioned bladder surgery.
Several recent studies have found no association between patients with normal weight or those underweight with risk of DVT, possibly due to the occurrence of metabolic disorders.13,26,27 Notably, findings from animal studies have demonstrated that metabolic disorders in DVT are primarily related to energy metabolism, sphingolipid metabolism, and adenosine metabolism, although this conclusion was based on small sample sizes. 28 Therefore, BMI may not be the best choice for interpreting risk of DVT.
Postoperative use of hemostatic agents
Because this new operation uses suture recanalization between the urethra and the digestive tract, secretion of digestive juice and potential gastrointestinal bleeding is likely to occur after the operation. Therefore, many patients are administered somatostatin and other hemostatic drugs after surgery. 5
Our results demonstrated that postoperative hemostasis aided in preventing DVT development, which is contrary to conclusions from other studies that have recommended the use of anticoagulants. Functionally, somatostatin reduces visceral blood flow, increases vascular resistance, and promotes platelet aggregation to achieve hemostasis. 29 Previous studies have shown that thrombus development is associated with decreased activity of the anticoagulant system, increased activity of the procoagulant system, and reduced activation of the fibrinolytic system. There are two primary ways of activating the coagulation system: the tissue factor pathway and the contact pathway. Clotting factor VII and factor XII play a central role in thrombosis. 30 Recent studies have shown that somatostatin inhibits the activity of factors VII and VIII in patients with hyperglycemia and diabetes, thereby blocking activation of the procoagulant system activation and thrombogenesis. 31 As stated by van der Pas et al., 32 Protein S is regulated by somatostatin and may be an important mechanism through which somatostatin acts on the anticoagulant system. Additionally, a previous study cloned the DNA sequence encoding the murine somatostatin octreotide gene into the pET-28a–Δsak–Δsec2 and pET-28a–Δsec2–Δsak plasmids. 33 The fusion protein, when expressed and purified, showed the thrombolytic activity of Δsak, which specifically activates the fibrinolytic system. 33 Therefore, administration of somatostatin to prevent DVT after surgery may cause an adjustment between the aforementioned systems and different platelet aggregation mechanisms across different parts of the body.18,34 At the very least, postoperative use of hemostatic agents is not a risk factor for thrombosis. Therefore, we recommend using hemostatic drugs for patients with postoperative bleeding, as long as there are no contraindications.
Passive muscle massage
The modified operation involves the digestive system and urinary system; therefore, the ability of the patient to leave the bed is limited and bed rest is needed as much as possible to promote wound recovery and prevent bleeding. 5 Our results revealed that passive muscle massage, referred to as intermittent pneumatic compression (IPC) could prevent DVT development in patients lying in bed after the new procedure. The rate of veinous blood flow in bedridden patients may slow down, resulting in blood pooling, which is an important cause of DVT.18,35
Previous studies have shown that IPC can prevent DVT development by increasing activity of the systemic fibrinolytic system as well as levels of D-dimer and tissue factor pathway inhibitors in the blood. 36 In this study, we also compared postoperative IPC treatment time per day, and found no significant differences across groups of patients. Therefore, postoperative use of IPC in patients is an effective approach for preventing DVT, after the exclusion of contraindications, 37 regardless of the length of use.
Conclusion
Clinicians performing laparoscopic reconstruction of detenial sigmoid neobladder may need to pay close attention to older patients and those with a normal BMI (18.5–23.9) and consider postoperative hemostatic drugs and postoperative IPC to effectively prevent postoperative DVT development. Future explorations will evaluate the relationship between this improved surgical procedure with DVT development using a larger patient cohort.
Footnotes
Author contributions
XL conceived the study; YL and XL contributed to the research design; all authors were involved in data collection; and YL coordinated funding for the project.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article:This work was supported by grants from the Medical Science and Technology Research Foundation of Guangdong Province (No. B2020137).