
Abstract
A Hoffa fracture is a rare intra-articular injury consisting of a coronal plane fracture of one or both of the distal femoral condyles. Because of the rarity of medial Hoffa fractures, only a few reports have described this injury and its arthroscopic management. In this article, we present a rare case involving a 32-year-old man with a displaced medial Hoffa fracture associated with a proximal anterior cruciate ligament tear. He was treated by a single-stage fully all-inside arthroscopic technique. Arthroscopic-assisted internal fixation ensured fragment stability and enabled us to visualize the fracture reduction, monitor the screw insertion, and reconstruct the anterior cruciate ligament tear at the same time. This technique is a novel but demanding treatment method for medial Hoffa fractures and is particularly useful for properly selected patients with associated intra-articular knee injuries.
Keywords
Introduction
A Hoffa fracture is an uncommon intra-articular injury consisting of a coronal plane fracture of one or both of the distal femoral condyles. The main mechanism of injury is a concentration of shear stress that acts on the posterior half of the femoral condyle when the knee is in a flexed position. Although either femoral condyle can be involved, Hoffa fractures of the lateral femoral condyle are three times more common than those of the medial condyle. 1 Because of the rarity of medial Hoffa fractures, only a few reports have described this injury and its management,2,3 and fractures with associated intra-articular knee injuries are even rarer.
Because a Hoffa fracture is an intrinsically unstable intra-articular fracture, operative fixation is often required to achieve anatomical reduction of the articular surface and prevent future development of post-traumatic arthritis. 4 Hoffa fractures are conventionally treated with open reduction and internal fixation using a plate or headless compression screws. 5 Only a few reports have described attempts to fix medial Hoffa fractures using an arthroscopic-assisted procedure.6,7 No reports to date have described a fully arthroscopic technique for medial Hoffa fractures with concomitant intra-articular injuries. We herein present a rare case of a medial Hoffa fracture associated with an anterior cruciate ligament (ACL) tear treated using a single-stage fully all-inside arthroscopic approach.
Case report
The reporting of this study conforms to the CARE guidelines. 8
A 32-year-old man who had been involved in a traffic accident was admitted to a community hospital immediately after injury. He had severe left knee pain with a visual analog scale score of 8 points. The general practitioner found no obvious abnormalities on the initial X-ray image. Analgesics were administered, but the patient was still unable to walk for the next several days. Therefore, he presented to us 7 days after injury with persistent left knee pain and disability of weight bearing. The patient had no history of drug allergy, other major diseases, or hospitalization. He denied any significant family history of disease. In addition, no history of trauma to his left knee was noted. Physical examination revealed significant swelling, extensive tenderness, and limited range of motion of his left knee. The anterior drawer test and Lachman test were positive during the examination. Anteroposterior and lateral radiographs showed an occult medial Hoffa fracture (Figure 1). Computed tomography (CT) demonstrated a displaced medial Hoffa fracture of Letenneur type III 9 (Figure 2(a)). Magnetic resonance imaging (MRI) revealed a medial Hoffa fracture associated with an ACL tear (Figure 2(b)). Therefore, the patient was diagnosed with a medial Hoffa fracture combined with an ipsilateral ACL tear.

(a) Anteroposterior and (b) lateral radiographs of the left knee. The arrow shows an occult medial Hoffa fracture.

(a) Computed tomography of the left knee showed a displaced medial Hoffa fracture. (b) Magnetic resonance imaging showed a complete anterior cruciate ligament tear (arrow).
The patient was placed in the supine position under spinal anesthesia. Using standard anteromedial and anterolateral portals, a complete diagnostic arthroscopic examination was performed to identify associated intra-articular injuries with the aid of a tourniquet. After removal of the hematoma, a displaced coronal fracture of the medial femoral condyle with a concomitant proximal ACL tear was confirmed. The posterior cruciate ligament and the meniscus were intact.
By flexing the knee to 120°, the fracture was fully reduced with the aid of a curved probe. A percutaneous K-wire was percutaneously inserted in the anterior-to-posterior direction to temporarily stabilize the fracture. Under arthroscopic control, two additional percutaneous guide pins were inserted parallelly into the medial aspect of the suprapatellar bursa, perpendicular to the fracture line (Figure 3(a)). These pins were carefully placed to avoid penetration into the medial femoral condyle cartilage. The final fracture reduction and position of the guide pins were verified by C-arm imaging (Figure 3(b)). Following placement of the guide pins, two 4.5-mm cannulated cancellous lag screws (Depuy Synthes, West Chester, PA, USA) were placed to achieve appropriate compression (Figure 3(c)). During arthroscopy, stable fixation was observed and the length and size of the screws were confirmed to be correct. ACL reconstruction was then performed using a hamstring tendon autograft with preservation of the tibial insertions. An additional anteromedial portal was used for preparation of the femoral tunnel to allow improved access to the anatomical footprint. An Endobutton device (Smith & Nephew, Andover, MA, USA) was used for femoral fixation, and a polyether ether ketone interference screw (BIOSURE SYNC; Smith & Nephew) was used for tibial fixation (Video 1).

(a) Under arthroscopic control, two percutaneous guide pins were inserted to stabilize the medial Hoffa fracture after reduction. (b) After a C-arm scan showed satisfactory reduction and proper position of the guide pins, (c) two 4.5-mm cannulated cancellous lag screws were placed following the guide pins.
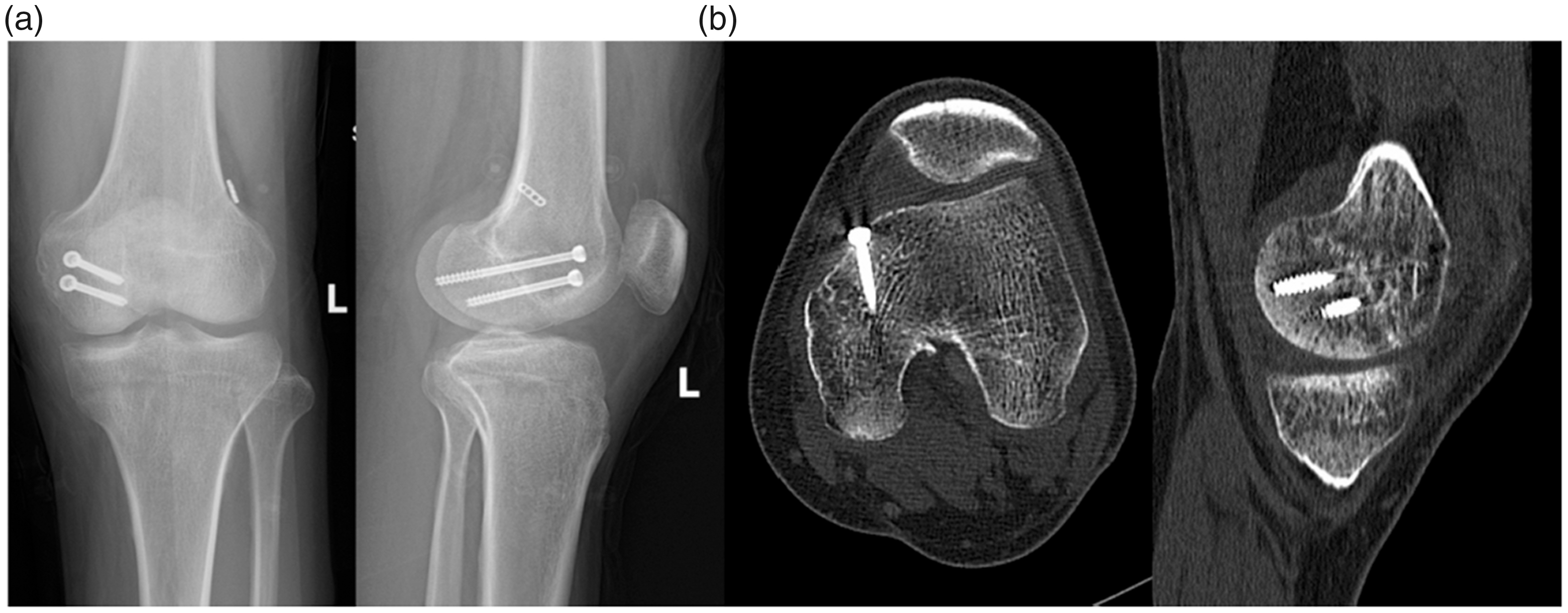
The patient underwent X-ray and CT examinations postoperatively (Figure 4). A long-leg knee brace was used for 3 weeks. Physiotherapy including active and passive knee movement was then performed. Weight-bearing activity was limited for 6 weeks. After successful fracture union was observed radiographically, the patient was allowed to walk without support at 3 months postoperatively with no pain and full range of motion of the knee. At the 1-year follow-up, the patient returned to daily activity and sports with favorable knee function (Figure 5). He developed no short- or long-term complications and was fairly satisfied with his knee status and clinical outcomes. We did not remove the screws; we planned to remove the screws only if the patient developed hardware-related complications during follow-up, such as persistent pain or infection.

Immediate postoperative (a) X-ray and (b) computed tomography images of the left knee.
(a) X-ray and (b) computed tomography images of the left knee at the 1-year follow-up showed successful fracture union.
The procedures performed in this study were approved by the ethics committee of the Third Hospital of Wenzhou Medical University in accordance with the Helsinki declaration. Written informed consent was obtained from the patient.
Discussion
The main finding of the present study is the successful application of a minimally invasive technique in an extremely rare case of a medial Hoffa fracture with concomitant intra-articular ligament injury. The possible mechanism of this rare injury is that when the patient’s knee joint was in a flexed position, the shear stress became concentrated and acted on the posterior half of the medial condyle of the femur, initiating development of the medial Hoffa fracture. The shear stress further increased, the distal femur moved backward, and the tibia moved excessively forward, leading to tearing of the ACL. When such an injury is combined with simultaneous rotation of the knee joint, ligament damage is more likely to occur. Finally, the patient underwent a single-stage fully all-inside arthroscopic procedure and ultimately achieved a favorable clinical outcome. We believe that this case significantly contributes to the literature because the favorable results highlight the beneficial effects of this novel but demanding method in treating medial Hoffa fractures, particularly in patients with associated intra-articular knee injuries.
A Hoffa fracture, first described by Hoffa in 1904, 10 is usually caused by the application of direct anteroposterior force on a flexed knee in high-energy trauma. Although the exact mechanism of this injury remains incompletely understood, a medial Hoffa fracture, as a rare intra-articular injury, is postulated to result from a medial impact on the medial femoral condyle while the affected knee is in a flexed position with an element of adduction and internal rotation. 11 In addition to anterior femoral shear forces, the combined high-energy injury can cause knee valgus and tibial internal rotation, thereby leading to an ACL tear. This could support the association of the medial Hoffa fracture with the ACL tear in our patient.
The diagnosis of a Hoffa fracture is always difficult on plain radiographs because the fracture line is obscured by the intact anterior part of the femoral condyle in the anteroposterior view. If the fragments are minimally displaced, the fracture may be missed even in the lateral view. 12 Nork et al. 13 reported that only 69% of Hoffa fractures are revealed on plain radiographs. CT scans are therefore necessary to detect these occult Hoffa fractures and thereby provide valuable information for surgical planning. Apart from Hoffa fractures, high-energy forces could lead to associated multiple injuries, including cruciate ligament avulsion fracture, 14 cruciate ligament tear, 15 periarticular fractures of the knee, 16 or even multi-ligament injuries. 17 MRI is an accurate and noninvasive diagnostic method to detect concomitant intra-articular injuries of the knee. In the present study, MRI revealed a concurrent ACL tear accompanied by a medial Hoffa fracture.
Because of their intra-articular nature, Hoffa fractures are potentially unstable and often require operative fixation to achieve good clinical outcomes. Various studies have demonstrated that both screw and plate fixation can provide satisfactory functional results.2,18 Nevertheless, Onay et al. 19 performed a retrospective 5-year follow-up of surgical outcomes of isolated Hoffa fractures and observed that medial Hoffa fractures tended to have worse functional results than lateral Hoffa fractures. Arthroscopy has recently been used in the treatment of lateral and medial Hoffa fractures because of its benefits of minimal invasion.20–22 However, no previous reports have described the use of fully arthroscopic techniques in such a rare case as a medial Hoffa fracture with concurrent intra-articular injuries. As demonstrated in the present study, arthroscopic-assisted internal fixation is an ideal technique for a Hoffa fracture with concurrent intra-articular knee injuries. In our case, minimally invasive screw fixation ensured fragment stability, and the use of arthroscopy was beneficial to visualize the reduction of the joint surface, monitor screw insertion, and reconstruct the ACL at the same time. However, the disadvantages of arthroscopic treatment include difficulty of fracture reduction, limited fixation options, and the requirement of experience in arthroscopic treatment. In agreement with a case reported by Say and Kuyubas, 6 our study demonstrated favorable clinical outcomes after use of an arthroscopic-assisted percutaneous screw fixation method to treat a medial Hoffa fracture.
In conclusion, a fully arthroscopic all-inside procedure can facilitate easy access to visualization and reduction of an intra-articular fracture with simultaneous treatment of concurrent knee disorders. This technique can be the optimal method for the treatment of medial Hoffa fractures, particularly for properly selected patients with associated intra-articular knee injuries.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.