
Abstract
Objective
This meta-analysis evaluated the association between the mean platelet volume (MPV) and polycystic ovary syndrome (PCOS).
Methods
A systematic literature search using PubMed, EMBASE, and Web of Science databases until June 2021 was conducted. Pooled standardized mean differences (SMD) and 95% confidence intervals (CI) were determined using a random effects model.
Results
Ten studies involving 866 women with PCOS and 548 age- and body mass index-matched women without PCOS were included. The MPV was significantly increased in women with PCOS compared with non-PCOS women (SMD = 0.43, 95% CI = 0.13–0.72). Subgroup analyses showed that this trend was consistent in cross-sectional studies (SMD = 0.44, 95% CI = 0.03–0.86) and in Turkish women (SMD = 0.46, 95% CI = 0.13–0.79). Meta-regression analysis revealed a marginally positive correlation between the MPV and the homoeostasis model assessment of insulin resistance in women with PCOS. The sensitivity analysis showed that the effect estimate was robust and stable, and publication bias was not evidenced in the pooled analysis.
Conclusions
This meta-analysis revealed that women with PCOS have a significantly increased MPV than women without PCOS, which is probably associated with insulin resistance.
INPLASY registration number: INPLASY2021100021.
Keywords
Introduction
Polycystic ovary syndrome (PCOS) is a common endocrine disorder affecting 5% to 10% of reproductive aged women worldwide. 1 It is characterized by menstrual disorders, oligo-ovulation or anovulation, hyperandrogenism, and polycystic ovaries. 2
Numerous studies have shown that women with PCOS are at an increased risk of developing type 2 diabetes mellitus (T2DM), metabolic syndrome, and cardiovascular disease (CVD).3–5 The mechanistic connection between PCOS and these diseases has been recognized as insulin resistance and chronic low-grade inflammation, which is frequently observed in patients with PCOS.6,7 Inflammation and insulin resistance are capable of triggering vascular endothelial injury and dysfunction, followed by platelet activation,8,9 which was recently shown to be critical to the pathophysiology of T2DM and CVD.9,10
The mean platelet volume (MPV) is an inexpensive and easy parameter to measure that derives from complete blood cell counts determined in daily clinical practice. It indicates platelet size and has long acted as an effective marker of platelet activity. 11 Larger platelets exhibiting a higher MPV are metabolically and enzymatically more active than smaller ones, and produce greater amounts of platelet-activating factors which contribute to the development of CVD. 12 In recent years, several meta-analyses have suggested that an elevated MPV is associated with T2DM, nonalcoholic fatty liver disease, and CVD.13–15 Moreover, studies have investigated whether MPV levels in patients with PCOS influence disease severity. However, findings have been inconsistent. Therefore, to clarify the role of the MPV in PCOS, the present systematic review and meta-analysis were conducted on all eligible studies to evaluate the relationship between the MPV and PCOS based on existing evidence.
Methods
The present systematic review was performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 16 In error, we did not prospectively register this trial, but it has now been registered retrospectively at INPLASY under registration number INPLASY2021100021.
Search strategy
A systematic literature search was performed of electronic databases including PubMed, EMBASE, and Web of Science until June 20, 2021. The search terms consisted of (“Polycystic ovary syndrome” OR PCOS) AND (“mean platelet volume” OR MPV). Reference lists and relevant review articles were manually searched to identify additional eligible studies.
Inclusion and exclusion criteria
Studies were eligible for inclusion if they met the following criteria: (1) including adult subjects (age ≥18 years), (2) comparing the MPV between women with and without PCOS, and (3) no statistically significant differences between cases and controls in terms of mean age and body mass index (BMI). Studies were excluded if they met the following criteria: (1) non-English language studies, (2) interventional studies or samples overlapping with those of another study, or (3) reviews, letters to the editor, case reports, or conference abstracts.
Data extraction and quality assessment
Data were independently extracted from the included studies in a predefined form by two investigators, and then confirmed by a third reviewer. The following information was abstracted from eligible studies: (1) the first author’s name, year of publication, study location, and study design; (2) sample size, mean, and standard deviation of the MPV in PCOS cases and controls; (3) age, BMI, white blood cell (WBC) count, homoeostasis model assessment of insulin resistance (HOMA-IR), and diagnostic criteria for women with PCOS.
The quality of the included studies was assessed by complying with a criterion under the Newcastle–Ottawa Quality Assessment Scale (NOS) for observational studies modified by van Dijk et al. 17 The maximum score was 9, and studies achieving a score of 0 to 3 were considered low quality, while those scoring 7 to 9 were considered high quality.
Statistical analysis
Statistical software STATA version 15 (StataCorp LP, College Station, TX, USA) was used to perform all statistical computations. To quantify individual effect sizes, the standardized mean difference (SMD) and 95% confidence interval (CI) were calculated to estimate the difference in the MPV between PCOS cases and controls. A random effects model was employed to estimate the pooled results because it achieves a more conservative result than a fixed effects model. 18 Heterogeneity of the studies was assessed by performing the chi-square test, with a statistical significance set at P < 0.10. Heterogeneity was quantified by I2 statistics, and I2 > 50% revealed significant heterogeneity. To investigate the sources of heterogeneity, subgroup and meta-regression analyses were conducted. The subgroup analysis explored study location and study design. In the meta-regression analysis, SMD was the dependent variable, and age, BMI, WBC count, and HOMA-IR were predefined as independent variables. Sensitivity analysis was conducted to assess the stability of the results by sequentially removing one study at a time. Publication bias was initially evaluated by visually inspecting funnel plots, then statistically assessed by performing Egger’s test.
A P value of <0.05 was considered statistically significant, unless otherwise noted.
Results
Study selection
An initial publication search from three electronic databases yielded 53 potentially relevant records. After eliminating duplicates, 18 records remained, of which five were excluded by screening the title and abstract. Two of the remaining 13 articles selected for full-text reading were excluded because of a lack of data, and one was excluded for a mismatched BMI between cases and controls. Finally, 10 studies without overlapping patients complied with the inclusion criteria, so were selected for the meta-analysis.19–28 A flowchart illustrating the study selection process is presented in Figure 1.
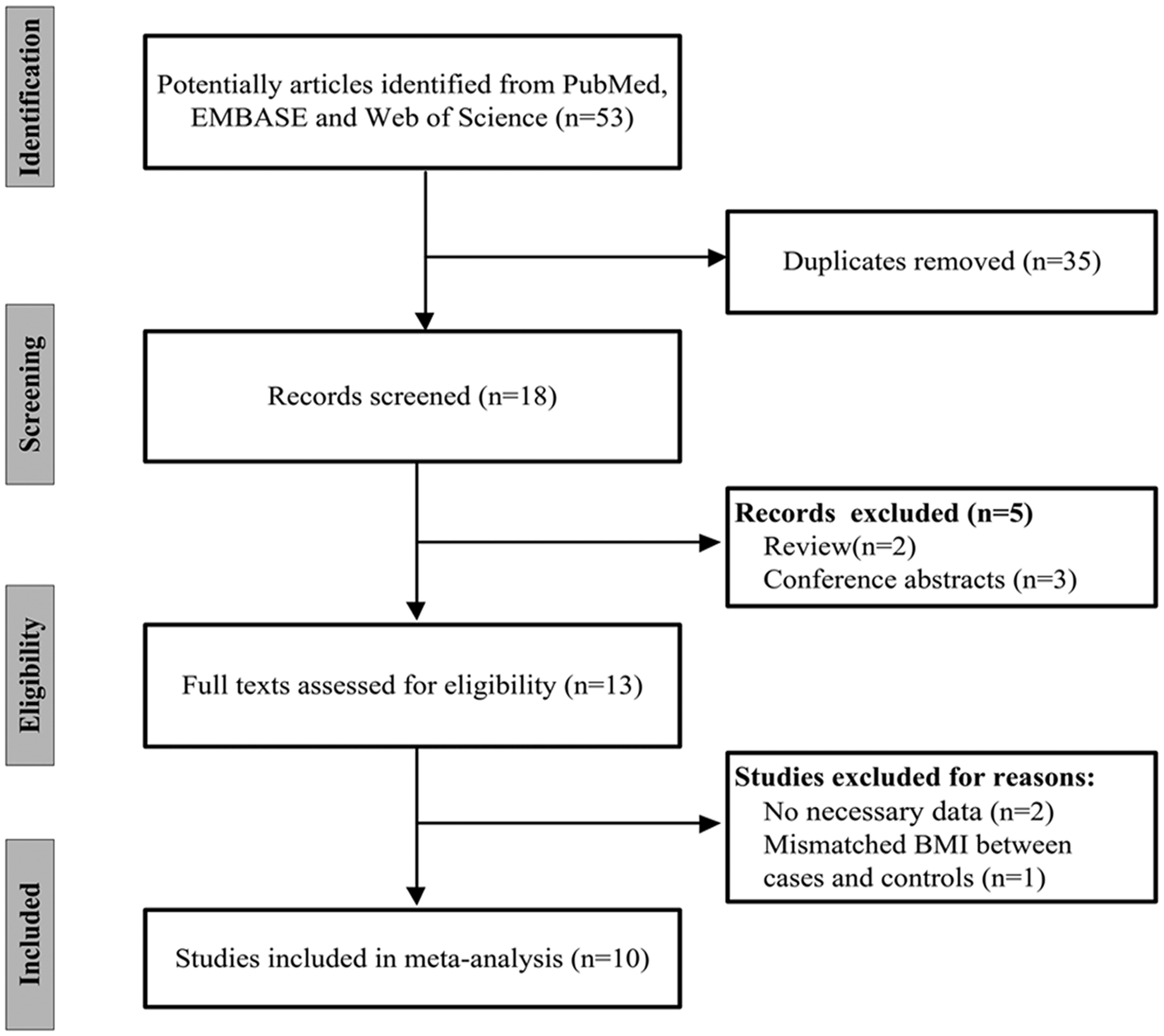
Flow chart of the study selection process.
Characteristics of included studies
The main characteristics of the 10 included studies are listed in Table 1. The studies were published from 2009 to 2020, and included 866 women with PCOS and 548 non-PCOS controls. Healthy women were the control subjects in nine studies, and infertile women were the controls in one study 25 . Seven were cross-sectional studies, and three were case–control studies. Nine studies were conducted in Turkey and one in Saudi Arabia. All studies reported age and BMI, and seven reported the WBC count and HOMA-IR. Additionally, Rotterdam criteria were used for the definition of PCOS in all studies. The number of women with PCOS in each study ranged from 35 to 279, and the number of non-PCOS controls from 24 to 146. The MPV ranged from 7.51 to 10.70 FL in the PCOS group, and from 7.40 to 10.50 FL in the non-PCOS group. Two studies were considered of high quality with NOS scores ≥7, and the remaining eight were regarded as moderate quality. No studies were classified as low quality.
Main characteristics of the studies included in this meta-analysis.

PCOS, polycystic ovary syndrome; MPV, mean platelet volume; BMI, body mass index; WBC, white blood cell; HOMA-IR, homoeostasis model assessment of insulin resistance; NA, not assessed.
Meta-analysis
The MPV was significantly higher in women with PCOS than in age- and BMI-matched women without PCOS (SMD = 0.43, 95% CI = 0.13–0.72, P = 0.005, Figure 2). Significant heterogeneity was identified among studies (I2 = 84.4%; P < 0.001).
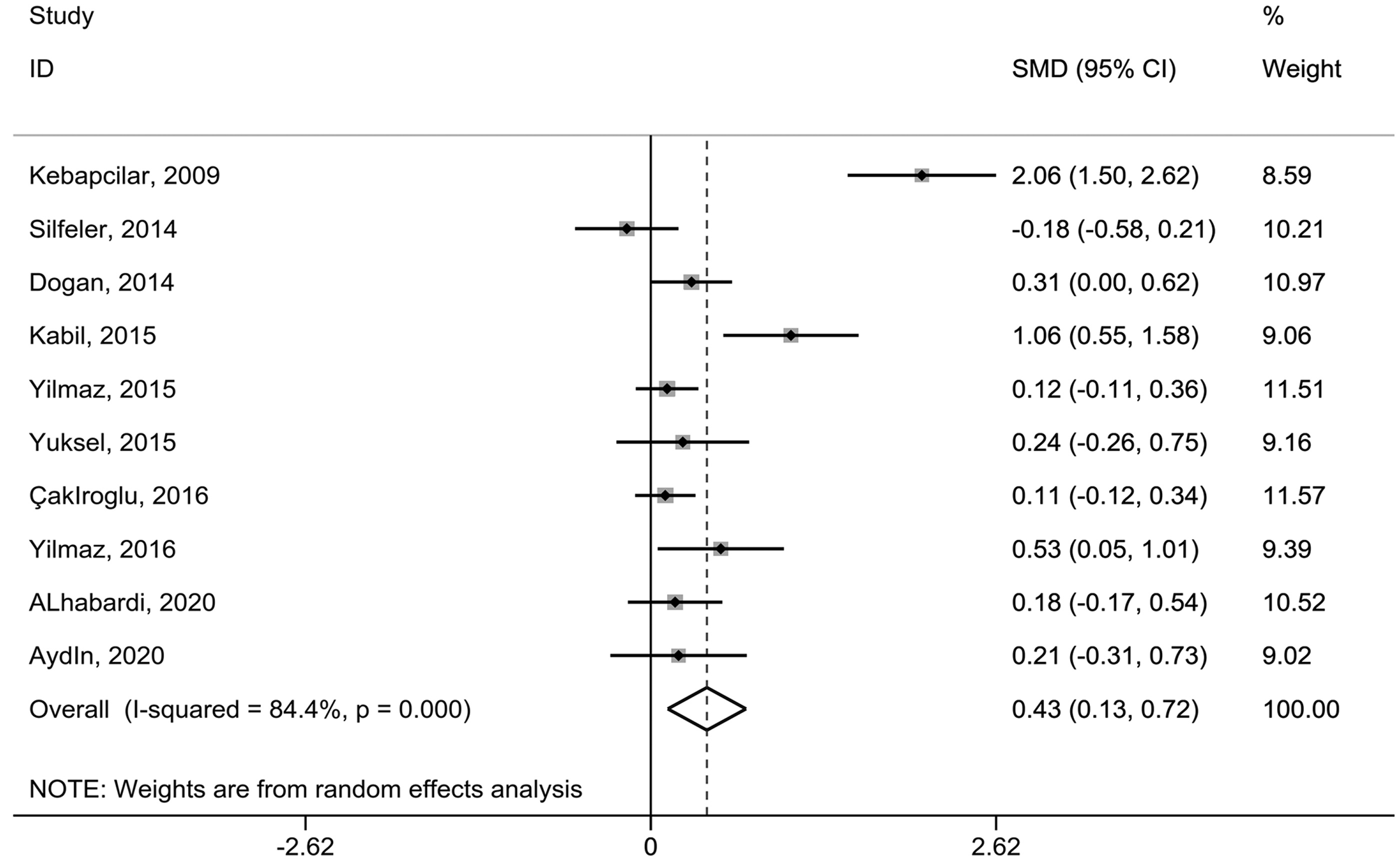
Overall meta-analysis of the MPV in women with PCOS compared with non-PCOS controls.
Subgroup analysis
Subgroup analysis was conducted using study design and study location. As shown in Figure 3a, when the studies were stratified by study design, the subgroup of cross-sectional studies showed a significantly higher MPV (SMD = 0.44, 95% CI = 0.03–0.86, P = 0.038) among women with PCOS, while the difference did not reach statistical significance in case–control studies (SMD = 0.40, 95% CI = ˗0.08–0.89). According to study location, Turkish women with PCOS from nine studies had a significantly higher MPV compared with controls (SMD = 0.46, 95% CI = 0.13–0.79, P = 0.007), whereas in the single study with non-Turkish women, there was no significant difference in the MPV between those with and without PCOS (SMD = 0.18, 95% CI = ˗0.17–0.54) (Figure 3b).
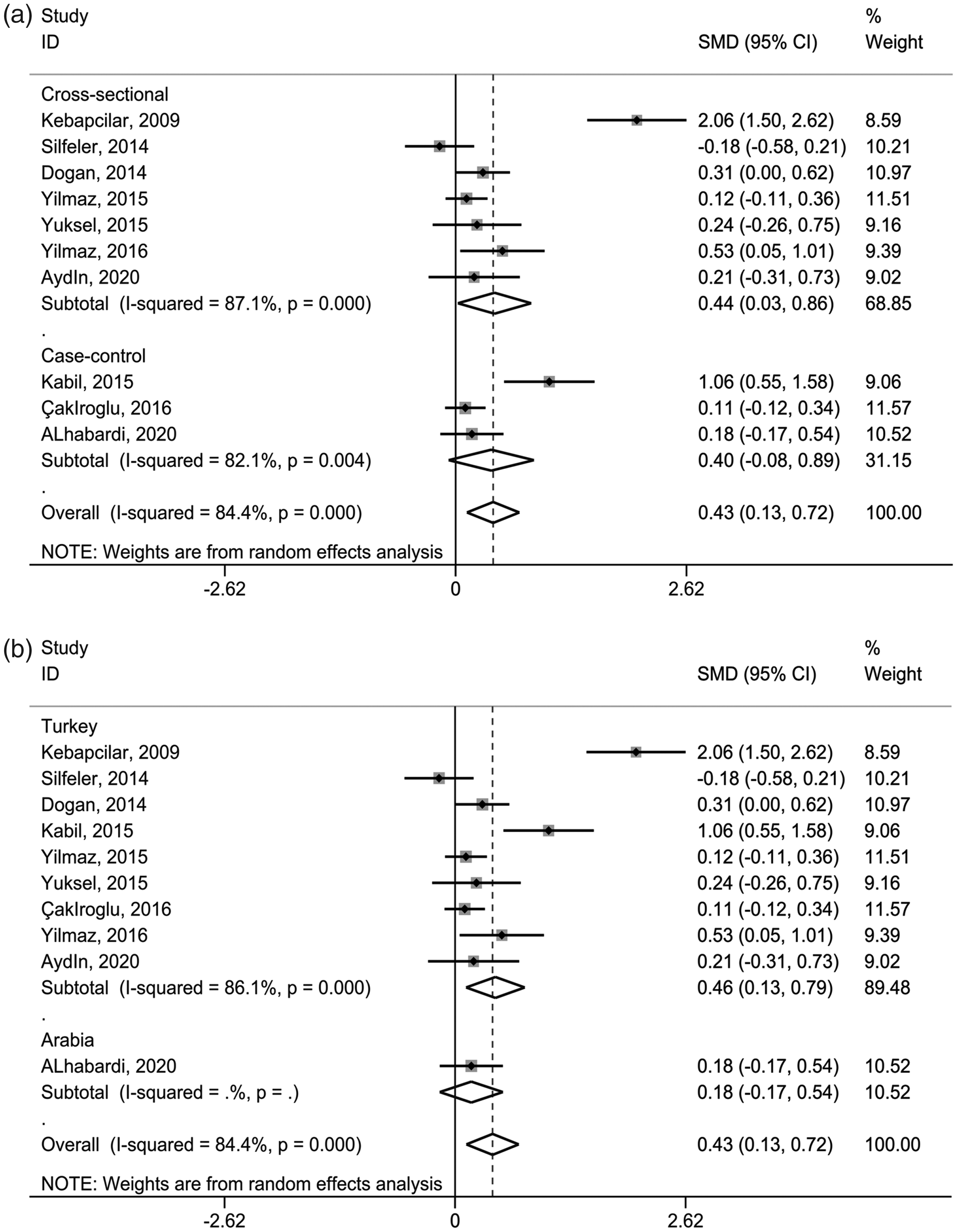
Subgroup analysis of the MPV in women with PCOS compared with non-PCOS controls stratified by study design (a) and study location (b).
Meta-regression analysis
To determine whether continuous variables impacted on the estimated effect size, a random effects meta-regression analysis was conducted on the appropriate studies. A marginally positive correlation was identified between the MPV and HOMA-IR (P = 0.058) (Figure 4d). No significant correlations were observed between the MPV and other variables including age (Figure 4a), BMI (Figure 4b), and the WBC count (Figure 4c).
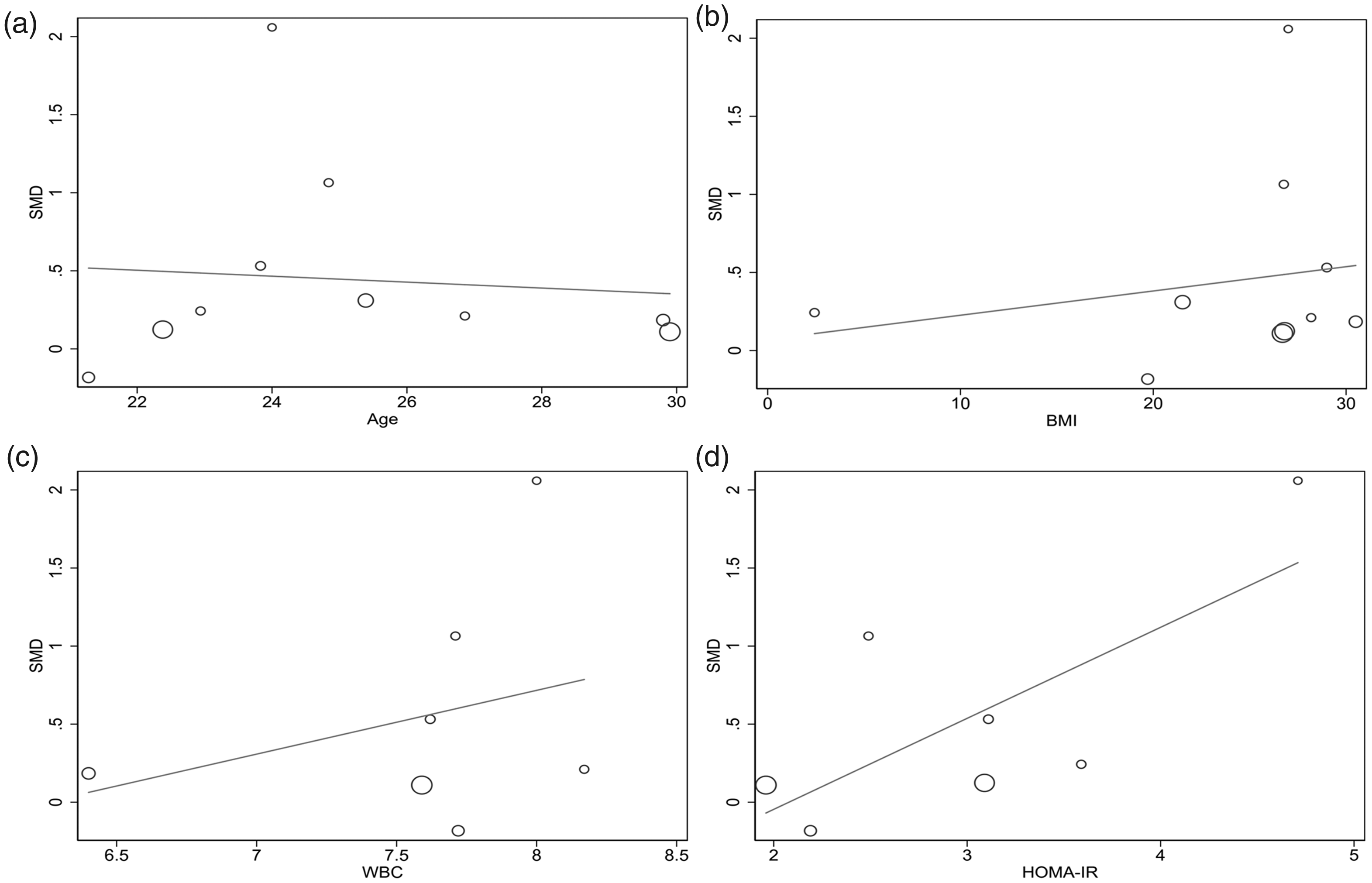
Meta-regression analysis demonstrating relationships between the MPV with age (a), BMI (b), WBC count (c), and HOMA-IR (d).
Sensitivity analysis
No single study excessively impacted on the pooled effect estimate in the comparison between women with PCOS and non-PCOS controls (Figure 5). When excluding the single study 25 in which the controls were infertile women, the pooled SMD was 0.47 (95% CI = 0.12–0.82, P = 0.008).

Sensitivity analysis assessing the influence of each individual study on the pooled effect estimate.
Publication bias
Visual inspection of a funnel plot revealed no obvious asymmetry (Figure 6), and the lack of publication bias was further confirmed by performing an Egger’s test.
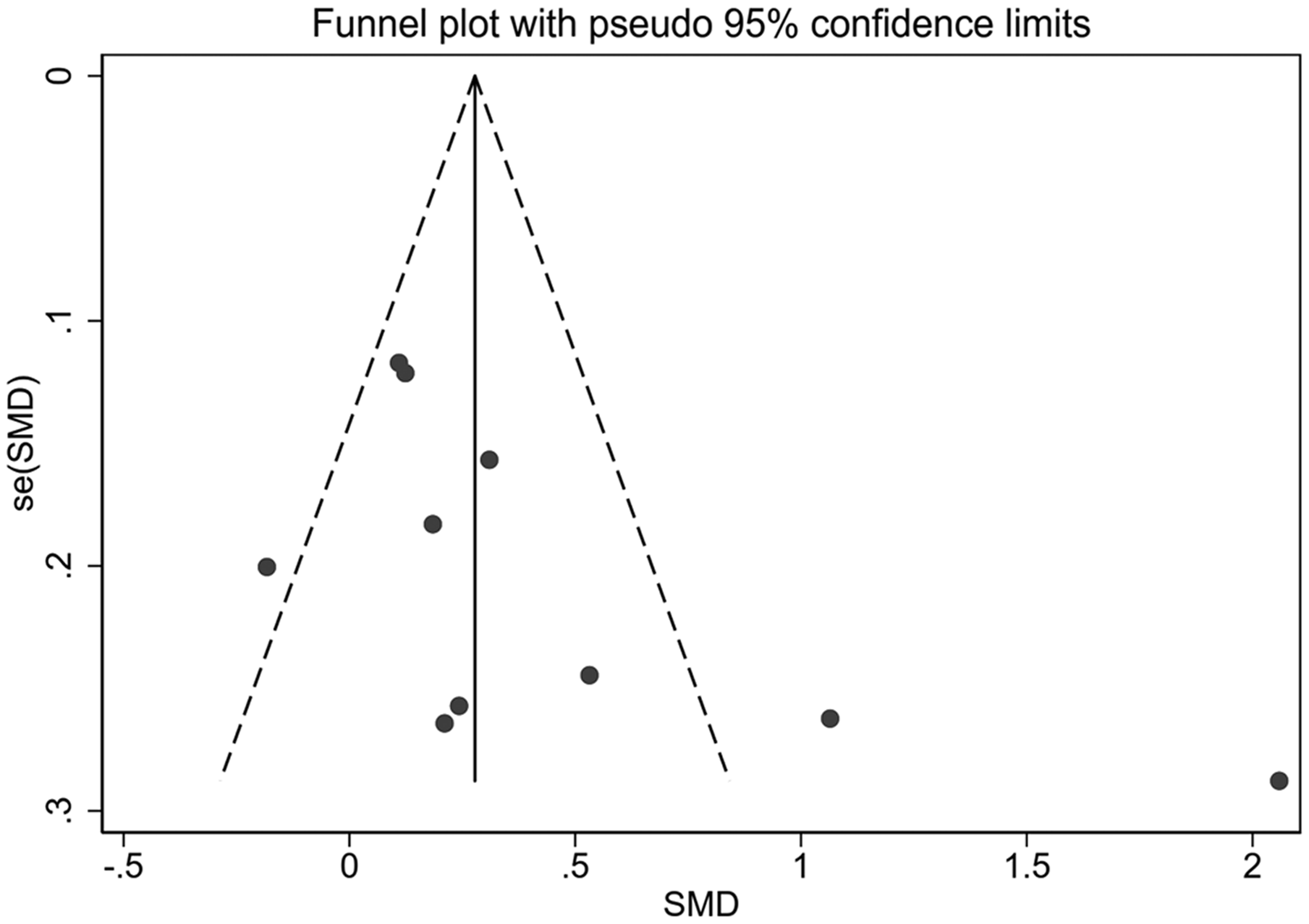
Visual inspection of funnel plots evaluating potential publication bias of the included studies.
Discussion
The present meta-analysis suggests that the MPV is significantly higher in women with PCOS compared with age- and BMI-matched women without PCOS. According to the sensitivity analysis, no single study significantly impacted the effect estimate, and there was no evidence of publication bias. Accordingly, the results of our meta-analysis appear to be stable and robust. To the best of our knowledge, this is the first meta-analysis to evaluate the association between the MPV and PCOS.
The MPV acts as an indicator of platelet activation. Platelets can be activated by multiple forms of stimulation such as chronic persistent inflammation, and, particularly, insulin resistance8,9 which critically impacts the pathogenesis of PCOS. 29 In a large cohort of patients with PCOS, insulin resistance was identified in 59.3% of those of a healthy weight, in 77.5% of those who were overweight, and in 93.9% of obese women. 30 The degree of insulin resistance can, to some extent, reveal the severity of PCOS. 31 Our meta-regression analysis detected a marginally positive correlation between the MPV and HOMA-IR. Moreover, previous studies have suggested that the MPV is significantly positively associated with ovarian volume, which is related to insulin resistance and found to be a hallmark of PCOS development and progression.32,33 Thus, the MPV could be used to reflect insulin resistance and monitor disease progression in women with PCOS.
Although existing research has shown PCOS to be a state of chronic low-grade inflammation, 7 our meta-regression analysis found no significant association between the MPV and WBC count. However, the WBC count is not recognized as an ideal indicator to evaluate low-grade chronic inflammation, and some chronic inflammatory markers such as high sensitivity C-reactive protein (hs-CRP) were only measured in a limited number of studies.23,26 Therefore, our meta-regression analysis cannot be said to have evaluated the association between the MPV and chronic inflammatory markers. Similarly, no significant association was detected between the MPV and BMI. BMI is the most accepted and extensively used index for evaluating obesity, but is far less sensitive than waist circumference or the waist-to-hip ratio (WHR) which are more closely linked to insulin resistance and cardiovascular risk factors.34,35 Moreover, the WHR, rather than the BMI, was found to be associated with testosterone and estradiol levels in young women. 36
There are several limitations to this systematic review and meta-analysis. First, considerable heterogeneity was observed in our pooled analysis. Although subgroup analyses were performed to explore the potential sources of heterogeneity, high levels still persisted. Additionally, given that some subgroups contained few studies, such as the case–control subgroup, our results should be interpreted with caution whether or not they indicated statistical significance. Our meta-regression analysis showed that HOMA-IR may have contributed to the high level of heterogeneity. However, it could not reasonably be explained by any of the other predefined variables including age, BMI, or WBC count. Moreover, because other variables of interest, such as hs-CRP, waist circumference, WHR, follicle-stimulating hormone, luteinizing hormone, testosterone, and estradiol, were only reported in a limited number of our included studies, the meta-analysis could not evaluate whether they contributed to high heterogeneity. Second, all retrieved articles were from English language databases, such that several non-English language articles were excluded; therefore, the pooled effect estimates based on studies that were mostly from Turkey (9 out of 10) might not be applicable to the general population. Similarly, the observed close relationship between the MPV and insulin resistance may not be present in other regions or countries. Moreover, the inclusion of only English language articles may have introduced a selective bias. Third, we did not carry out a power analysis in this meta-analysis; however, a recent study by Jackson al. suggested that five or more studies can achieve reasonable power in a random effects meta-analysis.
In conclusion, the present meta-analysis indicates that women with PCOS have a higher MPV than those without, and this is probably related to insulin resistance. Our findings also suggest that platelet activation may be involved in the development of PCOS. In-depth studies should be conducted to confirm these findings in a larger and more diverse population.
Footnotes
Availability of data
The datasets presented in this study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.