
Abstract
Objective
This study was performed to compare the clinical outcomes of large duodenal lipomas (DLs) of ≥2 cm between endoscopic submucosal dissection (ESD) and endoscopic full-thickness resection (EFTR).
Methods
This retrospective study included patients who underwent endoscopic resection of large DLs from June 2017 to March 2021 at our hospital. Clinicopathologic features, clinical outcomes, and follow-up endoscopy findings were retrospectively reviewed.
Results
Twenty-three patients (12 men) with a mean age of 57.4 years were included. The median tumor size was 28.4 ± 13.3 mm. ESD was performed in 19 patients, and EFTR was performed in 4. Complete resection was achieved in 21 patients. The operative time and postoperative hospital stay were significantly shorter in the ESD than EFTR group. Four patients in the EFTR group developed a fever; no other adverse events occurred. No patients required surgical intervention. During the average follow-up of 21.1 months, no residual tumor, recurrence, or metastasis was observed.
Conclusion
Both ESD and EFTR provide minimally invasive, localized treatment of selected DLs. ESD might have some advantages in resecting large DLs in terms of procedure time and hospitalization.
Keywords
Introduction
A duodenal lipoma (DL) is a rare duodenal mesenchymal tumor accounting for 4% of small intestinal benign tumors and 20% of benign duodenal tumors. 1 Approximately 90% of DLs originate from the submucosa, whereas a smaller number arise from the muscularis propria (MP) layer. Most DLs are benign, but about 1 in 200 is malignant, particularly those larger than 5 cm in diameter. 2 One study showed that 79.6% of patients with DLs were adults aged 40 to 70 years, and 39% of the lipomas grew in the second portion of the duodenum. 3 Most DLs are asymptomatic, presenting as duodenal submucosal tumors (SMTs). However, DLs of >2 cm may cause symptoms. Tarry stool and anemia may occur because of gastric acid erosion and ulceration of the overlying mucosa. DLs of this size may also cause bowel obstruction, intussusception, or abdominal pain. Increasingly more DLs are being incidentally found with the widespread use of screening esophagogastroduodenoscopy. Preoperative differentiation of DLs from other duodenal SMTs is still difficult, and the final diagnosis still relies on pathological examination.
Although most DLs are benign, there is a significant risk of malignancy in those larger than 5 cm in diameter. Surgical resection is the mainstay of treatment of DLs because of the risk of malignancy of large DLs and the challenge in distinguishing benign DLs from liposarcoma; however, surgical resection is associated with considerable morbidity and mortality. 4 In addition, long-term follow-up increases patients’ mental and financial stress caused by repeated endoscopic procedures. Endoscopic resection, including endoscopic submucosal dissection (ESD) and endoscopic full-thickness resection (EFTR), is a minimally destructive treatment that can reportedly be used to remove large DLs.5,6 However, there is no consensus concerning the role of ER, and comparative outcomes between different procedures remain unknown. Therefore, this study was performed to compare clinical outcomes of large DLs treated by ESD versus EFTR.
Methods
Patients
Twenty-three consecutive eligible patients with DLs who underwent ER at our hospital from June 2017 to March 2021 were enrolled in this retrospective cohort study. The inclusion criteria were a DL size of ≥2 cm in diameter and treatment with ESD or EFTR. A flow diagram of patient screening and grouping is shown in Figure 1. All patients underwent endoscopic ultrasonography to evaluate the echogenicity, originating layer, and growth pattern of the tumor. Additionally, abdominal computed tomography (CT) with the administration of intravenous contrast material was performed to determine the tumor characteristics and metastasis before the operation. The tumors were classified into two types depending on the relationship between the tumor location and MP layer. Type A did not connect with the MP and protruded into the lumen; these tumors were treated by ESD. Type B closely attached to the MP and even serosa; these tumors were treated by EFTR. Among the 23 patients, 7 underwent ER because of symptoms and the other 16 underwent ER because of patient desire.
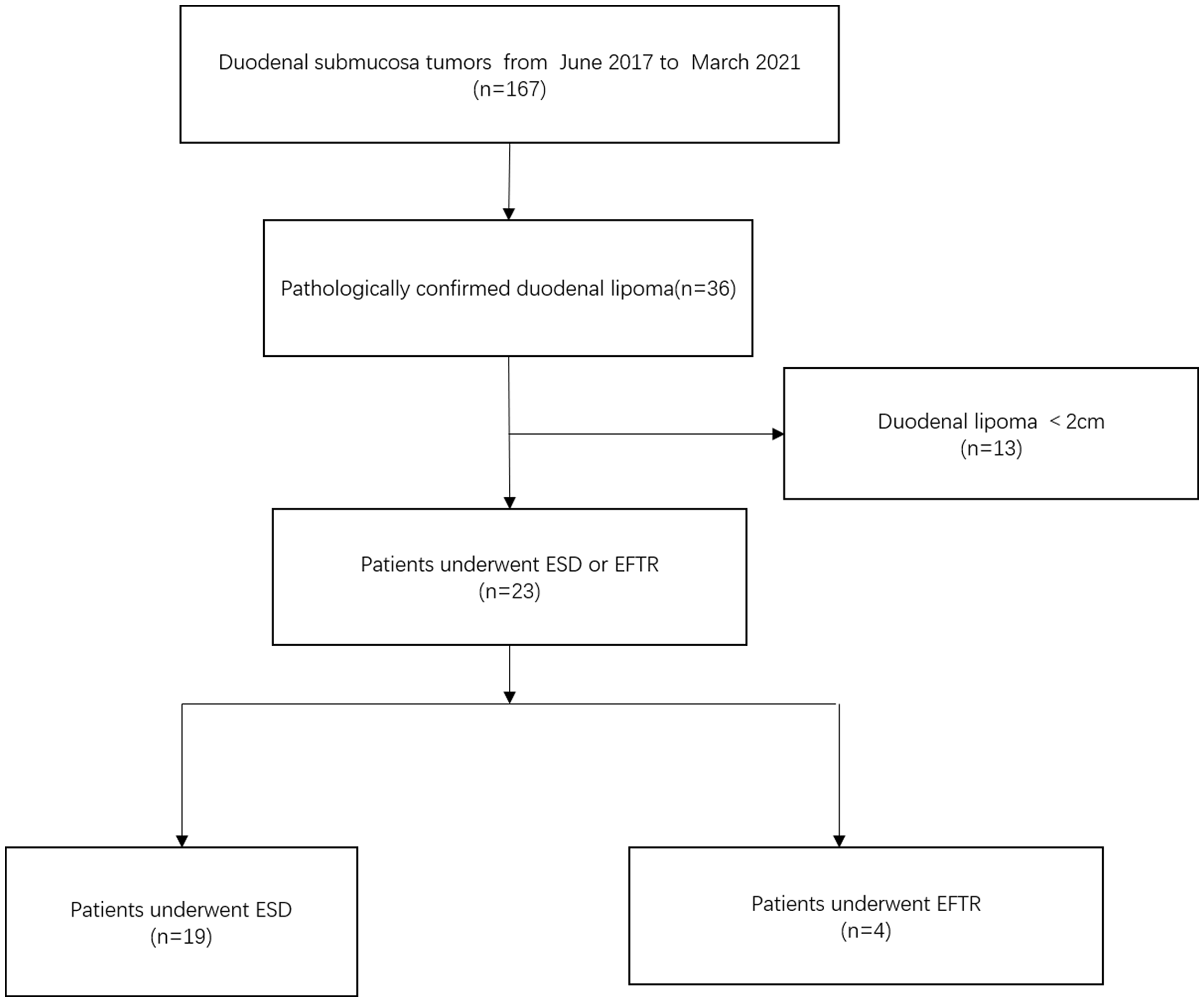
Study flow diagram based on the results of endoscopic resection of duodenal lipoma.
Data were retrospectively collected from a database of clinical report forms and included demographics, tumor characteristics (size, location, and relation to the MP), operational details, complete resection, adverse events, and surveillance endoscopy findings. Complete resection was defined as en bloc resection of the entire gross lesion with negative resection margins. Perioperative perforation was not regarded as a complication in this study. Adverse events were evaluated according to the criteria established by the American Society for Gastrointestinal Endoscopy.
The macroscopic appearances of the polyps were categorized according to the Yamada classification system. 7 Elevated lesions were subclassified into four types using this system: Yamada I, elevations with a smooth baseline without a clear boundary; Yamada II, elevations with a boundary at the base but no notch; Yamada III, elevations with a clearly notched base but no peduncle; and Yamada IV, pedunculated elevations.
Written informed consent was obtained prior to all surgical procedures. The ethics committee of Shanghai Xuhui Center Hospital approved this study (decision date: 13 January 2021; Issue No. 200(2020), IRB). The reporting of this study conforms to the STROBE guidelines. 8
ER procedures
Experienced endoscopists performed all operations. ESD and EFTR were tailored to the tumor’s growth pattern and relation to the MP layer. ESD was indicated for the removal of DLs arising from the submucosal layer with no connection to the MP, whereas EFTR was indicated for tumors closely adhered to the MP and even serosa.
ESD technique
First, a solution composed of saline (2–3 mL), indigo carmine, and epinephrine was injected with a needle into the submucosal layer around the lesion to lift the mucosa. After the mucosa had been incised 5 mm from the edge of the lesion, yellowish tissue was found under the mucosa. The submucosal connective tissue under the lesion was gradually dissected. Injection of the aforementioned solution was periodically repeated by insertion of a needle into the submucosal layer to guarantee persistent mucosal elevation. Finally, the lesion was removed. If pedunculated, the lesion was removed with the assistance of a snare (SD-9u-1; Olympus America, Center Valley, PA, USA); if sessile, the lesion was removed with both the tip of a snare as a flexible diathermic knife and a standard snare (Figure 2).

Endoscopic submucosal dissection of a duodenal lipoma. (a) Endoscopic view of a large duodenal lipoma. (b) Endoscopic ultrasound view, showing the duodenal lipoma without connection with the muscularis propria. (c) A saline solution containing a small amount of indigo carmine dye was injected beneath the lesion to elevate it. (d) The lesion was dissected from the submucosal layer. (e) The lesion was completely removed. (f) The wound was closed with metal clips. (g) The resected specimen. (h) Histologic image of the duodenal lipoma.
EFTR technique
In addition to resecting the submucosal lipoma, the nearby MP and serosa were also removed to achieve complete resection. If a tumor fell into the abdominal cavity, thread-traction was helpful throughout the procedure. A transparent cap was attached to the end of the gastroscope before EFTR. A mixed solution containing 1 mL of indigo carmine was injected into the submucosal layer around the lesion. The mucosa around the lesion was then circumferentially incised, and the lesion was dissected as deep as the MP. The serosal layer was incised around the edge of the lesion. Suction of fluid and air from the duodenum facilitated closure of the duodenal defect, which was performed by application of purse-string sutures using an endoloop and metallic clip (Figure 3). A 20-gauge needle was percutaneously inserted to reduce pneumoperitoneum during and after the procedure. A gastrointestinal decompression tube was placed near the wound to keep the wound clean and detect any postoperative bleeding as early as possible.

Treatment of a duodenal lipoma by endoscopic full-thickness resection. (a) A large lipoma was located in the duodenum. (b) Endoscopic ultrasound view, showing half of the duodenal lipoma closely adhered to the muscularis propria. (c) A saline solution containing a small amount of indigo carmine dye was injected beneath the lesion to elevate it. (d) The lesion was dissected from the deep fibers of the muscularis propria. (e) The tumor was completely resected, creating an artificial perforation. (f) The wound was closed with a nylon band and several clips. (g) The resected specimen. (h) The histologic view, showing large, thick blood vessels within the submucosal adipose tissue.
Follow-up
Patients underwent regular upper gastrointestinal endoscopy to detect local recurrence of DL after ESD. The first follow-up endoscopy was performed 3 months after ESD to confirm mucosal healing, with annual endoscopic surveillance afterward. CT or magnetic resonance imaging (MRI) of the upper abdomen could be an alternative for follow-up surveillance if endoscopy was not affordable and accessible. Follow-up was achieved using a telephone directly or at an outpatient clinic of endoscopy center.
Statistical analysis
Statistical analysis was conducted with IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY, USA). Continuous variables are shown as mean ± standard deviation or median with range. Categorical variables are presented as frequency and proportion. Continuous variables were assessed by Student’s test or the Mann–Whitney U test as appropriate. Categorical variables are displayed as proportions and were analyzed with Pearson’s chi-square test or Fisher’s exact test as appropriate.
Results
The patients’ baseline characteristics and the treatment outcomes of ESD and EFTR are shown in Table 1. Of the 23 patients, 12 (52.2%) were men. The mean age of all patients was 57.4 years (range, 28–73 years). Most patients were asymptomatic (n = 16), whereas symptomatic patients presented with epigastric pain (n = 5) and melena (n = 2). One patient (Patient 12) underwent simultaneous ER of four DLs, the largest of which was 40 mm in diameter and removed by ESD and the others of which were <20 mm in diameter and removed by EMR.
Summary of clinicopathologic features and treatment outcomes in 23 patients with duodenal lipomas who underwent ESD or EFTR.
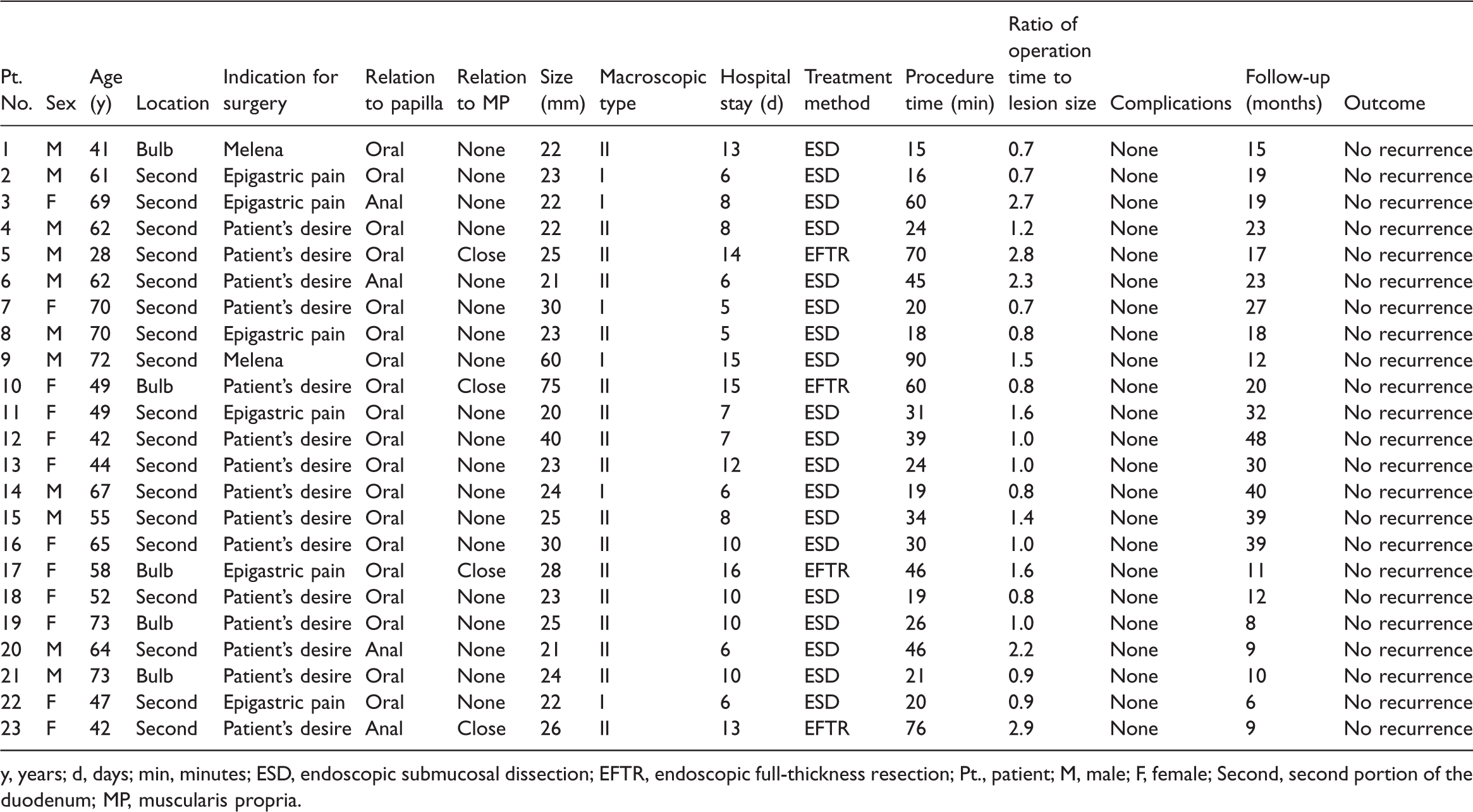
y, years; d, days; min, minutes; ESD, endoscopic submucosal dissection; EFTR, endoscopic full-thickness resection; Pt., patient; M, male; F, female; Second, second portion of the duodenum; MP, muscularis propria.
Most of the tumors were located in the second portion of the duodenum (n = 18); only five (21.7%) were located in the bulb. Yamada II (73.9%) was a more common architecture than Yamada I (26.1%). The mean tumor size was 28.4 ± 13.3 mm. Patients in the EFTR group had significantly larger tumors than patients in the ESD group (P < 0.05). All patients underwent mini-probe endoscopic ultrasonography, which showed that 19 (82.6%) tumors grew with no adhesion to the MP and that 4 tumors were closely adhered to the MP. All tumors were hyperechoic, originating from the submucosal layer. Complete resection was achieved in 21 (91.3%) patients. One incomplete resection occurred during ESD when the tumor was adjacent to the papilla and a snare was used for piecemeal resection (Patient 9). In the other case (Patient 10), the tumor was resected en bloc but was too large (75 mm) to pass through the esophagus. We divided the tumor into two pieces in the stomach to achieve successful peroral retrieval. The en bloc resection rate of ESD was 94.7% (18/19), and the en bloc resection rate of EFTR was 100% (4/4). Treatment outcomes are shown in Table 2. Among the four patients who underwent EFTR, the duodenal wall defects were closed with multiple clips and an endoloop. The procedure time of ESD (median, 24 minutes; range, 15–90 minutes) was significantly shorter than that of EFTR (median, 65 minutes; range, 46–76 minutes) (P < 0.05). The ratio of the procedure time to the lesion size was smaller for ESD (median, 1.0; range, 0.7–2.7) than for EFTR (median, 2.2; range, 0.8–2.9), but the difference was not statistically significant. Moreover, the ESD group had a significantly shorter operative time than the EFTR group (P < 0.05). The postoperative stay after ESD (median, 8.0 days; range, 5–15 days) was significantly shorter than that after EFTR (median, 14.5 days; range, 13–16 days), (P < 0.01). No patients developed adverse events such as delayed bleeding or perforation; only four patients in the EFTR group developed a fever on the first postoperative day (highest temperature of 38.8°C–39.2°C). All patients’ fever resolved the next day with conservative therapy. No patients required a surgical intervention. The follow-up time after EFTR (median, 14 months; range, 9–20 months) was significantly shorter than that after ESD (median, 19 months; range, 11–48 months) (P = 0.2). During the long-term surveillance (average of 21.1 months), no residual tumor or local recurrence was identified in any patient.
Treatment outcomes after endoscopic resection of duodenal lipomas according to each treatment method.

Data are presented as median (range) or number of patients.
ESD, endoscopic submucosal dissection; EFTR, endoscopic full-thickness resection.
Discussion
A DL is a rare type of duodenal SMT that originates from fat tissue in the submucosal layer of the duodenal wall. The incidence rate of DLs is low but has been increasing with the growing popularity of screening esophagogastroduodenoscopy. DLs are more likely to occur from 50 to 70 years of age and show no sex predominance. In the present study, the male:female ratio was similar and the patients’ mean age was 57.4 years. DLs have traditionally been managed surgically, including segmental intestinal resection and Whipple’s pancreatectomy; however, surgical procedures are associated with high morbidity and mortality.9,10 Moreover, because of its technical difficulties and high risk of perforation and bleeding, ER for DLs was previously regarded as controversial. Therefore, endoscopists were reluctant to perform endoscopic removal of duodenal tumors. As surgeons’ experience in removing duodenal tumors subsequently grew and as endoscopic tools and devices underwent further development, ER was proven acceptable for the management of large DLs with a satisfactory overall prognosis.11,12
ER has been regarded as an ideal replacement for surgical treatment of duodenal SMTs and has been performed as a diagnostic and therapeutic method. 13 Several reports concerning the efficacy and safety of ER for DLs have been published.14–16 SMTs with Yamada I or Yamada II architecture are difficult to resect by EMR; instead, ESD is more appropriate for these tumors. 12 In addition, partial resection of the tumor will cause a psychological burden and result in repetitive endoscopic treatment. In the present study, the complete resection rate was 91.3%. Two patients underwent piecemeal resection because of their large tumor size (50 mm). After a mean follow-up of 21.1 months, no residual tumor, recurrence, or metastasis was identified. We performed ESD for 19 lesions and EFTR for 4 lesions. The procedure time of ESD was significantly shorter than that of EFTR, which is used to treat much larger lesions and involves closure of a duodenal wall defect. Additionally, we noted that most operations (n = 20) could be completed in ≤1 hour with en bloc resection. We consider that 90% of submucosal lipomas are well-demarcated. The pseudocapsule of the lipoma helps doctors to identify the edge of the swelling and free the base from the deep tissue. Because of the clear delineation between the subcutaneous tissue and the pseudocapsule, fewer difficulties might be encountered than when resecting other SMTs. One ESD procedure took 90 minutes because the tumor was large (60 mm) and rooted in the ampullary papilla. After removal of the DL, endoscopic drainage of bile juice was performed to prevent blockage of the common bile duct. However, according to several studies of duodenal SMTs, ESD for DLs has several advantages over surgery, including an intact duodenal lumen after surgery, less intraoperative blood loss, a shorter operating time, a shorter postoperative hospital stay, and lower cost. Further large-scale studies are required to definitively demonstrate these advantages.
Delayed adverse events (bleeding or perforation) are major concerns in patients undergoing duodenal ER because of the particular anatomy involved in this procedure. 17 ER-induced ulcers are exposed to acids and pancreatic juices in the lumen. The thin luminal wall and extensive second-order blood supply of the duodenum increase the risk of adverse events. In addition, ER-induced ulcers on the anal side of the ampullary papilla are exposed to bile and pancreatic juice and are more likely to result in adverse events. A multicenter survey of 1397 patients who underwent ER in Japan showed that postoperative hemorrhage occurred in 3.6% of patients. 18 In the present study, no patient developed delayed bleeding or perforation because all ulcers were managed with hemostatic forceps, particularly at the root of the tumor. All ulcers were completely closed with endoscopic clipping. In addition, most lesions (n = 19) were on the oral side of the papilla of Vater. Inoue et al. 19 reported that the rate of delayed perforation of duodenal ESD on the anal side of the major papilla was higher than that on the oral side of the major papilla (21% vs. 0%, respectively). We noted that coagulation forceps should be used carefully because careless transmural burns may increase the risk of perforation. When coagulating forceps are used, the muscle layer should be pulled away before coagulation.
Closing duodenal luminal defects is a technical challenge. After gas leakage from the duodenum to the retroperitoneal cavity, the duodenal lumen becomes smaller. In addition, the working channel of the endoscope in the 6-o’clock position makes it quite challenging to place a clip in the anterior or medial wall. Tsutsumi et al. 20 reported that mucosal suturing and coverage of duodenal mucosal wall defects significantly reduced the risk of delayed adverse events by more than 80%. In our study, all defects were closed with clips and endoloops. Endoclips are still commonly used for endoscopic closure of defects of <1 cm in size. 21 A nylon loop and metallic clips are also applied to close large gastrointestinal wall defects through a two-channel gastroscope. 16 Zhu et al. 22 reported 23 cases of complete closure of wall defects with purse-string sutures using novel endoloops and repositionable hemostasis clips through a single channel. A 3-cm duodenal wall defect was successfully closed, and no patients developed peritonitis or duodenal stricture. Standardized endoscopic procedures for closing duodenal wall defects have not been established, and selection of the procedure is mainly determined by the defect size, location, available devices, and endoscopists’ preference. This highlights the need for performing closure of duodenal wall defects in a longitudinal direction to ensure that duodenal stricture does not occur. 23
The strategy of follow-up endoscopy for DLs remains undetermined. No local recurrence of DLs was encountered during follow-up in the present study. We do not recommend frequent surveillance CT and endoscopy because of the rarity of recurrence of benign DLs. Considering its good prognosis and long-term endoscopic outcomes, we consider that one endoscopic examination is imperative for observing wound healing within 3 to 6 months after the operation.
To the best of our knowledge, this study involved one of the largest groups of patients with DLs treated with ER to date. Our results suggest that the clinical outcomes of ESD for large DLs are impressive and that no adverse events occur.
This study had some limitations. First, selection bias was undoubtedly present because this was a single-center study with a small sample size. Second, recall bias may have occurred because of the retrospective nature of the study. Third, the follow-up was not long enough to make definitive conclusions about recurrence when considering the indolent nature of lipomas.
In conclusion, ESD and EFTR are minimally invasive techniques that may benefit selected patients with DLs. They offer localized treatment of these tumors with few complications and low mortality. However, ESD might be superior to EFTR for DLs in terms of shortening the operating time and length of hospital stay.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211066397 - Supplemental material for Minimally invasive management of large duodenal lipoma: endoscopic submucosal dissection
Supplemental material, sj-pdf-1-imr-10.1177_03000605211066397 for Minimally invasive management of large duodenal lipoma: endoscopic submucosal dissection by Bin Yang, Fei Jiang, Pinxiang Lu and Huazhong Han in Journal of International Medical Research
Footnotes
Authors’ contributions
BY and HZH substantially contributed to the design of the study. BY and FJ collected, analyzed, and interpreted the data. BY drafted the manuscript. BY, FJ, and HZH critically revised the manuscript for important intellectual content. PXL performed all operations. All authors gave final approval of the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Financial disclosure
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This study was supported by Shanghai Committee of Science and Technology [No. 19511121303]
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.