
Abstract
Objectives
We aimed to identify the risk factors for coronavirus disease 2019 (COVID-19)-associated hospitalization to provide evidence for improved clinical care of patients with COVID-19 infection.
Methods
We conducted a cross-sectional study among 300 participants. The collected data comprised sociodemographic data, lifestyle habits, physical activity, medical history, anthropometric measurements, COVID-19-related symptoms, dietary habits prior to and after COVID-19 infection, and psychological status.
Results
Fifty-nine participants were hospitalized. Fever, dry cough, joint pain, chills, diarrhea, and shortness of breath were significantly associated with hospitalization owing to COVID-19. Adults with obesity, diabetes mellitus, hypertension, respiratory diseases, and cardiovascular diseases had higher rates of hospitalization. The findings also showed that residential area and age were related to COVID-19 hospitalization. Furthermore, our analysis revealed that certain dietary habits were associated with hospitalization rates.
Conclusion
Our study confirmed that older age, urban residence, illiteracy, obesity, hypertension, diabetes mellitus, respiratory diseases, cardiovascular diseases, and symptoms of loss of smell and sneezing elevated the risk of hospitalization among patients with COVID-19 infection. Patients with a higher risk of hospitalization may benefit from targeted therapeutic and preventive interventions.
Introduction
The first case of coronavirus disease 2019 (COVID-19) was reported in Wuhan, China in December 2019. This disease is caused by a virus belonging to the coronavirus family called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which spread globally over a short period. 1 In March 2020, the World Health Organization (WHO) categorized COVID-19 as a global pandemic. 2
As of 22 May 2021, there have been 166,513,727 confirmed cases of COVID-19 infection and 3,458,945 COVID-19-related deaths worldwide. 3 In Palestine, the first case of COVID-19 infection was confirmed on 5 March 2020 after a group of Greek tourists who visited a hotel in late February tested positive for SARS-CoV-2. As of 22 May 2021, there have been 333,810 COVID-19 cases and 3720 COVID-19-related deaths in the country. 4
The early symptoms of COVID-19 infection include dry cough, fatigue, shortness of breath, and fever. 5 Severe complications including cardiomyopathy, acute respiratory injury, severe pneumonia, septic shock, and acute respiratory distress syndrome have been reported in 33% of infected patients. 6 Earlier studies indicate that older people, especially those with health problems, have a greater probability of developing serious symptoms of this viral infection7,8
During the 2009 pandemic of influenza A virus H1N1, a strong relationship between influenza infection and obesity was noted. During that period, it was observed that obese individuals had a high risk of severe disease, high rates of mortality, and increased hospitalization. 9 Similarly, a link has been observed between body weight status and the severity of COVID-19 symptoms. 10 Overweight and obesity are considered a public health issue worldwide, and these factors increase the risk of severe COVID-19 infection. 11 This situation increases the burden on health care systems, with increased likelihood of collapse. 12 A sedentary lifestyle has also been indirectly 13 and directly linked with weak immunity via a circular relationship between obesity and inactivity. 14
Researchers have reported that older patients have a greater risk of experiencing severe symptoms of COVID-19 infection. 15 Early studies have pointed out that certain chronic diseases, such as pulmonary and cardiovascular diseases as well as hypertension, can increase disease severity among individuals affected with COVID-19, thereby leading to an increase in the rates of hospitalization and mortality.5,8 Nonetheless, several risk factors associated with the severity of this disease remain ambiguous. 16
Unhealthy dietary patterns (e.g., excessive consumption of empty-calorie foods; foods high in cholesterol, trans-fatty acids, saturated fatty acids, and salt; and low consumption of fruits and vegetables) are considered the primary contributor to the high prevalence of chronic disease and obesity. 17 Indeed, past reports indicate that certain dietary habits may influence inflammatory markers related to low-grade systematic inflammation. 18 As a rule, low-grade inflammation is linked to interleukin (IL)-10 and IL-17 ratios; IL-17 has a fundamental role in host defense against inflammation and infection via generation of antimicrobial peptides and absorbing neutrophils. 19
Certain risk factors have a potential influence on the likelihood of being hospitalized owing to COVID-19 infection. Therefore, in the current study, we aimed to explore the relationship of demographic characteristics, lifestyle factors, clinical factors, comorbidities, and dietary habits with COVID-19 hospitalization. Our study findings will assist in identifying appropriate clinical care and treatment to improve the health status of patients with COVID-19 infection.
Methods
Study design, setting, and population
This cross-sectional study was performed among a representative sample of recovered patients with COVID-19 infection in Hebron city, Palestine.
Sample determination
Participants were recruited using voluntary non-random sampling
The inclusion criteria were participants over 18 years old who had recovered from COVID-19 infection and were willing to participate and to provide all the required data. The exclusion criteria were individuals who did not consent to participate in the study and those who had missing primary data. Participants were recruited via announcements published on social networks (e.g., Facebook, Instagram, Twitter).
Ethical considerations
The research protocols were in accordance with the Declaration of Helsinki and reported in line with the STROBE checklist for reporting cross-sectional studies. The study protocol was approved by the Deanship of Scientific Research Ethical Committee at Palestine Polytechnic University (approval number KA/41/2019). Permissions and approval to conduct the study were obtained from the Palestinian Ministry of Health. Informed written and verbal consent was collected from all participants prior to data collection.
Data collection and research instruments
An interview based on a pre-tested questionnaire was administered to the included participants. Data collection began in August 2020 and ended in December 2020 and was conducted by a group of four nutritionists. Participants were briefed on the objective of the study; then, the questionnaires were administered upon receiving verbal consent from each patient. The collected data included sociodemographic data, lifestyle habits, medical history, anthropometric measurements, psychological status, COVID-19 symptoms, and habits prior to and after COVID-19 infection.
Demographics and lifestyle habits
Questions addressed demographic data, including age, sex, marital status, residential area, living arrangements, and income. Data regarding lifestyle habits (e.g., smoking, physical activity) were elicited from the patients.
Medical history
Medical history included self-reported presence of disease (e.g., diabetes mellitus, hypertension, respiratory diseases, cardiovascular diseases, kidney diseases, gastrointestinal diseases, liver diseases diabetes) and self-reported blood type (A+, A−, B+, B−, O+, O−, AB+, AB−).
Anthropometric measurements
Anthropometric indices including weight and height were used to assess the nutritional status of participants. Height and body weight were measured according to the standard anthropometric procedures described by Lee and Nieman. 21 Body mass index was calculated as body weight in kilograms divided by height in meters squared (kg/m2), and was classified according to WHO cutoffs. 22
Psychological status
In this part of the questionnaire, participants were asked three questions to assess their psychological status owing to the COVID-19 pandemic (e.g., need for psychological counseling, feelings of anxiety and fear, and behaviors when suspecting infection with COVID-19).
COVID-19 symptoms
Participants were asked about the presence of COVID-19-related symptoms (fever, dry cough, sneezing, headache, joint pain, chills, diarrhea, shortness of breath, loss of smell, loss of taste, runny nose), the duration of symptoms, and duration of infection.
Dietary habits prior to and during COVID-19 infection
This section focused on eliciting data regarding participants’ dietary habits (e.g., vitamin deficiency, number of meals per day, number of snacks per day and type, number of servings of fruits and vegetables/carbohydrates/dairy products/meats consumed daily, the type and frequency of meats consumed weekly, consumption of sweetened beverages, type of bread consumed, and increased consumption of foods that boost immunity) and participants’ physical activity (e.g., duration of physical activity) prior to COVID-19 infection.
The following two items were also included in this section of the questionnaire: (1) participants’ use of dietary supplements, (2) participants' need for hospitalization owing to COVID-19 infection.
Statistical analysis
We used IBM SPSS, version 21 to analyze the collected data (IBM Corp., Armonk, NY, USA). A 5% alpha level and 80% power were considered in all of the statistical tests. The results of descriptive analysis are reported as mean and standard deviation for continuous data, and categorical data are described using number and percentage. To determine the risk factors for hospitalization, we conducted univariate analysis using Fisher’s exact test. Further analysis was done using hierarchical binary logistic regression to determine the risk factors for hospitalization in a multivariate model. We checked logistic assumptions, multicollinearity, and outliers. To determine how well the model fit the data, we used the Hosmer–Lemeshow goodness-of-fit test.
Results
Participant characteristics
Figure 1 shows the steps followed in participant enrollment. Among the total of 312 participants, only 300 were included in the final analysis: 165 (55.0%) women and 135 (45.0%) men. The remaining participants were excluded, mainly owing to missing data.

Participant recruitment.
Table 1 shows the sociodemographic characteristics of our study population. Participants were 45.0% men and 55.0% women. The mean age of participants was 30.5 ± 12.2 years, ranging from 18 to 77 years. The analysis revealed that half of enrolled participants (50.7%) were unmarried. Only 12.3% of participants did not complete high school. Approximately half of the study population (58%) was living in either a camp or village and was not working (44.7%). Most participants (92.0%) were living with their family (e.g., spouse/siblings/parents) and 65.3% had a monthly income of 1500 to 5000 Israeli new shekels.
Participants’ sociodemographic characteristics according to sex.

NIS, Israeli new shekel.
Participant lifestyles
The findings showed that most participants (70.3%) were non-smokers. Moreover, 42.7% (n = 128) of participants reported engaging in physical activity, with a mean duration of 45 ± 22.1 minutes per week (data not shown).
Nutritional status
Figure 2 shows that slightly more than half of participants had a normal weight (53.7%) and only 3.4% were classified as underweight.

Weight categories of participants based on body mass index, according to sex.
Medical history
Hypertension was prevalent among our participants (12.1%) whereas liver and kidney diseases were the least common (1.3%). In our sample, the rarest blood type was B− (4.4%) whereas the most common was A− (33.7%).
Patients’ psychological status
Most participants did not need psychological counseling (65.7%); however, more than half (55.3%) reported having feelings of fear and anxiety during the COVID-19 pandemic. Nearly half of participants (45.0%) reported that they sought out a health care professional if they suspected COVID-19 infection. Our analysis also revealed that fear and anxiety during the pandemic was significantly more prevalent among women than men (p < 0.05).
Prevalence of hospitalization
Our analysis revealed that most participants (80.3%) were not hospitalized owing to COVID-19 infection; only 59 participants (19.7%) reported being hospitalized.
COVID-19 symptoms
Overall, the most frequently reported COVID-19 symptoms were fever, headache, and joint pain, with 72%, 70.3%, and 69.7%, respectively. The least frequently reported symptoms among our participants were runny nose and sneezing, with 31.0%, and 35.0%, respectively. The mean duration of losing the sense of smell or taste was 31.4 ± 39.9 days. Half of participants (50.7%) reported that COVID-19 symptoms lasted for 2 weeks and only 24 participants reported having COVID-19 symptoms for more than a month. Furthermore, over half of participants (59.7%) made a full recovery within 2 weeks; a small proportion of participants (5.7%) needed more than 1 month before making a full recovery.
Dietary habits before COVID-19 infection
Table 2 shows participants’ lifestyle and dietary habits prior to COVID-19 infection. Nearly half of participants (45.0%) consumed three meals per day, and 40.7% reported consuming one snack per day. Most participants reported consuming fruits and vegetables (72.0%) and meat products (93.0%) and fewer consumed dairy products (60.7%) and white bread (62.3%). All types of meat including poultry, fish, red meat, and processed meat were consumed with a mean frequency of 2.8 ± 1.0 times/week by 62.8% of participants. Furthermore, the analysis revealed that participants consumed a mean 2.2 ± 1.0 servings/day of fruits and vegetables, 5.0 ± 1.6 servings/day of meat, and 1.6 ± 0.5 servings/day of dairy products. Approximately half of participants reported that they did not consume either sweetened beverages (54.3%) or canned foods (55.7%).
Dietary habits prior to COVID-19 infection.

Dietary habits during COVID-19 infection
Table 3 shows the dietary habits followed by participants during COVID-19 infection. More than half of participants reported that they did not take dietary supplements (62.3%) and did not change their dietary habits (61.7%) during the period of infection. Our analysis revealed that nearly half of participants consumed three meals per day (44.7%) had two snacks per day (46.3%). Furthermore, 38.0% of participants engaged in physical activity with a mean duration of 44.5 ± 29.4 minutes/day. Most participants consumed fruits and vegetables (65.7%) and meat products (92.7%); 67.3% consumed dairy products and 61.7% reported consuming white bread. Approximately 39.9% of participants reported consuming red and processed meat, with a mean frequency of 2.8 ± 1.0 times/week. Our analysis revealed that participants consumed a mean 3.0 ± 1.4 servings/day of fruits and vegetables, 1.8 ± 0.8 servings/day of meat, and 1.8 ± 0.6 servings/day of dairy products. Most participants reported that they did not consume either sweetened beverages (80.3%) or canned foods (87.3%). Unsurprisingly, approximately three-quarters of respondents (73.0%) reported consuming immunity boosting foods.
Dietary habits during COVID-19 infection.

Hospitalization and participants’ sociodemographic characteristics
The results of univariate and multivariate analyses for sociodemographic variables showed that area of residence and age were related to hospitalization (Table 4). Hospitalization was significantly more common among participants older than age 40 years (p < 0.001) and living in urban areas (p = 0.001), in comparison with their counterparts. Participants aged more than 40 years were 0.2 times more likely to be hospitalized than those aged 18 to 40 years, and respondents living in urban areas had a 3.6-times higher risk of being hospitalized as compared with their counterparts. Additionally, univariate analysis revealed that educational level was a significant predictor of hospitalization (p = 0.014). Educational level was associated with a 1.2-times increased risk of hospitalization, as shown in Table 4.
Association of sociodemographic and lifestyle variables with hospital admission among participants.
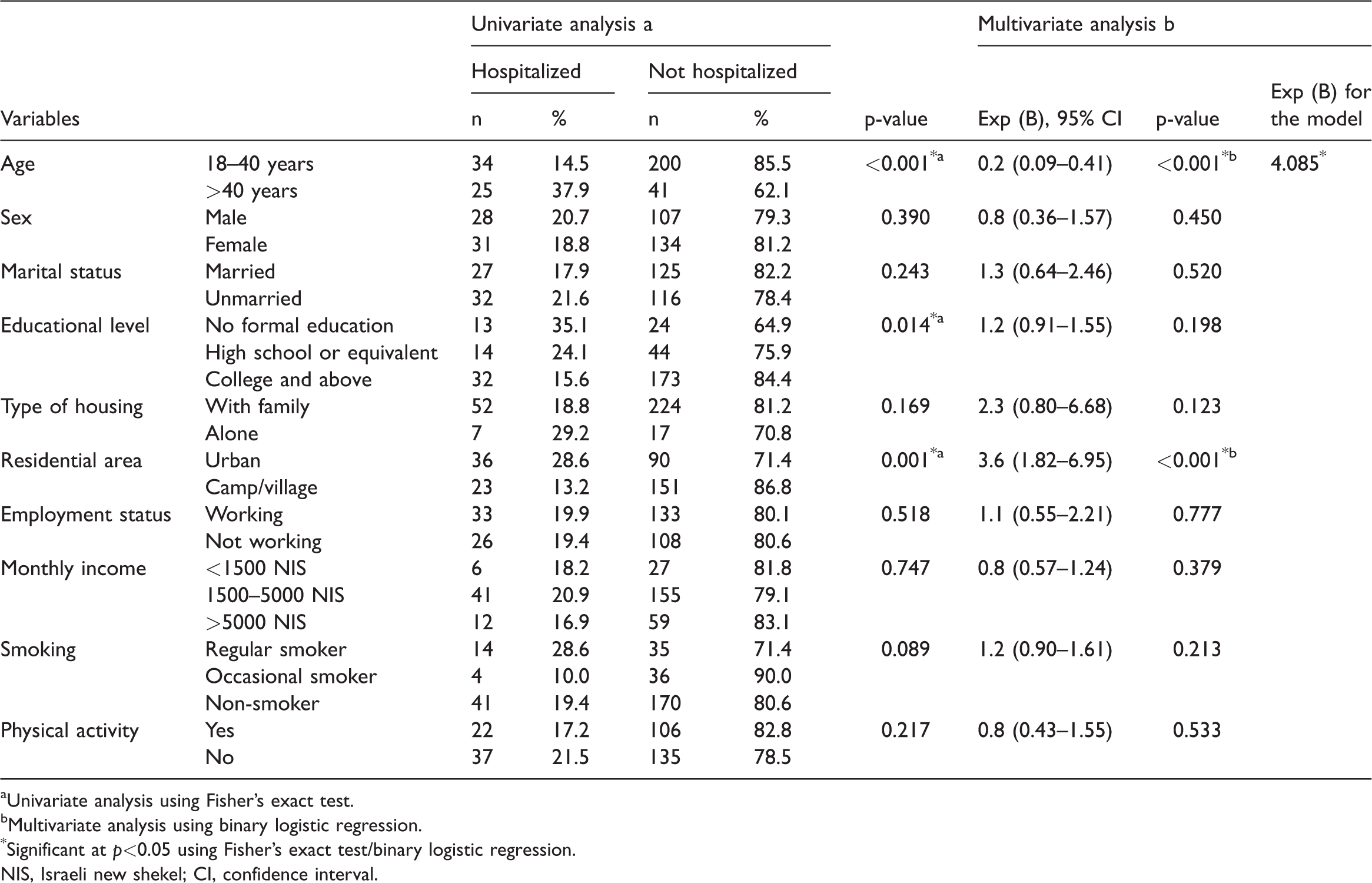
aUnivariate analysis using Fisher’s exact test.
bMultivariate analysis using binary logistic regression.
*Significant at p<0.05 using Fisher’s exact test/binary logistic regression.
NIS, Israeli new shekel; CI, confidence interval.
Hospitalization and participants’ medical history
With respect to participants’ medical profile, diabetes mellitus, hypertension, and respiratory diseases were associated with being hospitalized in univariate analysis (Table 5), as compared with participants who did not have these comorbidities. Participants with either respiratory diseases or diabetes mellitus were 0.3 times more likely to be hospitalized than their counterparts whereas those with hypertension had a 0.4-times higher risk of being hospitalized in comparison with those who did not have hypertension. Cardiovascular diseases were also related to hospitalization in both univariate and multivariate analysis. The proportion of non-hospitalized patients was significantly lower among those without cardiovascular diseases (9.1%) as compared with patients who had cardiovascular diseases (90.9%). Participants with cardiovascular disease were 0.1 times more likely to be hospitalized than those without cardiovascular disease.
Association of comorbidities with hospital admission among participants.

aUnivariate analysis using Fisher’s exact test.
bMultivariate analysis using binary logistic regression.
*Significant at p < 0.05 using Fisher’s exact test/binary logistic regression.
CI, confidence interval.
Hospital admission and participants’ habits before and during COVID-19 infection
Multivariate analysis and univariate analysis confirmed that the number of snacks consumed per day before COVID-19 infection was a significant predictor of hospitalization. The number of snacks consumed per day prior to being infected with SARS-CoV-2 increased the risk of hospitalization by 0.6 times. Moreover, multivariate analysis revealed that the number of meals consumed per day prior to COVID-19 infection was a significant predictor of hospitalization. The number of meals consumed per day before being infected with SARS-CoV-2 decreased the risk of hospitalization by 0.5 times, as shown in Table 6. In terms of anthropometric measurements, BMI showed a significant association with hospitalization in both univariate and multivariate models. We observed that the prevalence of hospitalization was significantly more common among obese participants (40.0%) compared with normal-weight participants (12.6%). Obesity increased the risk of hospitalization by 0.4 times (Table 7).
Risk factors for hospital admission.
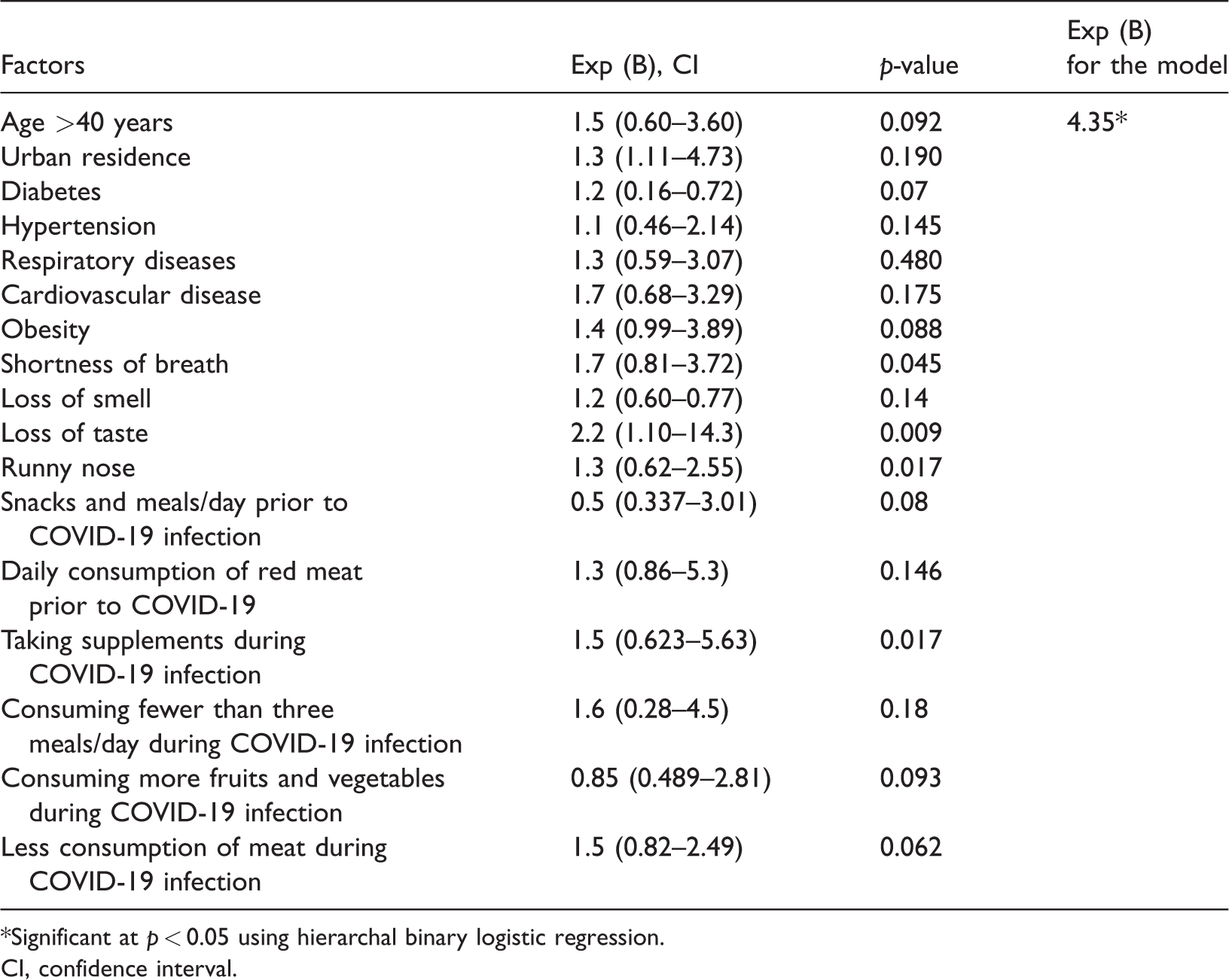
*Significant at p < 0.05 using hierarchal binary logistic regression.
CI, confidence interval.
Association of BMI, dietary habits, and lifestyle factors prior to COVID-19 infection with hospital admission.
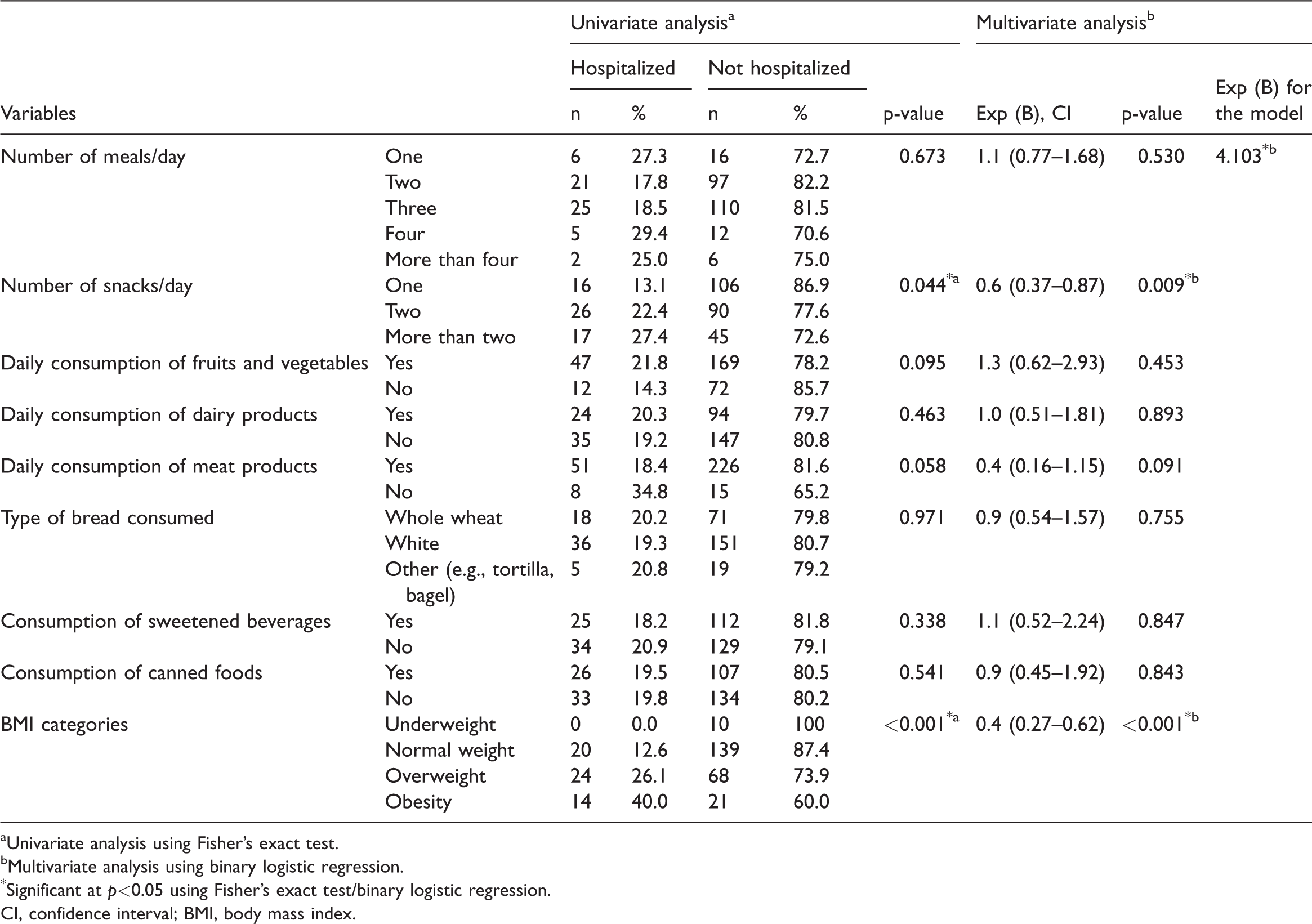
aUnivariate analysis using Fisher’s exact test.
bMultivariate analysis using binary logistic regression.
*Significant at p<0.05 using Fisher’s exact test/binary logistic regression.
CI, confidence interval; BMI, body mass index.
Both models showed that taking dietary supplements and daily consumption of meat products during the period of COVID-19 infection were associated with hospitalization. Interestingly, we noted that the frequency of hospitalization was significantly more prevalent among participants who did not consume meat products on a daily basis (40.9%) and those who took dietary supplements (25.7%) during the period of COVID-19 infection, in comparison with their counterparts who consumed meat products daily (18.0%) and did not take dietary supplements (9.7%). Participants who were taking dietary supplements and were not consuming meat on a daily basis were 0.3 times more likely to be hospitalized (Table 8). In the multivariate analysis, the number of meals and snacks consumed per day during the infection period was shown to be a significant risk factor for hospitalization. The number of meals consumed per day during the infection period increased the risk of being hospitalized by 1.7 times. Our univariate analysis also revealed that the prevalence of hospitalization was significantly higher among participants who changed their dietary habits during the infection period (27.8%) and consumed fruits and vegetables on a daily basis (22.8%) compared with those who did not do so (14.6%). Participants who changed their dietary habits during the period of COVID-19 infection had a 1.5-times higher risk of being hospitalized than those who made no changes to their dietary habits during infection. Moreover, daily consumption of fruits and vegetables increased the risk of hospitalization by 1.7 times (Tables 6, 8, and 9).
Association of BMI, dietary habits, and lifestyle factors during COVID-19 infection with hospital admission.
aUnivariate analysis using Fisher’s exact test.
bMultivariate analysis using binary logistic regression.
*Significant at p<0.05 using Fisher’s exact test/binary logistic regression.
CI, confidence interval.
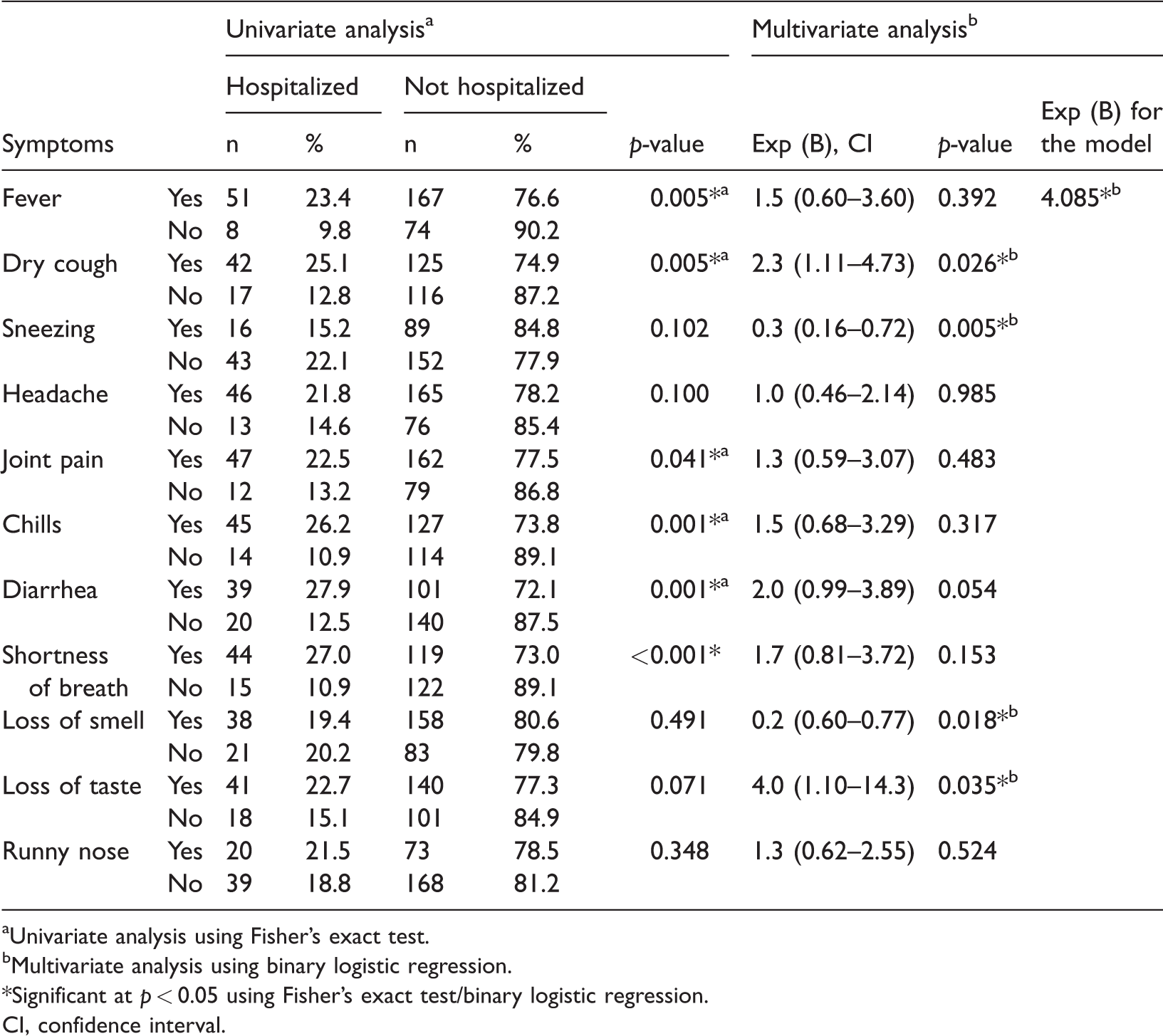
Association of COVID-19-related symptoms with hospital admission.

aUnivariate analysis using Fisher’s exact test.
bMultivariate analysis using binary logistic regression.
*Significant at p < 0.05 using Fisher’s exact test/binary logistic regression.
CI, confidence interval.
Hospital admission and participants’ symptoms
Participants with the following symptoms were hospitalized less often than expected: fever, dry cough, joint pain, chills, diarrhea, shortness of breath, and loss of taste. Other symptoms, including loss of smell and sneezing, resulted in hospitalization rates that were greater than expected (p < 0.05).
We performed an analysis of all significant variables. The analysis revealed that participants who had a loss of taste were 2.2 times more likely to be hospitalized than those who did not have a loss of taste, and patients with shortness of breath were 1.7 times more likely to be hospitalized than those who did not have this symptom. We also found that participants who were taking dietary supplements during the period of COVID-19 infection had a 1.5-times higher risk of being hospitalized than their counterparts. Furthermore, we noted that participants with symptoms of a runny nose had a 1.3-times higher risk of being hospitalized than their counterparts without this symptom.
Discussion
In the current study, we targeted demographic characteristics, medical history, signs and symptoms, and dietary habits to identify possible predictors of COVID-19 hospitalization.
The present study findings demonstrated that approximately 19.7% of participants in our study in Hebron city, Palestine had a high risk of hospitalization. The prevalence of hospitalization in our sample was generally lower than that reported in previous studies in New York (52%) 23 and Massachusetts (31%). 24 In contrast, the prevalence of hospitalization among our participants was slightly higher than that reported in studies conducted in Brazil (10.8%) 25 and the United Kingdom (0.2%). 26
We found that older participants were more likely to be hospitalized, which is supported by former studies.8,23,25,27 Although it is not yet evident why this correlation occurs, many interpretations have been suggested by investigators, such as greater contact with and more evolved immune responses to other viruses,28,29 greater incidence of comorbidities, 30 and reduced angiotensin-converting enzyme 2 (ACE2) protein expression among older people. 31
The current findings also showed that there was no significant relationship between participants’ sex and hospitalization. This is in contrast to the results of other studies15,23,25 reporting that COVID-19-associated hospitalization rates are greater among male patients than female patients.
Our findings revealed that hospitalization was significantly more prevalent among participants with higher education levels (e.g., bachelor's, master's, or doctoral degree) compared with their counterparts who did not complete their schooling. This finding is supported by those of a study by Wang and colleagues. 24 We also explored the relationship between area of residence and COVID-19 hospitalization. Hospitalization rates were significantly higher among individuals who were living in cities in comparison with individuals living in either a camp or village. The relationship between these variables and hospitalization has not been previously reported.
Consistent with former studies,25,26,32–34 our study findings showed that obese participants are more likely to be hospitalized with COVID-19 infection. Obesity is considered a pro-inflammatory condition and that obesity stimulates oxidant stress to negatively influence cardiovascular function.35,36 Furthermore, having extra weight in the abdomen beneath the diaphragm makes the respiration process more difficult by reducing diaphragm excursion. Obesity also weakens the immune responses to viral infection. 37
Our findings showed that diabetes mellitus, hypertension, cardiovascular diseases, and pulmonary diseases were significantly more prevalent among patients with COVID-19-associated hospitalization. This finding was in agreement with previous literature.25,32–34
Smoking has been confirmed as a predictor of disease severity, such as in pulmonary diseases. 38 However, our study showed that smoking was not associated with COVID-19 hospitalization. This finding was inconsistent with those of a Brazilian study, 25 which reported that smoking is a strong predictor for COVID-19 hospitalization; the prevalence of smokers who were hospitalized in that study was more than three times greater than the prevalence of hospitalized non-smokers.
Fever was the most common symptom in the current study as well as in past studies.25,27,39,40 The overwhelming majority of our participants reported at least one symptom (96.7%). Our analysis revealed that all symptoms, except runny nose and headache, were important in explaining hospitalization. In contrast, Soares and colleagues found that symptoms of runny nose and headache were related to a reduced risk of COVID-19 hospitalization. 25
According to the current study findings, certain dietary habits either before or during the infection period were significantly associated with a high risk of hospitalization. Surprisingly, we found that meat consumption during the infection period decreased the risk of hospitalization in our participants. Additionally, we found that consuming more than two snacks per day either before or during the infection period increased the hospitalization risk. The association between dietary habits and risk of hospitalization has not been reported previously.
We demonstrated that changing dietary habits, consuming one main meal per day, and consuming fruits and vegetables during the infection period increased the risk of hospitalization. Previous studies have not investigated the relationship between dietary habits and risk of hospitalization. It is possible that our participants had poor dietary habits prior to being infected with SARS-CoV-2, and as a result of feeling fatigue and distress during the infection period, they changed their dietary habits and consumed more fruits and vegetables.
We also found that taking dietary supplements during the COVID-19 infection period increased the risk of hospitalization. Previous studies have not explored the relationship between dietary supplements and risk of hospitalization owing to COVID-19. That individuals may take dietary supplements without a medical prescription or they may take them in large doses that may cause toxicity, which could lead to hospitalization, can explain our findings.
The findings of the current study must be considered within the framework of certain limitations. First, the main study limitation resides in the study design. Being a cross-sectional study, it was not possible to determine a causal relationship. Second, the study was limited to Hebron city and was not representative of the entire population with COVID-19 infection in Palestine. Third, complex interactions including among many variables may not be able to be clarified using multivariate logistic regression. 41 Fourth, dietary assessment was not included in the study. Fifth, we used self-reports, which increases the risk of error and bias. Finally, environmental variables were not considered in this study, for example, the use of biomass for cooking or exposure to chemical hazards. Such variables have been shown to increase vulnerability to developing acute COVID-19 infection that can result in hospitalization.42,43 Despite these limitations, our study can aid health care professionals in identifying individuals who may require additional attention, close monitoring, and access to preventive and therapeutic treatments. Further studies should focus on examining the association between dietary habits and COVID-19 hospitalization. Future research should also investigate the effect of different variables (e.g., dietary habits, sociodemographic, and clinical characteristics) on the period of hospitalization.
Conclusion
The current study results showed that the prevalence of hospitalization among our study population in Palestine was relatively low, compared with former studies. The present findings provide evidence that older age, living in urban areas, low education level, comorbidities (primarily hypertension, followed in descending order by diabetes mellitus, respiratory diseases, cardiovascular diseases), loss of smell, and sneezing are related to an elevated risk of hospitalization among patients with COVID-19. Fever, dry cough, joint pain, chills, diarrhea, shortness of breath, and loss of taste were found to be related to a reduced hospitalization risk. Moreover, we noted a higher likelihood of COVID-19 hospitalization with increased BMI. Surprisingly, our analysis revealed that daily consumption of meat during the infection period decreased the risk of hospitalization; in contrast, changing dietary habits, consuming one main meal per day, daily consumption of fruits, and taking dietary supplements during the infection period increased the risk of hospitalization. Additionally, we found that consuming more than two snacks per day either prior to or during the period of infection increased the risk of hospitalization owing to COVID-19. These findings may assist health care professionals to determine those patient groups at greater risk for hospitalization who may require greater monitoring and who may benefit from targeted therapeutic and preventive interventions.
Footnotes
Acknowledgements
We would like to acknowledge the students who helped the researchers in the data collection. We would like to express our gratitude to the patients who agreed to participate in this study. We also extend our thanks to all co-researchers and fieldworkers involved in this study.
Authors’ contributions
May Hamdan supervised the project and data collection. Manal Badrasawi was responsible for proposal revision and methodology optimization, supervision of data collection, and data analysis. Souzan Zidan was responsible for proposal revision and methodology optimization, supervision of data collection, data analysis, and writing the first draft. Asma Sayarah, Lamia Abu Zahra, Shahd Dana, and Tasneem Almasry were responsible for writing the review, drafting the proposal, collecting data, and data entry, and assisting in writing the proposal. All authors have read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.