
Abstract
Objective
Restrictive fluid therapy is recommended in thoracoscopic lobectomy to reduce postoperative pulmonary complications, but it may contribute to hypovolemia. Goal-directed fluid therapy (GDFT) regulates fluid infusion to an amount required to avoid dehydration. We compared the effects of GDFT versus restrictive fluid therapy on postoperative complications after thoracoscopic lobectomy.
Methods
In total, 124 patients who underwent thoracoscopic lobectomy were randomized into the GDFT group (group G, n = 62) or restrictive fluid therapy group (group R, n = 62). The fluid volume and postoperative complications within 30 days of surgery were recorded.
Results
The total fluid volume in groups G and R was 1332 ± 364 and 1178 ± 278 mL, respectively. Group R received a smaller colloid fluid volume (523 ± 120 vs. 686 ± 180 mL), had a smaller urine output (448 ± 98 vs. 491 ± 101 mL), and received more norepinephrine (120 ± 66 vs. 4 ± 18 µg) than group G. However, there were no significant differences in postoperative pulmonary complications, acute kidney injury, length of hospital stay, or in-hospital mortality between the two groups.
Conclusion
Restrictive fluid therapy performs similarly to GDFT in thoracoscopic lobectomy but is a simpler fluid strategy than GDFT.
Keywords
Introduction
Intraoperative fluid optimization is essential to improve the prognosis after thoracoscopic lobectomy. Wu et al. 1 found that differences in the infusion rate of total fluids or colloids during minimally invasive lobectomy were related to significant differences in postoperative pneumonia and postoperative pulmonary complications (PPCs). A liberal fluid scheme may lead to hypervolemia, resulting in pulmonary edema, pneumonia, atelectasis, empyema, and acute respiratory distress syndrome.2–4 A restricted fluid scheme is recommended by the Enhanced Recovery After Surgery Society and the European Society of Thoracic Surgeons. 5 Shin et al. 6 also pointed out that moderately restrictive fluid management may improve postoperative outcomes for most patients. However, the safe lower limit of restricted fluid therapy remains unclear. Patients undergoing such fluid management are susceptible to hypovolemia, deterioration of tissue perfusion, organ dysfunction, and acute kidney injury (AKI).6–9 Both liberal and restrictive fluid administration are associated with postoperative adverse effects.
Goal-directed fluid therapy (GDFT) can control fluid infusion to the amount required based on the patient’s fluid responsiveness. The stroke volume variation (SVV) and cardiac index (CI) have been shown to sensitively predict fluid responsiveness and cardiac function.10–12 A meta-analysis showed that GDFT may be the best way to improve renal perfusion and oxygenation by means of fluids and inotropes. 13
The Cheetah noninvasive continuous cardiac output monitoring (NICOM) system (Cheetah Medical, Newton Center, MA, USA), a totally noninvasive bioreactance-based monitor, uses four electrodes placed on the chest to measure changes in the frequency of the electrical currents from which hemodynamic variables, including the CI, stroke volume (SV), and SVV, can be calculated. This NICOM system has been validated for acceptable clinical precision and accuracy when compared with the pulmonary artery catheter and pulse index continuous cardiac output catheter;14,15 it also avoids the disadvantages of these catheters, such as high cost, high invasiveness, and many serious complications. As a noninvasive hemodynamic monitor, the NICOM system is regarded as a valuable alternative to invasive hemodynamic monitoring. Studies have shown that GDFT based on NICOM is associated with a smaller volume of fluids, fewer postoperative complications, faster gastrointestinal function recovery, and a shorter hospital stay. 16 We therefore chose the NICOM system to monitor the SVV, CI, and other hemodynamic parameters.
Existing knowledge about the impacts of intraoperative fluids on the prognosis has been drawn from studies comparing two different fluid management strategies (restrictive vs. liberal and GDFT vs. liberal). However, no prospective study has compared GDFT based on NICOM versus restrictive fluid therapy in thoracoscopic lobectomy. Therefore, this prospective trial was performed to compare the effects of GDFT based on NICOM versus restrictive fluid therapy on postoperative complications after thoracoscopic lobectomy.
Methods
Participants
The reporting of this study conforms to the CONSORT statement. 17 This study was approved by the Medical Ethics Committee of Yongchuan Hospital of Chongqing Medical University (2020 Collen trial 30) and registered at the Chinese Clinical Trial Registry (ChiCTR2100046349) (http://www.chictr.org.cn/index.aspx). This prospective comparison study was conducted from October 2020 to May 2021 in Yongchuan Hospital of Chongqing Medical University. Written informed consent was provided by the patients and their families.
Patients who were scheduled for thoracoscopic lobectomy in our hospital were enrolled in this trial. They were allocated to either the GDFT group (group G) or restrictive fluid therapy group (group R) in a 1:1 ratio by a computer-based random number generator. Numbers were concealed in sealed opaque envelopes and were not opened before anesthetic induction. The exclusion criteria were an American Society of Anesthesiologists classification of ≥III; body mass index of >28 kg/m2; serious heart, liver, brain, lung, kidney, metabolic, or central nervous system diseases; and skin defects that prevented measurement by NICOM.
Study protocol
All patients fasted for 8 hours for solids and 2 hours for liquids before the operation and were monitored by electrocardiography, noninvasive blood pressure measurement, and peripheral pulse oximetry. After administration of local anesthesia, the patients underwent catheterization of the radial artery and internal jugular vein to monitor the mean arterial pressure (MAP) and central venous pressure. All patients were managed using the same anesthetic scheme by the same anesthesiologist. Anesthesia was induced with sufentanil (0.4 µg/kg), etomidate (0.3 mg/kg), and rocuronium (0.6 mg/kg) and maintained with sevoflurane, propofol, and sufentanil boluses to keep the bispectral index at 40 to 60. One-lung ventilation was performed with a double-lumen tube during the operation, and a lung-protective ventilation scheme was used with a tidal volume of 4 to 6 mL/kg ideal body weight, positive end-expiratory pressure of 5 to 10 cmH2O, and use of recruitment maneuvers. A recruitment maneuver was defined as 30 s of continuous positive airway pressure at 30 cmH2O every 30 minutes. 18 An infusion heater and heating blanket were used to keep the patient’s body temperature at ≥36°C. Paravertebral nerve block was performed under ultrasound guidance after induction of general anesthesia. Patient-controlled analgesia was used for postoperative analgesia. The patients resumed drinking, eating, ambulation, incentive spirometry, and respiratory physiotherapy as early as possible after surgery.
Group G was equipped with the NICOM system to monitor the SVV and CI. The SVV was controlled from 10% to 13%, and the CI was maintained at a minimum of 2.5 L/minute · m2. 19 The baseline infusion was 2 mL/kg/hour compound sodium chloride; when the SVV was >13% for at least 2 minutes, an additional 250 mL of succinylated gelatin was infused within 5 minutes. A fluid challenge was repeated until the SVV was <13%. Norepinephrine was administered if the CI remained below 2.5 L/minute · m2 despite preload optimization. The hemodynamic status was recorded every 10 minutes.
Group R was treated with a restrictive fluid scheme: the baseline infusion was 2 mL/kg/hour compound sodium chloride, and succinylated gelatin was infused to supply blood loss with a colloid to blood loss ratio of 1:1 (mL). Norepinephrine was administered by the anesthesiologists according to their experience to maintain the MAP at >65 mmHg.
All the patients were treated by the same surgical group. All patients and surgeons were blinded. The observation indicators were as follows: perioperative fluid volume (total fluid volume, colloid volume, and crystalloid volume), estimated blood loss volume, blood products, norepinephrine administration, urine output, PPCs, AKI, length of hospital stay (LOS), and in-hospital mortality.
Definitions of primary and secondary outcomes
PPCs 2 were defined as pneumonia, atelectasis, acute respiratory distress syndrome, reintubation, need for bedside bronchoscopy, pulmonary embolism, prolonged air leakage, and failure to expand. AKI 6 was defined as an increase in serum creatinine by at least 0.3 mg/dL or 50% from the preoperative level within 48 hours postoperatively or the existence of an AKI diagnostic code within 7 days postoperatively.
Statistical analysis
According to a relevant statistical study, 19 the incidence of PPCs and AKI is 35.7% and 5.9% in patients undergoing liberal infusion and GDFT. The sample size of the present trial was calculated using PASS 15.0 software (NCSS LLC, Kaysville, UT, USA) to achieve a power of 0.8 and an alpha of 0.05 with a two-sided test. Considering a 10% rate of potential dropouts, 62 patients were required per group. Analyses were conducted using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). Continuous data are expressed as mean ± standard deviation and were compared by independent-samples t tests. Categorical variables are expressed as percentage and were analyzed using the r × c chi-square test; when the theoretical frequency was <5, Fisher’s exact test was used. Differences with a P value of <0.05 were considered statistically significant.
Results
In total, 124 patients scheduled for thoracoscopic lobectomy were enrolled in this study, and 6 patients were excluded from the data analysis because of conversion to thoracotomy. Therefore, 118 patients were included in the analysis and randomized into group G (n = 59) and group R (n = 59). The patients’ baseline characteristics were similar between the two groups. There were no statistically significant differences in the anesthesia duration or operative duration between the groups (Table 1).
Patients’ baseline characteristics and clinical data in the two groups.

Data are presented as n or mean ± standard deviation.
BMI, body mass index; ASA, American Society of Anesthesiologists; Hb, hemoglobin; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second.
Comparison of intraoperative fluid inflow and outflow and vasoactive drugs
Compared with group G, group R was administered a smaller total fluid volume (1178 ± 278 vs. 1332 ± 364 mL), was administered a smaller colloid fluid volume (523 ± 120 vs. 686 ± 180 mL), and had a smaller urine output (448 ± 98 vs. 491 ± 101 mL) (P < 0.05). Norepinephrine was used more frequently in group R than in group G to correct hypotension (P < 0.05). No significant differences were found in the crystalloid volume, blood loss, or blood products between the two groups (Table 2).
Comparison of intraoperative fluid inflow and outflow.
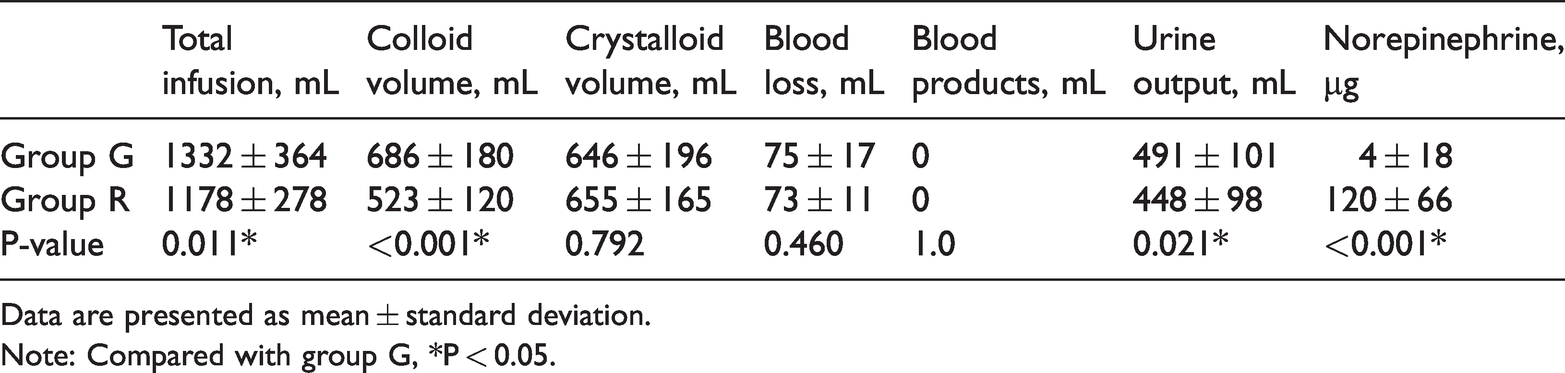
Data are presented as mean ± standard deviation.
Note: Compared with group G, *P < 0.05.
Comparison of postoperative prognosis.
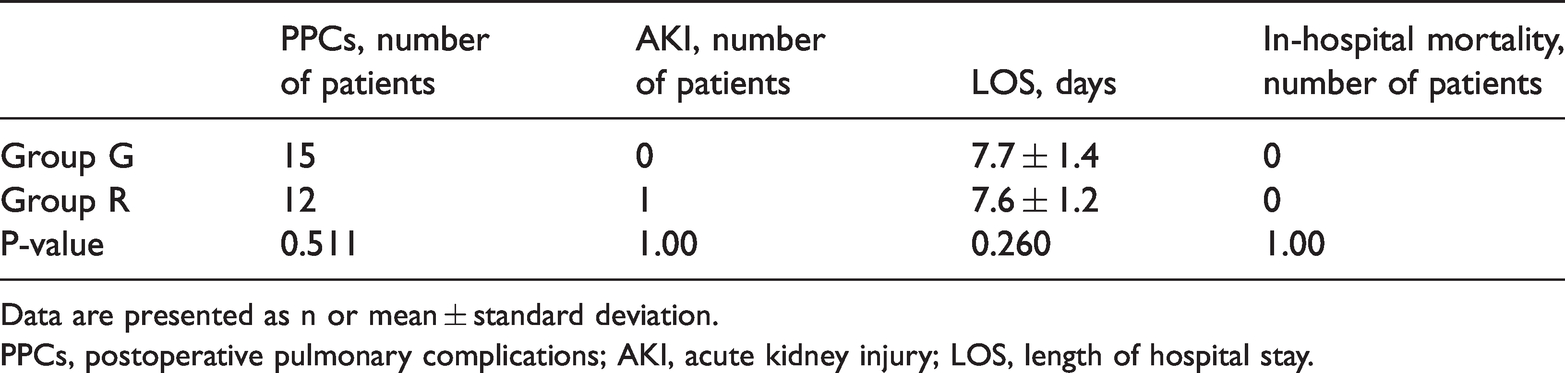
Data are presented as n or mean ± standard deviation.
PPCs, postoperative pulmonary complications; AKI, acute kidney injury; LOS, length of hospital stay.
Comparison of postoperative complications between groups
The PPCs, AKI, LOS, and in-hospital mortality were not different between the two groups. The intervention caused no harm, and no patients died during the trial period.
Discussion
In this study, group R received a smaller total fluid volume, received a smaller colloid fluid volume, and had a smaller urine output than group G. Norepinephrine was used more frequently in group R than in group G to correct hypotension. However, there were no significant differences in the PPCs, AKI, LOS, or in-hospital mortality.
An appropriate fluid scheme during thoracoscopic lobectomy is considered to be an integral part of anesthetic management by reducing postoperative complications. Single-lung ventilation, a non-physiological ventilation technique, is widely used in thoracoscopic lobectomy. However, single-lung ventilation may cause changes in the alveolar endothelial cells, resulting in a decreased fluid clearance rate in the alveoli. 20 It places patients at heightened risk for pulmonary edema, lung infections, and respiratory failure. Although a restricted fluid scheme is recommended in thoracoscopic lobectomy, uncontrolled fluid restriction may result in hypovolemia-related complications such as tissue hypoxia, which plays a key role in organ dysfunction. Moreover, untreated hypovolemia and prerenal azotemia may lead to acute tubular necrosis and renal dysfunction. 21 It is generally considered that liberal fluid administration is significantly associated with respiratory complications, whereas both liberal and restrictive fluid administration are significantly associated with AKI. 6
The SVV reflects variations in left ventricular output secondary to intrathoracic pressure changes induced by mechanical ventilation and represents the percentage of change between the maximum and minimum SVs over a period divided by their average value. The SVV has been shown to be an accurate predictor of the fluid response10,11 and can be used as a resuscitation endpoint to evaluate postoperative recovery. When arterial oxygen saturation and hemoglobin levels are adequate, the CI can serve as an effective measurement index to evaluate the oxygen supply within tissues and organs. 12 GDFT based on the SVV and CI, optimizing not only the intraoperative infusion volume but also the end-organ perfusion, can decrease the content of extravascular lung water. 22 Colloids can reduce the incidence of PPCs by increasing the plasma colloid osmotic pressure and reducing pulmonary edema to keep the lung dry. 23 Additionally, an intraoperative colloid infusion rate of >3.8 mL/kg/hour has been shown to be associated with a lower incidence of postoperative pneumonia and PPCs without increasing the risk of postoperative AKI. 1 We therefore perform fluid challenges with colloids instead of crystalloids.
Norepinephrine was administered to maintain the MAP at > 65 mmHg in our study. We observed that norepinephrine was used more frequently in group R than in group G to correct hypotension. This indicates that the relative hypovolemia in group R could be reversed by a vasopressor, which was conductive to counteract vasodilation. Although group R received a smaller total fluid volume, received a smaller colloid fluid volume, had a smaller urine output, and received a larger amount of norepinephrine, there were no significant differences in the PPCs, AKI, LOS, or in-hospital mortality. Thus, restrictive fluid therapy is safe and feasible in thoracoscopic lobectomy. Taking all the above factors into consideration, restrictive fluid therapy performs similarly to GDFT in terms of postoperative complications in thoracoscopic lobectomy, but it is simpler to manage than GDFT.
Our study has several limitations. We did not regulate the postoperative fluid treatment, which may have influenced the effect of intraoperative therapy. Although we attempted to exclude potential confounding factors, some other factors such as social and genetic factors may have interfered with the accuracy of the results. In addition, this was a single-center study; hence, a multicenter study may mitigate the potential limitations.
Conclusions
Restrictive fluid therapy performs similarly to GDFT in thoracoscopic lobectomy with respect to PPCs, AKI, LOS, and in-hospital mortality. However, restrictive fluid therapy is a simpler fluid strategy than GDFT.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211062787 - Supplemental material for Prospective comparison of the effects of intraoperative goal-directed fluid therapy and restrictive fluid therapy on complications in thoracoscopic lobectomy
Supplemental material, sj-pdf-1-imr-10.1177_03000605211062787 for Prospective comparison of the effects of intraoperative goal-directed fluid therapy and restrictive fluid therapy on complications in thoracoscopic lobectomy by Min Li and Mingqing Peng in Journal of International Medical Research
Footnotes
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
This study was approved by the Medical Ethics Committee of Yongchuan Hospital of Chongqing Medical University (2020 Collen trial 30) and was performed only after written informed consent was provided by the participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by a specific grant from the Graduate Innovation Fund of Yongchuan Hospital of Chongqing Medical University.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.