
Abstract
Objective
Spondylodiscitis is an important clinical a problem requiring serious approaches. In this study, we sought to raise awareness by examining the epidemiology and laboratory, clinical, and radiological findings of spondylodiscitis, which sometimes has a delayed diagnosis and which can be difficult to treat.
Methods
In total, 343 patients with spondylodiscitis were included in the study.
Results
The patients were classified as having as pyogenic (n = 153, 44.6%), brucellar (n = 138, 40.2%), or tuberculous (n = 52, 15.2%) spondylodiscitis. Meanwhile, 281 patients underwent magnetic resonance imaging, 71 underwent computed tomography, and 17 underwent scintigraphy for diagnosis. The rates of involvement at more than two segments and paraspinal abscess were significantly higher in tuberculous spondylodiscitis. However, disc involvement was significantly more common in brucellar and pyogenic spondylodiscitis.
Conclusion
The incidence of spondylodiscitis has increased substantially, especially in the young population. The invasive procedures and high rate of culture negativity make the diagnosis difficult. Therefore, clinical and radiological findings are useful in the diagnosis of spondylodiscitis. Despite the high rate of culture negativity, every effort should be made to identify the causative organism using invasive methods.
Introduction
Spondylodiscitis is an infection of vertebrae and the adjacent disc structures, and it usually occurs in adults. 1 In recent years, its prevalence has increased, leading to longer hospitalization; therefore, it is an important burden for both patients and the health system. 2 The reasons for the increased prevalence may include the growing elderly population, the increased number of patients on dialysis, and the increased number of patients with immunosuppression. 3 The nonspecific symptoms of spondylodiscitis may lead to confusion with other spinal diseases, thereby delaying diagnosis. Despite the importance of culture, typical radiological findings are useful in cases in which histopathology cannot be performed and in cases of negative culture. 4
Spondylodiscitis is extremely difficult to treat and diagnose, as low back or neck pain is often not considered because of mechanical disorders of the spine and invasive procedures are required for a definitive diagnosis, and it often requires long-term treatment and hospitalization. In this study, we examined the epidemiology, risk factors, and laboratory, clinical, and radiological findings of spondylodiscitis.
Materials and methods
Patients older than 18 years old with clinical, radiological, and/or microbiological evidence of spondylodiscitis who underwent follow-up and treatment between January 2012 and December 2018 were included in the study. This was a retrospective multicenter study (Gazi Yasargil Training and Research Hospital and Umraniye Training and Research Hospital), and ethics committee approval was obtained from the Ethics Committee of Gazi Yasargil Training-Research Hospital of The University of Health Sciences (Approval number: 294, approval date: June 14, 2019). All participants provided written informed consent.
The following data of the patients were recorded: age, sex, underlying diseases, symptoms, infection site, white blood cell, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) level, culture findings, causative microorganisms, radiological imaging methods, and duration of hospitalization. The data were obtained from the hospital automation system and patient files. Then, the patients were divided into three groups based on a diagnosis of pyogenic, tuberculous, or brucellar spondylodiscitis. Patients in whom pyogenic bacteria were isolated from samples obtained under interventional radiology or from intraoperative tissue samples and/or blood cultures and culture-negative patients who were cured with antibiotic treatment were diagnosed with pyogenic spondylodiscitis. Patients with Brucella tube agglutination ≥1/160 and/or Brucella growth in abscess and/or blood culture were diagnosed with brucellar spondylodiscitis. Patients with Mycobacterium tuberculosis growth in radiology-guided or intraoperative tissue samples and/or blood cultures and those who were considered to have tuberculosis clinically, laboratory and radiologically were diagnosed with tuberculous spondylodiscitis.
The reporting of this study conforms to STROBE guidelines. 5
Statistical analysis
All statistical analyses were performed using SPSS version 19.0 for Windows (IBM Corp., Armonk, NY, USA). Data are presented as the mean, standard deviation, and percentage. The one-sample Kolmogorov–Smirnov test was used to confirm that results followed a normal distribution. The Kruskal–Wallis test was applied to compare means, and Pearson’s chi-squared test was used to compare qualitative data. The results were evaluated using hazard ratios and 95% confidence intervals. In these analyses, P < 0.05 denoted statistical significance.
Results
In total, 343 patients who received follow-up after a diagnosis of spondylodiscitis were included in our study. Of these patients, 183 (53.4%) were men, and the mean age of the patients was 43.56 ± 15.91 years (range, 18–89). The demographic and clinical features and underlying conditions of the patients are presented in Table 1. Specifically, 71.1% of patients exhibited involvement of the lumbar vertebrae. Abscess was present in 146 patients (42.6%), whereas 24 patients (7%) had neurological deficits. Laboratory results are presented in Table 1. Using blood cultures, Brucella spp., methicillin-susceptible Staphylococcus aureus (MSSA), and methicillin-resistant S. aureus (MRSA) were detected in 6.1%, 5%, and 3.8% of patients, respectively (Figure 1). Among 139 patients whose tissue/abscess culture was taken, M. tuberculosis and MRSA were detected in 8.7% and 5.5% of patients, respectively (Figure 1). In addition, 281 patients underwent magnetic resonance imaging (MRI), 71 underwent computed tomography (CT), and 17 underwent scintigraphy for diagnosis. Five patients underwent both CT and scintigraphy, 10 patients underwent both MRI and CT together, and 11 patients underwent both MRI and scintigraphy. The mean treatment period was 18.5 ± 13.18 weeks (range, 4–48).
Baseline characteristics of the patients with spondylodiscitis.
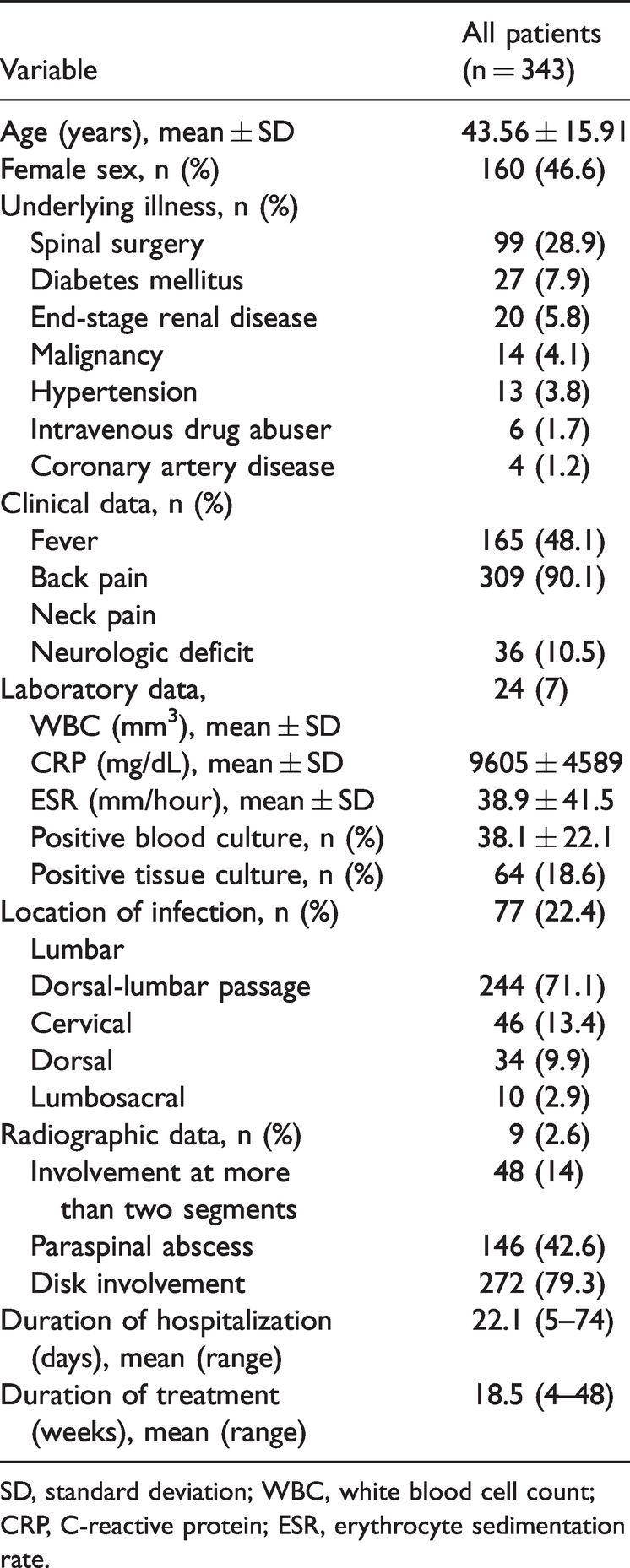
SD, standard deviation; WBC, white blood cell count; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate.

Bacteria isolated from the blood and tissue cultures of patients with spondylodiscitis.
The patients were categorized as having pyogenic (44.6%), brucellar (40.2%), or tuberculous spondylodiscitis (15.2%). The demographic, clinical, laboratory, and radiological findings and treatment periods of these groups were compared, as presented in Table 2. Patients diagnosed with tuberculous spondylodiscitis were significantly older, and their body temperature was significantly higher (both P < 0.001). Compared with the findings in the brucellar spondylodiscitis group, the incidence of neurological deficits was higher in the pyogenic and tuberculosis spondylodiscitis groups (both P < 0.001). White blood cell counts, CRP levels, and ESR were significantly higher in patients with tuberculous spondylodiscitis (all P < 0.001). Patients with pyogenic and brucellar spondylodiscitis mostly had lumbar vertebral involvement, whereas patients with tuberculous spondylodiscitis mostly had thoracolumbar vertebral involvement. The rates of involvement at more than two segments and paraspinal abscess were significantly higher in patients with tuberculous spondylodiscitis (both P < 0.001). However, disc involvement was significant in patients with brucellar and pyogenic spondylodiscitis (P < 0.001). The duration of hospitalization period was longer in patients with pyogenic or tuberculosis spondylodiscitis (both P < 0.001).
Comparison of patients with pyogenic, brucellar, and tuberculous spondylodiscitis.

SD, standard deviation; WBC, white blood cell count; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate.
One patient (0.3%) who underwent follow-up after a diagnosis of tuberculous spondylodiscitis died. Surgery was performed in addition to medical treatment in 96 patients (28%), and CT-guided abscess drainage was performed in addition to medical treatment in 40 patients (11.7%). Of the patients who underwent surgery, 68 (70.8%) had pyogenic spondylodiscitis, and 28 (29.2%) had tuberculous spondylodiscitis. In addition, 10 (25%), 10 (25%), and 20 patients (50%) who underwent CT-guided abscess drainage had pyogenic, tuberculous, and brucellar spondylodiscitis, respectively. In total, 207 (60.3%) patients received only medical treatment, including 75 patients (36.2%) with pyogenic spondylodiscitis, 118 patients (57%) with brucellar spondylodiscitis, and 14 patients (6.8%) with tuberculous spondylodiscitis.
Meanwhile, 230 patients (67%) were treated empirically, including 20 (8.7%) and 98 patients (42.6%) with tuberculous and pyogenic spondylodiscitis, respectively. Among patients who received empirical treatment, neurological deficits developed in 5 (25%) and 17 patients (17.3%) with tuberculous and pyogenic spondylodiscitis, respectively. Sequelae did not develop in 112 patients with brucellar spondylodiscitis who received empirical treatment.
Discussion
Because of advances in diagnostic methods in recent years, the number of patients with spondylodiscitis has increased.6,7 In two separate studies involving similar groups, the number of cases of spondylodiscitis among patients with S. aureus bacteremia rose from 1.1% in 1980 to 2.2% in 1990.8,9 In some cases, patients with spondylodiscitis partially respond to antimicrobials, but even among responders, it may take a long time to achieve complete remission. Therefore, early diagnosis and treatment are extremely important for improving outcomes and decreasing neurological sequelae and the socioeconomic burden. It is difficult to identify the etiology of these highly prevalent infections, and the selection of treatment is difficult for both patients and doctors; therefore, it is important to study these infections in large case series.
In this article, we examined 343 patients, including 153 patients with pyogenic spondylodiscitis, 138 patients with brucellar spondylodiscitis, and 52 patients with tuberculous spondylodiscitis. Although previous studies reported that spondylodiscitis is commonly observed in elderly patients and patients with comorbid diseases, 1 the mean patient age in this study was 43.5 years. The reason for this finding might be increased rates of comorbidity, and spinal surgery has been common in recent years even among younger patients. The symptoms of spondylodiscitis are nonspecific, as 90.1% of the patients in our study had lumbar pain. Nevertheless, it should be remembered that some patients may not have pain, 10 and spondylodiscitis should definitely be considered in the differential diagnosis in cases of unclear etiology. Fever is generally present in half of patients with spondylodiscitis, but fewer than half of our patients had fever. This illustrates that spondylodiscitis should definitely be considered in patients with vertebral pain regardless of the presence of fever. Neurological deficits were present in one-third of patients. This finding has been attributed to epidural abscess, delayed diagnoses, and cervical involvement.11,12 Only 7% of our patients had neurological deficits, including 17 patients (5%) with pyogenic spondylodiscitis, 6 patients (1.7%) with tuberculous spondylodiscitis, and 1 patient (0.3%) with brucellar spondylodiscitis. Because our study is retrospective, we do not know the duration from the onset of symptoms to the onset of treatment. Therefore, we cannot comment on the low rate of neurological deficits in our study. However, the low rate of cervical involvement is in line with previous findings. The most commonly involved region is the lumbar vertebral region because of the high numbers of patients with pyogenic or brucellar spondylodiscitis. In fact, the most common site of involvement is the thoracolumbar region in patients with tuberculous spondylodiscitis. In a systematic review, 52% (n = 919), 22% (n = 384), and 26% (n = 461) of patients exhibited lumbosacral, cervical, and thoracic involvement, respectively. 13
Spondylodiscitis is most frequently caused by a single microbe, and S. aureus is reported as the most common cause. Depending on the predisposition of patients, other microbes are identified less frequently.14,15 In a review of 212 patients with chronic renal failure and spondylodiscitis, the most common causative organism was S. aureus, followed by S. epidermidis and gram-negative bacteria. 16 In one review, microbiological data were available for 1060 of 1756 patients. Staphylococcus spp., M. tuberculosis, and other bacteria were the causative agents in 40.3%, 30.9%, and 28.3% of patients, respectively. 13 The most common causative organism was also S. aureus in our study, and its methicillin resistance rate was high. We suggest that the high prevalence of MRSA may be associated with the increased rate of MRSA infection in society in recent years and the presence of nosocomial infection following spinal surgery in most of our patients. This study was conducted in an endemic region in terms of brucellosis, and we know that tuberculosis is highly prevalent. In addition, the rate of extrapulmonary tuberculosis has risen in recent years. Therefore, we believe that these two diseases should not be ignored in patients with spondylodiscitis, and our study supported this supposition. However, it should be remembered that the number of culture-negative cases was considerable. One reason for this may be that tissue/abscess/blood cultures are obtained after antimicrobial therapy is initiated. Therefore, it is more appropriate to start treatment after diagnostic cultures in patients without sepsis.
In spondylodiscitis, white blood cell counts may increase or remain at normal levels. The levels of acute-phase reactants are usually high.17,18 Hamidi et al. 19 reported a significant difference in the levels of acute-phase reactants between patients with pyogenic spondylodiscitis and those with brucellar or tuberculous spondylodiscitis. In our study, the levels of acute-phase reactants were increased in all three groups, but the highest levels were observed in patients with tuberculous spondylodiscitis. Radiologically, the literature indicates that the most common site of involvement in patients with tuberculous spondylodiscitis cases is the thoracic vertebral region. Lumbar vertebral involvement is also common in pyogenic and brucellar spondylodiscitis. 20 In our study, lumbar involvement was common in patients with pyogenic or brucellar spondylodiscitis, whereas thoracolumbar involvement was common in patients with tuberculous spondylodiscitis. In line with the literature, the rates of paraspinal abscess and involvement at more than two segments were significantly higher in the tuberculous spondylodiscitis group. 21 In line with previous findings, the incidence of disc involvement was significantly higher in patients with pyogenic spondylodiscitis and elevated in patients with brucellar spondylodiscitis. 22 These radiological findings are extremely useful for differential diagnoses.
The incidence of spondylodiscitis has increased substantially, especially in the young population. Regardless of the presence of fever, pain in the affected area should be considered, especially in the presence of predisposing conditions, and it is necessary to raise awareness about spondylodiscitis among physicians. The requirement for invasive procedures and the high rate of culture negativity make the diagnosis of spondylodiscitis difficult. Meanwhile, clinical and radiological findings are useful for diagnoses. However, despite high rate of culture negativity, every effort should be made to identify the causative organism using invasive methods.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211060197 - Supplemental material for A disease that is difficult to diagnose and treat: evaluation of 343 spondylodiscitis cases
Supplemental material, sj-pdf-1-imr-10.1177_03000605211060197 for A disease that is difficult to diagnose and treat: evaluation of 343 spondylodiscitis cases by Safak Kaya, Sehmuz Kaya, Seyhmus Kavak and Senol Comoglu in Journal of International Medical Research
Footnotes
Authors’ contributions
Substantial contributions to the conception or design of the work or the acquisition, analysis, or interpretation of data: Seyhmus Kavak, Safak Kaya
Drafting the work or revising it critically for important intellectual content: Sehmuz Kaya, Senol Comoglu
Final approval of the version to be published: Sehmuz Kaya, Seyhmus Kavak, Senol Comoglu, Safak Kaya
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.