
Abstract
Objective
Cholecystostomy is a palliative treatment for patients unfit to undergo immediate cholecystectomy. Nevertheless, the role of cholecystostomy in the clinical management of such patients remains unclear. The Acute Physiology and Chronic Health Evaluation IV (APACHE IV) scoring system is useful for estimating the hospital mortality of high-risk patients. We evaluated the therapeutic effect of cholecystostomy by the APACHE IV scoring system in patients aged >65 years with acute cholecystitis.
Methods
In total, 597 patients aged >65 years with acute cholecystitis were retrospectively analyzed using APACHE IV scores.
Results
The fitness of the APACHE IV score prediction was good, with an area under the receiver operating characteristic curve of 0.894. The chi square independence test indicated that compared with conservative treatment, cholecystostomy may have different effects on mortality for patients whose estimated mortality rate was >10%. Comparison of the estimated mortality of patients before and after cholecystostomy indicated that the estimated mortality was significantly lower after than before puncture, both in the whole patient group and in the group with an estimated mortality of >10%.
Conclusion
The APACHE IV scoring system showed that cholecystostomy is a safe and effective treatment for elderly high-risk patients with acute cholecystitis.
Keywords
Background
Acute cholecystitis (AC) is a very heterogeneous disease, and its life-threatening potential is strongly determined by the general status of the patient. In the aging subpopulation with medical comorbidities, immediate definitive surgery may be hazardous. Percutaneous cholecystostomy (PC) offers an alternative method of management for patients unfit to undergo immediate cholecystectomy because of severe sepsis or other underlying comorbidities. 1 Lin et al. 2 reported that the rate of PC markedly increased from 0.5% in 2005 to 12.2% in 2015 and was more common among the elderly. Smith et al. 3 also reported increased use of PC in patients with AC over a 20-year period. Nevertheless, evidence for the role of gallbladder drainage as an effective alternative to early surgery remains poor, and few randomized controlled trials have focused on this issue.4,5 The Tokyo Guidelines 2018 state that early or urgent biliary drainage can significantly lower 30-day mortality in patients with grade II AC,6,7 but Lu et al. 8 reported that the mortality rates were far higher in patients undergoing PC than in patients undergoing cholecystectomy. Studies by Anderson et al.9,10 showed that cholecystostomy offered no survival benefit for patients with severe sepsis and shock and probably had increased risk of death. Determining the role of PC in the clinical management of high-risk surgical patients with AC remains difficult based on the currently available evidence. The World Society of Emergency Surgery recommends early laparoscopic cholecystectomy as the standard of care whenever possible, even in subgroups of patients who are considered fragile, such as the elderly. 11 Various definitions are used to identify “high-risk patients,” also making it more difficult to investigate the role of PC.
Outcome prediction is useful for therapeutic decision-making in critically ill patients. Acute Physiology and Chronic Health Evaluation IV (APACHE IV), the latest version of the APACHE scoring system published in 2006, was developed to estimate the hospital mortality for adult intensive care unit (ICU) admissions. The APACHE IV score consists of several parts, including diagnosis, chronic health status, age, vital signs, and physiologic measures such as blood gas analysis results, urine output, blood sugar level, white blood cell count, bilirubin level, and others; these are all not only accurate and reproducible but are also related to the prognosis of patients with AC, 12 especially elderly patients with AC. The present study was performed to evaluate the therapeutic effect of cholecystostomy by the APACHE IV scoring system in patients aged >65 years with AC. In this study, we defined high risk as an estimated mortality rate of >10%.
Methods
This study was approved by the ethics review board of Xuan Wu Hospital of Capital Medical University (Approval No. 862). All patients provided written informed consent. Consecutive patients admitted to our hospital (a 1200-bed urban tertiary-care referral center with a 12-bed surgical ICU) for the treatment of AC diagnosed by the Tokyo Guidelines diagnostic criteria 13 from January 2012 to December 2019 were retrospectively analyzed. All patients provided written consent to undergo the treatment protocol, and the authors did not have access to information that could identify individual participants during or after data collection. Our study focused on AC in general and not calculous AC. The diagnosis of AC was based on clinical symptoms (right upper quadrant or epigastric pain or tenderness), leukocytosis or an increased C-reactive protein level, and at least one of the following sonographic findings: distended gallbladder, gallbladder wall thickening of >3 mm, or debris in the gallbladder. 14 Patients who were admitted with AC were identified by International Classification of Diseases-9 diagnostic codes. The exclusion criteria were acute pancreatitis or choledocholithiasis; malignancy of the bile duct, gallbladder, liver, or pancreas; age of <65 years; and missing values that prevented calculation of the APACHE score. The data were collected from each patient on the day of admission or when necessary to compute the APACHE IV scores, and the worst value for each parameter in the first 24-hour period was used. Hospital mortality was defined as death before discharge from the hospital. The decision to perform PC or cholecystectomy was made by the hepatobiliary surgeons based on their experience and the patients’ will to undergo surgery.
PC was performed by a hepatobiliary surgeon who used ultrasound guidance under local anesthesia. First, a Chiba needle was transhepatically introduced into the gallbladder. Next, a guidewire was placed and the tract was sequentially dilated. A 7-Fr pigtail catheter was then positioned with its tip in the gallbladder. The PC catheter was left open, connected to a collection bag and drained by gravity. After 2 weeks, if the patient’s symptoms were relieved, the PC tube was clipped. Most patients who underwent PC retained the drainage tube, when was then removed during cholecystectomy; the other patients refused cholecystectomy, and the drainage tube was directly removed after a period of time. Conservative treatment mainly included antibiotic treatment, fasting, and nutritional support.
Statistical analysis
The reporting of this study conforms to the STROBE guidelines. 15 Data were analyzed using IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp., Armonk, NY, USA). Continuous variables are expressed as median and interquartile range, and categorical variables are expressed as frequency and percentage. The area under the receiver operating characteristic curve was used to compare the accuracy of the studied models. The rank sum test was used for intergroup comparisons, and P < 0.05 was considered statistically significant. We used the Hosmer–Lemeshow goodness-of-fit test to evaluate the calibration prediction fitness. The chi square independence test was performed to identify the relationship between mortality and the type of treatment of AC.
Results
In total, 862 consecutive patients with AC were enrolled in this study, of whom 265 patients were excluded because of choledocholithiasis (n = 124), acute pancreatitis (n = 108), cholangiocarcinoma (n = 5), gallbladder cancer (n = 3), and incomplete APACHE IV data (n = 25). Of the remaining 597 patients, the patients’ origins before admission were the emergency department (n = 521, 87.30%) and the inpatient units (n = 76, 12.70%). This study included 597 patients with a mean age of 75.88 years. Thirty patients died during hospitalization, resulting in a mortality rate of 5.03%. The 597 patients included 88 (14.75%) patients with American Society of Anesthesiologists (ASA) physical status class 1, 234 (39.20%) with ASA class 2, 192 (32.15%) with ASA class 3, 78 (13.07%) with ASA class 4, and 5 (0.83%) with ASA class 5. Because of local region conditions, many patients choose conservative treatment instead of emergency cholecystectomy or cholecystostomy. Among the 597 patients, 52 successfully underwent cholecystectomy within 72 hours of disease onset (2 died, 3.85%), 65 underwent ultrasound-guided PC within 7 days of disease onset (1 died, 1.54%), and 480 received conservative therapy (27 died, 5.63%). Of the 30 patients who died, 21 (70.00%) died of abdominal infection or sepsis, 4 (13.33%) died of pneumonia, 3 (10.00%) died of heart disease, and 2 (6.67%) died of cerebrovascular disease. Cholecystectomy was carried out according to conventional methods; 94.3% procedures were performed by laparoscopy, 5.7% procedures were performed by laparotomy, and no patients underwent subtotal cholecystectomy. Dislodged drainage tubes were found in two (3.08%) patients in the PC group without signs of bile leakage, and two (3.08%) cases of bleeding after PC were cured by conservative treatment. No other procedure-related complications occurred in the PC or cholecystectomy group. Fifty-four (84.38%) of the 64 survivors in the PC group underwent cholecystectomy approximately 60 days after cholecystostomy, 7 (10.94%) survivors only underwent drainage tube removal approximately 30 days after cholecystostomy, and the remaining 3 (4.68%) survivors maintained their drainage tube for >180 days, after which time it was removed and no cholecystectomy was performed. No obvious complications occurred among the 54 patients who underwent cholecystectomy after PC, and none of the other 10 patients died of gallbladder-related disease. The 1-year recurrence rate in the nonsurgical treatment group was about 28.98%.
A comparison of the patients’ characteristics between survivors and nonsurvivors is shown in Table 1. Many of the patients’ details, including the leukocyte count, transaminase level, bilirubin level, blood gas analysis results, and other indices are included in the APACHE IV score; therefore, we have not listed them in detail. The survivors were younger and had lower APACHE IV scores and lower risks of death than the nonsurvivors. The discrimination of the APACHE IV score prediction was good, with an area under the curve of 0.894 (95% confidence interval, 0.849–0.930) (Figure 1). The Youden index was 0.62, the sensitivity was 78.26%, the specificity was 83.33%, the positive predictive value was 19.57%, and the negative predictive value was 98.63%. The APACHE IV models were well-calibrated (with Hosmer–Lemeshow statistic: chi-square = 8.179, eight degrees of freedom); these data are shown in Figure 2. The average cost of conservative treatment for AC was 1303 US dollars, the average cost of PC was 1779 US dollars, and the average cost of cholecystectomy was 3320 US dollars (Figure 3).
Comparison of survivors and nonsurvivors with acute cholecystitis aged >65 years.

Data are presented as median (interquartile range).

Receiver operating characteristic curve for the APACHE IV score of the overall patients. The area under the curve was 0.878 (95% confidence interval, 0.780–0.932).
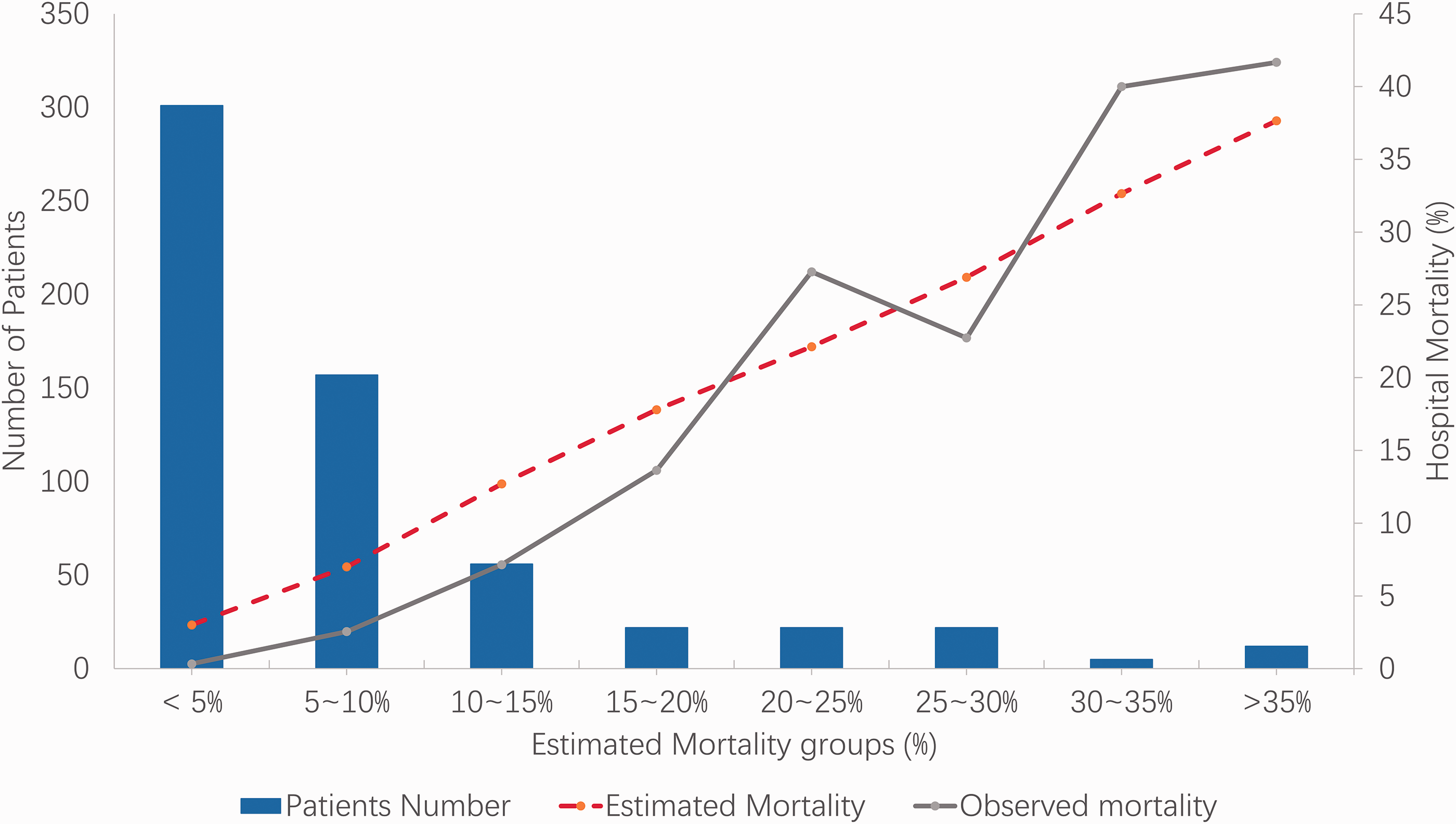
Calibration curve of APACHE IV models for all 597 patients. The numbers of patients in each group are shown in the columns, and the actual mortality rate and estimated mortality rate of each group are shown as solid and broken lines, respectively. The degree of fit is good (Hosmer–Lemeshow statistic).

Average treatment cost of various treatments for acute cholecystitis.
Using the chi square independence test for all patients (n = 597), we found that the two surgical treatments (cholecystectomy and PC) had no statistically significant effects on mortality. Because death is a serious event, we chose various levels of estimated mortality to further examine our data; the details are shown in Table 2. When the estimated mortality rate was >10% or >12.5% compared with conservative treatment, PC may have had different effects on mortality; however, cholecystectomy did not show a difference. Comparison of the estimated mortality of patients before and after PC indicated that the estimated mortality was significantly lower after than before puncture, both in the whole patient group (P = 0.002) and in the group with an estimated mortality of >10% (P = 0.001). These details are shown in Table 3.
Effect of cholecystectomy or cholecystostomy on different estimated mortality groups compared with conservative treatment.
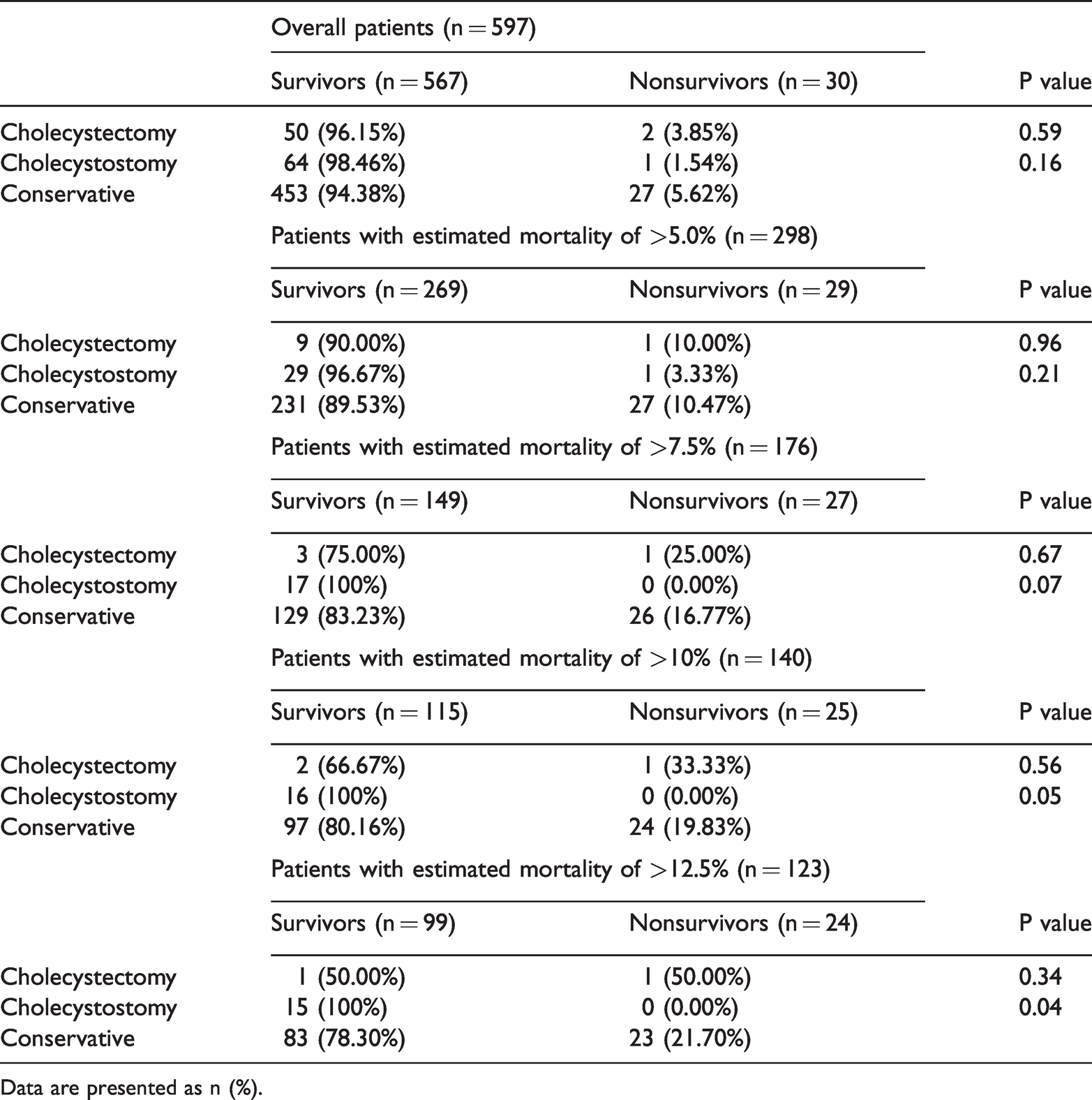
Data are presented as n (%).
Comparison of estimated mortality of patients before and after cholecystostomy.

Data are presented as median (interquartile range).
Discussion
As the prevalence of AC increases with the growing elderly population, we are paying more attention to older patients with AC. One of the main problems concerning the role of PC is the lack of validated, well-established scoring systems to stratify the severity of patient disease states; additionally, different definitions are used to identify “high-risk” patients. The authors of the Tokyo Guidelines suggest a staging system of mild, moderate, and severe depending upon the degree of local inflammation and the patients’ conditions,16–18 but the diagnostic criteria of these three levels are not continuous. A retrospective series failed to confirm a significant benefit of the application of the Tokyo Guidelines. 19 Amirthalingam et al. 20 concluded that the Tokyo Guidelines 2013 may be too restrictive for patients with moderate and severe AC and that more attention should be paid to patient comorbidities during clinical decision-making. Yacoub et al. 21 attempted to develop a score to stratify patients with gangrenous cholecystitis but did not pay much attention to the patients’ comorbidities; their score cannot be applied to patients who do not desire surgery. We believe that it is beneficial to supplement the three Tokyo Guideline levels with other grading standards. We propose the APACHE IV score as an effective tool to stratify and compare elderly patients with AC in clinical trials, and our study results indicate that this is possible 12 because the APACHE IV score prediction was good with an area under the curve of 0.894. Most hospitals. have no conditions or data to establish their own evaluation criteria; therefore, it is convenient and accurate to apply APACHE IV scoring in their clinical wards.
In a randomized controlled trial by Hatzidakis et al., 22 the efficacy of PC was compared with that of conservative management. The authors suggested that PC should not be performed as the first choice in patients with AC because it did not produce lower mortality rates than did conservative treatment. They also suggested that PC should be appealing to patients who do not show clinical improvement following 3 days of conservative treatment, as well as to critically ill ICU patients. 22 Their results are consistent with ours. For patients with mild or moderate AC with an estimated mortality rate of <10%, we found that there was no significant difference in the effect of PC and conservative treatment on mortality. One reason for the indistinguishability is that the death rates were very low; additionally, conservative treatment had a good effect. We suggest more precise indications for PC when the estimated mortality rate is >10%. Among these eligible patients, our data showed that cholecystostomy may have different effects on mortality than conservative treatment (P = 0.05), and the estimated mortality after puncture was significantly decreased (P = 0.001). Early recognition and intervention are required in these patients because of the rapid progression of AC to gangrene and perforation.
Although laparoscopic cholecystectomy is considered the gold standard treatment for patients with AC, it remains difficult to make definitive recommendations regarding treatment by PC or cholecystectomy in elderly or critically ill patients. The benefit of PC over cholecystectomy in the management of critically ill patients with AC could not be proven in a systematic review involving 337,500 patients. 23 Another review involved a particularly detailed examination of 53 papers regarding cholecystostomy as an option in AC and suggested that PC was beneficial in high-risk patient groups, predominantly as a bridging therapy, allowing safer elective cholecystectomy once the patient had recovered from the acute illness. 24 Our data agree with this suggestion in that the procedure can stabilize the patient so that appropriate therapeutic planning can be achieved. Because the number of patients with high predicted mortality in both the PC group and cholecystectomy group was too small in our study, the comparison between the two treatments would not have been statistically accurate. More data are required to clarify this issue.
In previous studies of the safety of PC, the rate of procedure-related complications was only about 6.25%. This is relatively low considering that candidates for PC are usually high-risk patients. In our study, the rate of procedure-related complications in elderly patients with AC was only 6.15%, which is comparable with the rate in previous reports. 25 Although urgent cholecystectomy (within 72 hours from symptom onset) has been proposed as a definitive treatment for symptomatic gallbladder disease, 26 routine cholecystectomy in an emergency setting can be challenging. Rather, gallbladder puncture is a better choice for surgeons with less experience. PC is a comparatively safe and effective procedure for the treatment of not only elderly high-risk patients with serious comorbidities but also patients with contraindications for the general anesthesia required for cholecystectomy. 27
Our study has some major limitations. First, it was a nonrandomized and retrospective study. Second, this research was performed in a local geographical region. Among the 597 patients, 480 (80.40%) underwent conservative management rather than the surgical management that they should have received according to the international guidelines. This was mainly due to the patients’ unwillingness to undergo surgery and the lack of experienced surgeons, and this situation may have impacted the patients’ prognosis. The relatively small number of patients undergoing cholecystectomy or cholecystostomy may have impacted the credibility of the results. Third, the decision to perform cholecystectomy or cholecystostomy was simply up to the surgeons, resulting in selection bias. The study’s external validity is also limited, and its purpose was to compare PC with conservative treatment, excluding patients who underwent cholecystectomy. Further studies will be required to elucidate this point. Fourth, the APACHE IV score provides a picture of “physiological stress” at the moment of diagnosis; nevertheless, in fragile patients aged >65 years, many confounding factors probably affect the results. The same age, same physiological parameters, and same recent diseases can be associated with very different mortality rates. In future research, greater numbers of parameters and more accurate algorithms may be needed to improve the accuracy of prediction.
Conclusion
The APACHE IV scoring system showed that cholecystostomy was a safe and effective treatment for AC in elderly patients with an estimated mortality rate of >10%, but cholecystostomy cannot be elevated to the gold standard treatment.