
Abstract
Osteochondromas are common in the long bones and relatively rare in the head and neck regions. We herein report a case of a solitary temporal bone osteochondroma associated with a functional pituitary adenoma hypersecreting prolactin. The patient was a 48-year-old man with progressive, painless temporal swelling associated with gradual visual loss, gynaecomastia, erectile dysfunction, and loss of libido. A brain computed tomography scan with bone windows showed right temporal sessile bony expansion and a pituitary tumour. A pituitary function test revealed hyperprolactinaemia. His symptoms resolved with medical management, and excisional biopsy of the temporal tumour confirmed an osteochondroma. To the best of our knowledge, this is the first reported case of a solitary temporal bone osteochondroma with a functional pituitary adenoma hypersecreting prolactin.
Keywords
Introduction
An osteochondroma is a benign tumour composed of mature hyaline cartilage with focal ossification. It is the most common benign bone tumour, accounting for 20% to 50% of benign bone tumours and 9% of all bone tumours.1,2 About 85% of patients have solitary tumours, while approximately 15% have multiple tumours. 3 Multiple osteochondromas develop in the setting of hereditary multiple osteochondromas (HMO), which is a rare genetic disorder with autosomal dominant inheritance. 4 Most patients with HMO have a positive family history, and 90% have mutations in either the EXT1 or EXT2 gene.5,6
Osteochondromas commonly affect the axial skeleton, especially the epiphyses of long bones such as the distal femur, proximal tibia, and proximal humerus. 7 Very rarely, they may affect the skull, carpus, tarsus, patella, sternum, or vertebrae. 8 Craniofacial osteochondromas are very rare, and most occur in the mandibular region.9,10 Only one case of temporal bone osteochondroma has been reported in the English-language literature to date. 10
The major concerns regarding osteochondromas are cosmesis and impingement on local structures such as peripheral nerves, blood vessels, and tendons, thereby leading to symptomatology.4,11 The presence of cortical and medullary continuity with the parent bone and a cartilaginous cap are two pathognomonic features that define osteochondromas.12,13 However, there is a low risk of malignant transformation that is more common with HMO than solitary osteochondromas.3,6–8,13 Whereas solitary osteochondromas are nonsyndromic and have. yet to be linked with any disease, HMO have been associated with endocrine diseases. Galasso et al. 14 described a patient with HMO who developed partial growth hormone deficiency that was treated for 4 years, and Bozzola et al. 15 described two patients with osteochondromas (one with a solitary osteochondroma and one with HMO) associated with growth hormone deficiencies. Growth hormone replacement therapy was discontinued because of a poor linear growth response and a moderate increase in the size of the exostoses. However, the diagnosis of growth hormone deficiency was not confirmed by a third test.15,16 Remde et al. 17 reported a case of HMO in a patient with an abnormal multiple endocrine neoplasia type 1 gene who presented with hyperparathyroidism and a nonfunctional pituitary adenoma. In the present report, we describe a patient with an osteochondroma located in the temporal skull bone and a concurrent functional pituitary adenoma.
Case presentation
A 48-year-old man presented with a 3-year history of progressive, painless right-sided skull swelling for which he had social and cosmetic concerns. Three months prior to presentation, he had developed right-sided facial deviation, progressive bilateral visual loss, gynaecomastia, erectile dysfunction, and loss of libido.
Brain computed tomography showed a hyperdense sessile expansion of the right temporal bone, a hyperdense intrasellar tumour with suprasellar extension associated with moderate heterogeneous contrast enhancement, and the snowman sign (Figure 1). A pituitary function test showed hyperprolactinaemia of 374 ng/mL. Diagnoses of a functional pituitary adenoma and a temporal bone tumour were made.

Cranial computed tomography scan showing temporal bone osteochondroma (thick arrow) and pituitary tumour (thin arrow).
The patient underwent medical treatment with a bromocriptine analogue (Parlodel), which resulted in remarkable improvement of his symptoms. However, he consented to surgical removal of the temporal skull tumour because of social and cosmetic concerns. He underwent an excisional biopsy with intraoperative findings of a sessile bony lesion continuous with the underlying temporal bone; the lesion measured 3 × 3 cm with no intracranial extension. The patient’s preoperative temporal swelling and postoperative tumour specimen are shown in Figure 2. Histopathological examination of the specimen (Figure 3) showed osteochondroma with a thin cartilage cap on the surface and the appearance of a disorganized growth plate. The cortex of the lesion merged with the cortex of the temporal bone, and cartilage islands were scattered throughout the underlying trabecular bone. The patient was followed up for 1 year; however, further neuroimaging could not be performed thereafter because the patient was lost to follow-up. The reporting of this study conforms to the CARE guidelines. 18

(a) Preoperative photograph showing temporal swelling. (b) Postoperative specimen showing sessile osteochondroma.
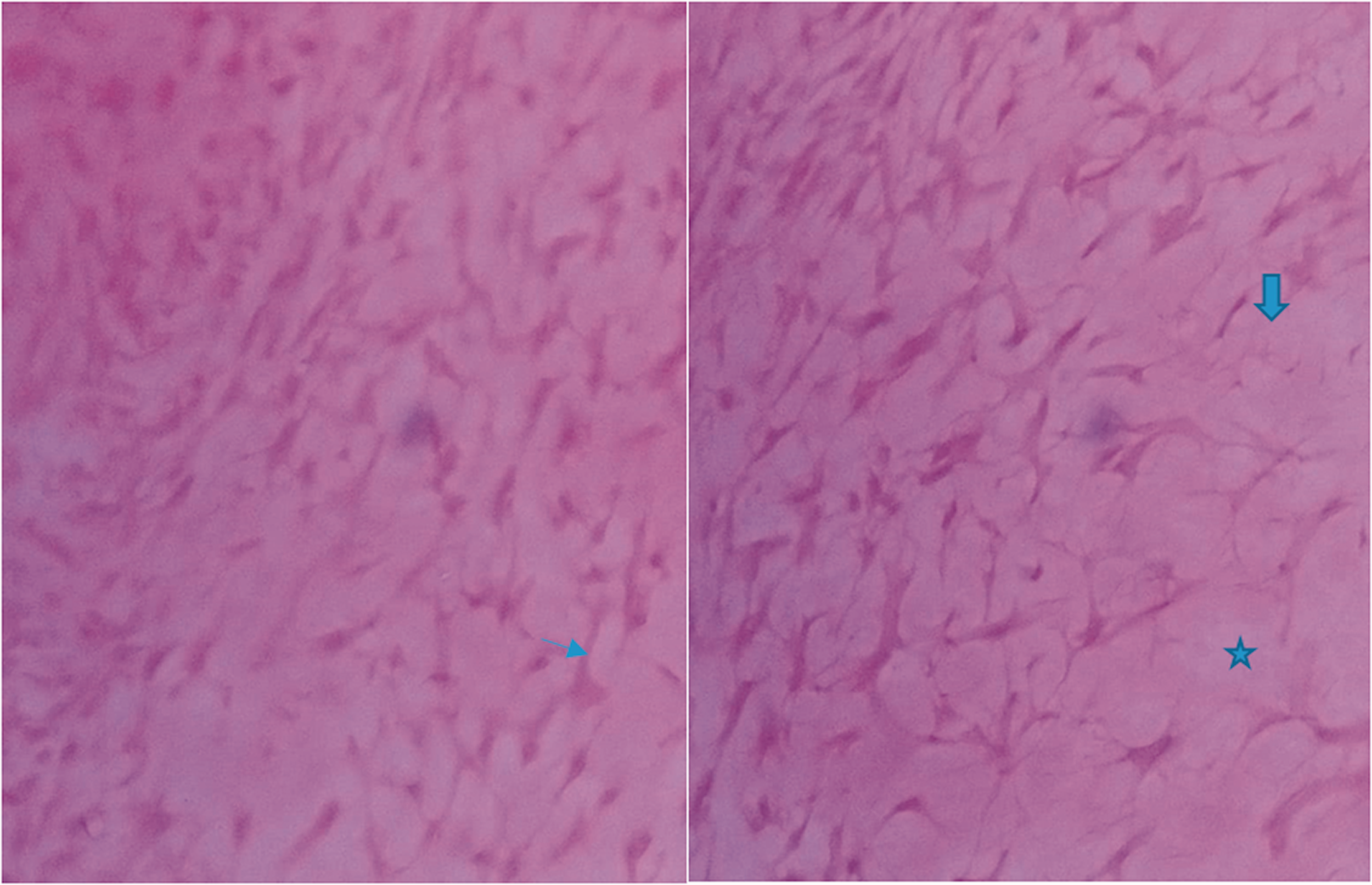
Histopathological photomicrograph showing the tumour with bone marrow (thick arrow), trabecular bone (thin arrow), and benign hyaline cartilaginous cap (asterisk).
Discussion
According to the World Health Organization classification of tumours, osteochondromas are cartilage-capped bony projections on the external surfaces of bones with marrow cavities that are continuous with those of the underlying bones. 8
The reported incidence of osteochondroma is 8% of all bone tumours, but this is likely an underestimation because most osteochondromas are asymptomatic. 19 A large series comprising patients who underwent detailed radiographic evaluations and examinations of pathologic specimens showed a prevalence of 4.4 per 1000 (0.44%). 8 That study involved assessment of a large osteological collection to estimate the prevalence of osteochondromas. 8 However, the true prevalence of osteochondromas remains unknown because many of these lesions are discovered incidentally. 20
Osteochondromas are usually seen in the axial skeleton, especially the metaphysis of long bones; they are rarely seen in the head and neck region. 10 Most cases seen in the head and neck region are located in the mandible. 10 Osteosarcomas are rarely found in the jaw, skull base, and cavarium.9,10,21
Osteochondromas are asymptomatic in most cases and are usually diagnosed incidentally on radiographs obtained for other reasons.1,20,22 However, they can present as a painless palpable mass on the involved bone, and patients sometimes have cosmetic concerns. 12 Our patient presented with a painless right temporal swelling, resulting in both social and cosmetic concerns. Symptoms of osteochondromas are caused by compression, fracture, bursitis, or malignant transformation. 23 Peripheral nerve compression can lead to numbness and tingling sensation in a limb. 24 Spinal osteochondroma may cause kyphosis or spondylolisthesis. 25 However, cord compression is a rare phenomenon because most osteochondromas develop outside the spinal cord. 26 Head and neck osteochondromas are associated with facial asymmetry and masseter dysfunction.27,28 The most feared complication of osteochondroma is malignant transformation, which leads to secondary chondrosarcoma. 29 Malignant transformation is estimated to occur in approximately 1% of solitary osteochondromas and 10% of HMO.1,3 Rarely, other malignant tumours such as osteosarcoma can complicate an osteochondroma. 30
Osteochondromas are usually diagnosed by plain radiographs. The key radiological features are cortical and marrow continuity between the lesion and the parent bone and the presence of a cartilage cap. 13 However, lesions located at complex anatomical regions like the shoulder girdle, pelvis, or spine can be studied by computed tomography or magnetic resonance imaging. 31
Osteochondromas commonly occur in people aged 10 to 30 years; however, our patient presented at 45 years of age.8,32 Osteochondromas can either be sessile or pedunculated. Pedunculated osteochondromas are the most common type, and this is the type that was seen in our patient (Figure 2).4,32,33 Osteochondromas are either solitary or multiple. Whereas solitary osteochondromas are the most common type and are usually nonsyndromic, multiple osteochondroma variants (although rare) are often part of HMO syndrome, seen in approximately 15% of patients with osteochondromas.34,35 HMO syndromes are autosomal dominant bone disorders characterized by multiple benign cartilage-capped tumours. 17 Two genes (EXT1 (65%) and EXT2 (35%)) are responsible for causing HMO. 13 Mutation of these genes leads to deficiency of heparin sulfate biosynthesis and irregular diffusion patterns of Indian hedgehog homolog, which plays a major role in endochondral ossification, and hence to abnormal chondrocyte polarization and proliferation. 17 In addition to HMO syndrome, osteochondromas have been reported in patients with endocrine abnormalities. Remde et al. 17 reported HMO involving the long bones in a patient with multiple endocrine neoplasia type 1. This patient had a parathyroid adenoma and nonfunctional pituitary tumour. Bozzola et al. 15 described a patient with HMO and growth hormone deficiency. In this report, we presented a patient with a histologically confirmed solitary osteochondroma of the temporal bone with a functional pituitary adenoma hypersecreting prolactin. To our knowledge, this is the first report of a solitary osteochondroma of the head and neck region in a patient with a functional pituitary tumour.
Osteochondromas can be complicated by deformities, functional limitations, compression of neurovascular bundles, and malignant transformation to secondary osteochondrosarcoma. 15 Our patient presented for treatment because of psychosocial embarrassment along with functional and pressure symptoms of the pituitary tumour.
Conclusion
We have presented a case involving a 48-year-old man with a solitary syndromic temporal osteochondroma associated with a prolactinoma. To the best of our knowledge, this is the first reported case of a syndromic solitary temporal bone osteochondroma associated with a functional pituitary adenoma hypersecreting prolactin.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211058860 - Supplemental material for Unusual location of osteochondroma in the temporal region in a patient with functional pituitary adenoma
Supplemental material, sj-pdf-1-imr-10.1177_03000605211058860 for Unusual location of osteochondroma in the temporal region in a patient with functional pituitary adenoma by Henry Olayere Obanife, Akaba Kingsley, John Ashindointiang, Joseph Asuquo, Olabisi Ogunleye and Iwasam E. Joshua in Journal of International Medical Research
Footnotes
Consent for publication
The patient provided both verbal and written informed consent for the reporting of this case and all accompanying images.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics approval
The requirement for ethics approval was waived because this study was a case report of a patient managed by our team, not an interventional study (i.e., no intervention or experimentation was carried out on the patient for the purpose of the study).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.