
Abstract
Objective
The present study aimed to investigate the recent trends in Helicobacter pylori infection associated with peptic ulcer disease in a large population in Shanghai.
Methods
We analyzed the medical records of all patients who had undergone upper gastrointestinal endoscopy (EGD) for uninvestigated dyspepsia at Ren Ji Hospital between 2013 and 2019 to determine the prevalence of H. pylori infection in patients with peptic ulcers.
Results
Peptic ulcers were found in 40,385 of the 383,413 patients who underwent EGD during the study period. Over the 7-year study period, the annual prevalence of H. pylori among patients receiving EGD declined from 32.2% to 26.5%. H. pylori was present in 60% of ulcers and the incidence was higher (66.9%) in duodenal compared with gastric ulcers (48.5%). The proportion of H. pylori-associated gastric ulcers declined from 52.2% to 49.3% and that of H. pylori-positive duodenal ulcers declined from 70.0% to 63.9%.
Conclusion
The prevalence of H. pylori-positive peptic ulcers, mainly duodenal ulcers, fell from 2013 to 2019. However, the proportion of non-H. pylori-associated peptic ulcer disease increased, especially in elderly people, possibly due to the use of nonsteroidal anti-inflammatory drugs. Further research is needed to confirm this hypothesis.
Keywords
Introduction
Peptic ulcer disease (PUD), including gastric and duodenal ulcers, is a major health burden in China. The reported prevalence of PUD in Western countries ranges from 0.1% to 4.7%, with an annual incidence of 0.19% to 0.3%. 1 The prevalence of PUD in many countries has decreased markedly since the discovery of Helicobacter pylori in the 1980s.1,2 However, the prevalence of PUD in Shanghai is substantially greater than that in Western populations, with a reported prevalence of endoscopically confirmed PUD as high as 17%3,4 in a random population.
The two most common causes of peptic ulcers are currently H. pylori infection and the use of gastrotoxic medications, primarily nonsteroidal anti-inflammatory drugs (NSAIDs). H. pylori was discovered in 1982, 5 when it was estimated to be responsible for up to 90% of duodenal ulcers and 70% of gastric ulcers. 6 However, recent studies have reported a decline in the prevalence of H. pylori in patients with PUD to 36% to 73%, depending on ethnicity, geographic location, and socioeconomic factors. 7 The increasing use of NSAIDs, including aspirin, is thought to responsible for most non-H. pylori ulcers. 8 The prevalence of H. pylori infection has fallen markedly in most developed countries and is also declining in developing countries in line with improving socioeconomic conditions and sanitation.9–11 However, a study in 2010 reported that more than half of the population was infected in Shanghai, where the population consists of urban residents and an influx of people from the country who are likely to have a higher rate of H. pylori infection. 3 The aim of this study was to investigate the changes in prevalence of H. pylori infection in patients in Shanghai undergoing endoscopy for uninvestigated dyspepsia, who had an endoscopically confirmed peptic ulcer over the 7-year period from 2013 to 2019.
Methods
Subjects and study design
This was a cross-sectional single-center retrospective study conducted at Ren Ji Hospital, Shanghai Jiao Tong University School of Medicine. The reporting of this study conforms to the STROBE statement. 12 We retrieved the medical records of all patients who had undergone upper gastrointestinal endoscopy (EGD) because of uninvestigated dyspepsia from 1 January 2013 through to 31 December 2019. All medical records with information on demographic features, H. pylori status, and pathological and endoscopic findings were stored prospectively in an electronic database at our center. The current study analyzed the above data by reviewing existing records, and there was no direct contact with the participants. No identifiable individual information was used and patient records were removed before being included in the analysis. For the above reasons, the research protocol did not require informed consent from the participants. The study was approved by the Ethics Committee of Shanghai Renji Hospital (approval number: KY2020-155).
Exclusion criteria
Patients who underwent upper endoscopy for reasons other than uninvestigated dyspepsia, such as cirrhosis follow-up, major systemic diseases, or other indications, were excluded. Patients without biopsies or with unknown H. pylori status and acute ulcer bleeding were also excluded. For patients who underwent multiple EGDs within the study period, only the first results were included.
Diagnostic methods and H. pylori status
A peptic ulcer was defined as a >5-mm diameter mucosal break with depth in the stomach and/or duodenum, detected by EGD. Gastric mucosal biopsies were routinely taken for histologic analysis unless contraindicated. At least three biopsy specimens from the antrum and/or corpus were taken during each endoscopy. One biopsy was used for the rapid urease test to detect H. pylori and the others were analyzed histologically. Biopsy specimens were fixed immediately in 10% formalin and then processed in accordance with standard sectioning and staining procedures. The morphology was evaluated by two gastroenterologists. Stomach biopsies were performed according to the updated Sydney System. 13 In patients with both gastric and duodenal ulcers, we counted both separately.
H. pylori infection was diagnosed by a positive urease test and/or the presence of H. pylori on histological examination of gastric biopsies.
Statistical analysis
We analyzed the prevalence of H. pylori infection among the entire study population and examined the prevalence of peptic ulcers across the population grouped by age, sex, and H. pylori status. We compared the prevalence of H. pylori-positive PUD between men and women using χ2 tests. Patients with and without peptic ulcer were compared by univariate analysis. The effects of individual risk factors on the occurrence of gastric or duodenal ulcers were tested by odds ratios (OR) and 95% confidence intervals (CI). CI values that did not include unity were considered significant. The significance of trends during the study period or among age groups was tested by linear regression analysis. Significance was defined as P < 0.05.
Results
The study population consisted of 383,413 patients who underwent EGD because of uninvestigated dyspepsia from 2013 to 2019. Gastric or duodenal ulcers were found in 10.5% of cases (40,385 of 383,413), including 15,114 patients with a gastric ulcer and 25,271 with a duodenal ulcer. The ulcer type and sex in relation to H. pylori infection status are shown in Table 1. The overall mean H. pylori-infection rate among the patients with ulcers was 60.0% (95%CI 59.5%–60.5%). As noted in prior studies,14,15 the prevalence of H. pylori infection was significantly higher among patients with duodenal compared with gastric ulcers (P < 0.0001). The overall sex ratio (male:female) for patients with PUD was 2.02:1 (gastric ulcer: 2.30; duodenal ulcer: 1.87; all P < 0.0001).
Characteristics and clinical data of patients with peptic ulcers.

GU, gastric ulcer; DU, duodenal ulcer.
The prevalences of H. pylori-positive gastric and duodenal ulcers grouped by sex are shown in Figure 1. The prevalences of both H. pylori-positive gastric and duodenal ulcers were higher in men than in women (P < 0.0001; Figure 1a). The fractions of H. pylori-positive gastric and duodenal ulcers were also higher in men than in women (P < 0.0001 and P = 0.0158, respectively), with a more obvious sex difference for gastric compared with duodenal ulcers (Figure 1b).

a. Prevalence of H. pylori-positive peptic ulcers grouped by sex. b. Fraction of H. pylori-positive ulcers grouped by sex.
The trends for gastric and duodenal ulcers and for H. pylori infection according to year of diagnosis and age are shown in Figure 2. There were a significant downward trends in the fractions of H. pylori-positive gastric and duodenal ulcers from 2013 to 2019 (gastric ulcer: r2 = 0.664, P = 0.0257; duodenal ulcer: r2 = 0.918, P = 0.0002) (Figure 2b). The rise and fall in age-related H. pylori infection did not match the rise in age-related gastric ulcers and fall in age-related duodenal ulcers. The H. pylori infection rate was highest in the 24- to 33-year age group but the age-related trend was not significant. Gastric ulcers showed an age-related rise (r2 = 0.8039, P = 0.0026) and duodenal ulcers showed an age-related fall (r2 = 0.817, P = 0.0021) (Figure 2c). The prevalences of H. pylori-positive gastric and duodenal ulcers also decreased significantly with age (gastric ulcer: r2 = 0.689, P = 0.0108; duodenal ulcer: r2 = 0.918, P = 0.0002) (Figure 2d).
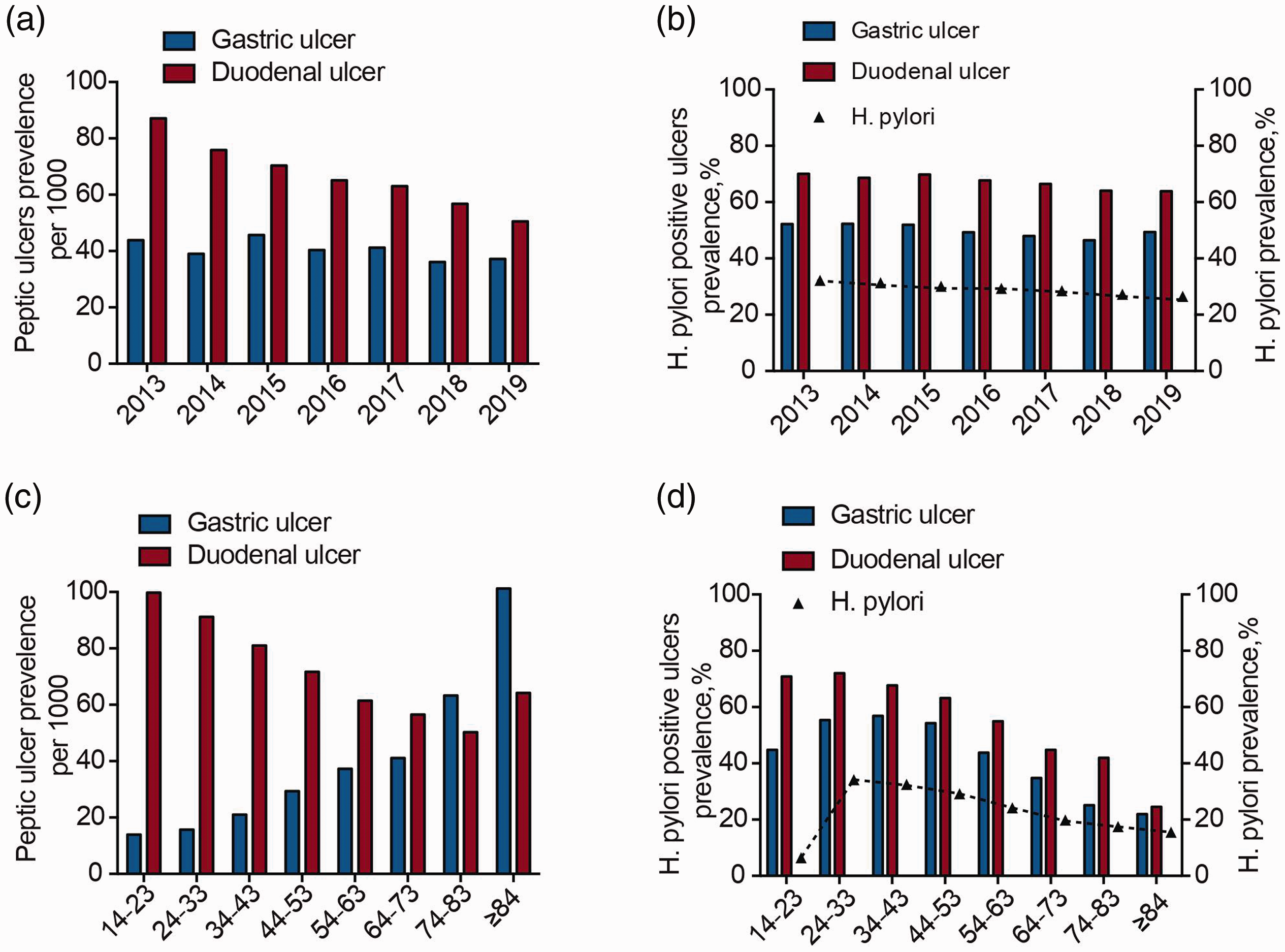
a. Prevalence of peptic ulcers according to year of diagnosis. b. Trends in fraction of Helicobacter pylori-positive peptic ulcers according to year of diagnosis. c. Trends in peptic ulcer prevalence grouped by age. d. Trends in fraction of H. pylori-positive peptic ulcers grouped by age.
Table 2 shows the results of univariate analysis of the effects of H. pylori and sex on the incidences of gastric and duodenal ulcers. As expected, there were significant differences between H. pylori-positive and H. pylori-negative patients according to univariate analysis. Men had significantly higher risks of both gastric ulcers (OR = 3.12, 95% CI 3.01–3.24) and duodenal ulcers (OR = 2.54, 95% CI 2.48–2.61).
Peptic ulcer risk in relation to sex and Helicobacter pylori status.

GU, gastric ulcer; DU, duodenal ulcer; OR, odds ratio; CI, confidence interval.
Discussion
The current study showed that the prevalence of H. pylori-positive PUD decreased significantly in Shanghai from 2013 to 2019. This was most likely secondary to a decline in H. pylori infections, which fell from 32.2% to 26.5% among patients with uninvestigated dyspepsia in our study, due to eradication treatment and improved hygiene. The prevalence of H. pylori was greater in duodenal compared with gastric ulcers and higher in male than in female patients. H. pylori infection contributed to >65% of duodenal and approximately 48% of gastric ulcers in the current study. However, unlike duodenal ulcers, there was no significant reduction in the prevalence of gastric ulcers over the 7-year study period, despite a decreasing trend in H. pylori infection rates in this area. 16 The proportion of non-H. pylori associated PUD obviously increased, especially in elderly people, and NSAIDs use is thought to be a major risk factor for non-H. pylori-associated PUD, especially gastric ulcers, in this population.17,18 H. pylori infection and NSAIDs have been considered to independently and significantly increase the relative risk of PUD. 8 Our data suggest that NSAIDs may account for a large percentage of cases of PUD.
Li et al. 3 carried out a population-based endoscopic study in Shanghai and reported a prevalence of PUD of 17.2% (gastric ulcer: 6.1%; duodenal ulcer: 13.3%), with positive H. pylori serology tests in 73.3% of the total Shanghai sample and H. pylori infection in 92.6% of PUD cases. The average H. pylori infection rate in the current study was 60% in patients with peptic ulcers (48.5% in gastric ulcer and 66.9% in duodenal ulcer). The difference in H. pylori infection rates in patients with PUD between the two studies may be due to the different methods used to confirm H. pylori infection. In addition, the present study was a retrospective study with a long time span and a large sample size compared with the previous prospective study. However, it should be noted that a high rate of H. pylori infection does not necessarily equate to a high incidence of PUD. For example, Indians in Malaysia have a high prevalence of H. pylori infection (36%) but a relatively low incidence of ulcers, while Chinese individuals have a lower prevalence of H. pylori (29%) but a higher incidence of ulcers. 19 It is also possible that Chinese populations may have a higher prevalence of more-ulcerogenic strains of H. pylori, such as strains including the duodenal ulcer-promoting (dupA) gene, which has been reported to be associated with duodenal ulcer development.20,21
The clinical implications of H. pylori infection have gradually been recognized since its first description in 1984. 22 Infection mainly occurs during childhood, commonly before 5 years of age, with the infection rate reflecting hygiene and sanitation. The H. pylori-infection rate among young people (age 14–23) in our study was low, which may reflect health and economic developments in China in the past 10 to 20 years. The change in prevalence of H. pylori with increasing age in our study may be due to specific treatment or to the use of antibiotics for other reasons. In contrast to the age-related increase in the incidence of gastric ulcers, the incidence of duodenal ulcers fell with age, which could be explained by the use of proton pump inhibitors and antibiotics for the management of peptic ulcer disease and the fact that older people are more likely to be exposed to NSAIDs. Our study also showed that the prevalence of H. pylori-positive PUD in Shanghai was significantly higher in men than in women, consistent with the results of many previous surveys.23,24 This may be due to differences in hormone secretion between men and women affecting gastric emptying and bacterial load; however, further studies are needed to investigate this possibility. The increased risk of H. pylori in men may also be associated with increased smoking and different social, living, and eating habits compared with women. 25
This study had some potential limitations. We did not assess the use of low-dose acetylsalicylic acid or NSAIDs, which may have affected the incidence of PUD. 26 Similarly, there was no information on the use of antibiotics for H. pylori infection or acid suppression therapy before EGD.
In conclusion, the prevalence of H. pylori-positive PUD, especially duodenal ulcers, decreased from 2013 to 2019, presumably in association with a decreasing trend in the prevalence of H. pylori infection. H. pylori-positive PUD now accounts for about 60% of all ulcers, indicating that 40% of ulcers are unrelated to H. pylori. This could provide evidence to support the prevention and treatment of PUD, but further studies are needed.
Footnotes
Acknowledgements
The authors would like to thank Professor David Y. Graham for helpful discussions on topics related to this work.
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Hong Lu is a consultant for Takeda and Astra Zeneca for proton pump inhibitors in relation to H. pylori infection treatment. Other authors declare no competing interests.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was supported by a grant from the National Natural Science Foundation of China [grant number 81800502].