
Abstract
Objective
To analyze recovery from dizziness in patients with acute vestibular neuritis (AVN) after applying the “Dizziness & Fall Risk Assessment and Intervention (DFRAI)”.
Methods
This prospective study involved patients with AVN who underwent a survey of dizziness and fall risk. The patients received medical treatment and customized vestibular rehabilitation, and vestibular function was evaluated at the initial attack and 3 months later.
Results
Forty-one patients underwent subjective questionnaire assessments, which showed significant improvement in visual analog scale-dizziness handicap inventory-fear of falling (VAS-DHI-FOF) results from the initial vertigo attack to 3 months later. In the sensory organization test (SOT), the initial composite score was 63 ± 13.1, which improved to 77.5 ± 4.9 3 months later. In caloric testing, the canal paresis (CP) score was 42.9 ± 35.2, which improved to 29.9 ± 23.5 3 months later.
Conclusions
Subjective improvement in dizziness and objective recovery of vestibular function were confirmed. DFRAI is a comprehensive solution for dizziness, and appropriate application of the DFRAI is expected to have a positive effect on recovery from dizziness and fall prevention in patients with AVN.
Keywords
Introduction
Dizziness is characterized by various abnormal sensations related to the perception of the body's relationship to space and is a frequent occurrence in elderly people. 1 Approximately 30% of elderly patients experience a balance disorder. 2 Classically, four subtypes of dizziness have been described: vertigo, pre-syncope, disequilibrium, and lightheadedness.1,3,4 In an aging society, dizziness is one of the most common reasons for visits to a doctor or hospitalization. Elderly people with vertigo and dizziness require both vestibular diagnosis and vestibular rehabilitation, 5 and they may also require education for fall prevention and assessment of their home environment.1,6,7 The causes of dizziness are multifactorial, and physicians should attempt to evaluate the degree of dizziness using multiple methods, such as the Dizziness Handicap Inventory (DHI), visual analog scale (VAS), and assessment of the fear of falling (FOF).1,8
Hospitalized patients with dizziness, such as those with acute vestibular neuritis (AVN), require a new treatment strategy that addresses the entire course of the disease causing the dizziness, including subjective/objective vestibular surveys, fall prevention, rehabilitation exercises, home environment intervention, and dizziness control using various drugs.4,5,9
This study presented a potential therapeutic system named “Dizziness & Fall Risk Assessment and Intervention (DFRAI)” and aimed to analyze the recovery pattern of dizziness in patients with AVN after applying the DFRAI. 9 The authors also aimed to validate the positive effect of DFRAI in AVN patients using subjective questionnaires and objective vestibular function tests.
Patients and methods
Dizziness & fall risk assessment and intervention
To assess the major risk factors related to dizziness and the possibility of falls, the authors developed a protocol named DFRAI, which comprises a basic survey of the patient’s medical history, medications, physiological functioning of the body, and vestibular function, along with objective vestibular function tests and information obtained from a home visit by a nurse, with interventions for dizziness.9–11
The contents of the protocol are summarized in Figure 1. The basic patient survey comprised questions regarding the patient’s name, identification (ID), sex, birth date, insurance coverage, residence type, and job. The medical history assessment comprised questions regarding previous fall and dizziness history, previous operation(s), hypertension, diabetes, smoking, drinking, exercise, weight gain or loss, and sleep disturbances. The assessment of medications surveyed the use of central nervous system (CNS) drugs, and sedatives, including benzodiazepines, anti-depressants, and diuretics, as well as the number of medications. The vestibular function questionnaire comprised the VAS score for dizziness, DHI, and the Survey of Activities and Fear of Falling in the Elderly (SAFE). 11 The objective vestibular function tests comprised video nystagmography (VNG), the sensory organization test (SOT), caloric test, and cervical vestibular evoked myogenic potentials (cVEMP). The survey conducted during home visits by nurses comprised a vestibular function questionnaire, evaluation of brightness using illumination photometry, and checks of floors, stairs, kitchens, bathrooms, and bedrooms. Interventions for dizziness comprised education, exercise, medication, referral, and environmental modification.9,12–15

Summary of the dizziness & fall risk assessment and intervention (DFRAI). DFRAI is a comprehensive solution for dizziness that comprises subjective/objective vestibular surveys, fall prevention, rehabilitation exercises, home environment intervention, and drugs to control dizziness.
The study design is summarized in Figure 2. The home visit was conducted 1 month after the onset of disease, and objective vestibular function tests were performed at the time of admission and 3 months after the onset of disease. Vestibular function questionnaire assessment was performed at the time of admission, during the home visit (1 month), and 3 months after the onset of disease.

Falls refer to sudden falling accidents resulting in injury and pain to the human body. Fall accidents mainly occur in patients with dizziness or in elderly people but can occur even in young people who have not adapted to the unfamiliar hospital environment. This study assessed the risk of dizziness and falls and evaluated the pattern of recovery after vestibular rehabilitation in acute vestibular neuritis patients at a tertiary hospital. This study also evaluated the efficacy of vestibular rehabilitation to improve vestibular function in acute vestibular neuritis.
Written informed consent for participation in this research was obtained from all patients, and the study was approved in September 2016 by the Institutional Review Board of the Korea University Anam Hospital (ED15350, Seoul, Republic of Korea). The study results have been reported in accordance with the STROBE guidelines. 16
Patients with AVN
This prospective study involved patients with AVN who visited the dizziness clinic of our medical center. Patients were diagnosed as having AVN if they presented with acute-onset (within 1 day) symptoms along with sustained vertigo, unidirectional horizontal spontaneous nystagmus aggravated by a head-shaking test, and positive unilateral bedside head impulse test. Inner ear diseases, such as Meniere’s disease, perilymphatic fistula, autoimmune inner ear disease, vestibular migraine, and central vertigo were excluded.
Patients with AVN were usually admitted for approximately 5 days and were treated with vestibular suppressants, high-dose oral steroids (64 mg methylprednisolone tablets [Methylon; Alvogen Inc., Pine Brook, NJ, USA]) for 12 days, and intravenous (IV) antiviral agents for 5 days.
The patients were evaluated using a survey of dizziness and fall risk, which was prepared using the Delphi method by 10 medical/nursing professors in South Korea. The survey of dizziness and fall risk comprised a VAS for dizziness, assessment of previous fall and dizziness history, and evaluations using the Morse fall scale, DHI, and SAFE. Patients were given three types of physical tests: 30-second chair stand test, four-stage balance test, and the timed up and go test. These tests are certified by the Centers for Disease Control and Prevention (CDC). The patients received education regarding customized vestibular rehabilitation over the course of AVN. Vestibular rehabilitation comprised adaptation (Figure 3) and substitution exercises (posture and gait training), and plans were customized and implemented to address the patient’s specific problems. Vestibular function was evaluated at the time of the initial attack and 3 months after the vertigo attack, to validate the recovery of objective vestibular function.5,9

Adaptation exercises in vestibular rehabilitation. (a) Eye saccade exercise: The patient places two objects at eye level, and with the head fixed, the patient quickly focuses on the two immovable objects using only eye movement. (b) Smooth pursuit exercise: With the head fixed, the patient uses only eye movement to slowly follow the object moving up, down, left, and right. (c) Vestibulo-ocular reflex (VOR) 1 exercise: Keeping the object fixed in front at arm’s length, the patient looks at the object by moving the head up, down, left, and right. (d) VOR 2 exercise: The patient performs the VOR 1 exercise while rotating the head in the opposite direction to the object.
Statistical analysis
All values are presented as mean ± standard deviation (SD) using the SPSS 13.0 statistical program (SPSS Inc., Chicago, IL, USA). The paired t test was used for data pairs, and multiple data were analyzed using analysis of variance (ANOVA). A P value less than 0.05 was considered statistically significant.
Results
Demographics
Forty-one patients (18 women and 23 men) with a mean age of 58.4 ± 16.1 years were enrolled in this study.
Recovery of subjective responses in AVN
In AVN, changes in dizziness degree were estimated using a VAS. At the initial AVN attack, the VAS score for all patients was 8.9 ± 1.7. One month after the attack, the VAS score improved to 2.2 ± 1.8. Three months after the attack, the patients had nearly recovered from dizziness, and their VAS score was 0.5 ± 0.9. Thus, the VAS score improved significantly from the initial attack of AVN to 3 months after the attack (Figure 4a; p < 0.001).

Recovery of subjective responses in acute vestibular neuritis (AVN). (a) In AVN, changes in the degree of dizziness were estimated using a visual analog scale (VAS). At the initial AVN attack, the mean ± standard deviation VAS score was 8.9 ± 1.7. One month from the attack, the VAS score improved to 2.2 ± 1.8. Three months from the attack, patients had nearly recovered from dizziness, and the VAS score was 0.5 ± 0.9. Thus, VAS improved significantly from the initial AVN attack to 3 months after the attack (p < 0.001). (b) Changes in dizziness degree were estimated using the dizziness handicap inventory (DHI). At the initial AVN attack, the DHI score was 76.6 ± 18.3. One month from the attack, the DHI score improved to 20.5 ± 27.3. Three months from the attack, patients had nearly recovered from dizziness, and the DHI score was 2.6 ± 5.5. Thus, the DHI score improved significantly from the initial AVN attack to 3 months after the attack (p < 0.001). (c) Changes in the degree of fear of falling (FOF) were assessed using the Survey of Activities and Fear of Falling in the Elderly (SAFE). At the initial AVN attack, the FOF score was 24.3 ± 12.4. One month from the attack, the FOF score improved to 3.9 ± 5.7. Three months from the attack, patients had nearly recovered from dizziness, and the FOF score was 1.6 ± 3.4. Thus, FOF improved significantly from the initial AVN attack to 3 months after the attack (p < 0.001). Even at 1 month from the attack, the FOF score had almost normalized to baseline.
Changes in the dizziness degree were estimated using the DHI. At the initial AVN attack, the DHI score was 76.6 ± 18.3, and 1 month later, the DHI score had improved to 20.5 ± 27.3. Three months after the attack, patients had nearly recovered from dizziness, and their DHI score was 2.6 ± 5.5. Thus, the DHI score improved significantly from the initial attack to 3 months after the attack (Figure 4b; p < 0.001).
FOF was estimated using SAFE. At the initial attack of AVN, the FOF score was 24.3 ± 12.4, and 1 month after the attack, the FOF score improved to 3.9 ± 5.7. Three months after the attack, the patients had nearly recovered from dizziness, and the FOF score was 1.6 ± 3.4. Thus, FOF improved significantly from the initial attack to 3 months after the attack (p < 0.001). Even at 1 month after the attack, FOF had almost normalized to baseline (Figure 4c).
Changes in posturography findings as a result of AVN
Vestibular function was evaluated at the time of the initial attack and 3 months after the vertigo attack in patients with AVN. In the SOT using computerized dynamic posturography (CDP), the initial composite score was 63 ± 13.1, which improved to 77.5 ± 4.9 3 months from the vertigo attack (p < 0.001). The initial score for the somatosensory (SOM) system was 95.8 ± 4.1, which was sustained at 96.8 ± 1.9 after 3 months. The initial score for the visual (VIS) system was 74.4 ± 13.6, which improved to 86.5 ± 5.3 after 3 months (p < 0.001). The initial score for the vestibular (VEST) system was 36.8 ± 29.8, which improved to 67.4 ± 10.4 after 3 months (p < 0.001), and the initial score for the preference (PREF) system was 101 ± 19.5, which was sustained at 100.4 ± 7 after 3 months. Thus, the SOT scores for the composite evaluation, visual system, and vestibular system improved significantly 3 months after the vertigo attack (Figure 5).

Vestibular function was evaluated at both the initial attack and 3 months after the vertigo attack in patients with acute vestibular neuritis (AVN). In the sensory organization test (SOT) using computerized dynamic posturography (CDP), the initial composite mean ± standard deviation score was 63 ± 13.1, which improved to 77.5 ± 4.9 3 months from the vertigo attack (p < 0.001). The initial score for the somatosensory (SOM) system test was 95.8 ± 4.1, which was sustained at 96.8 ± 1.9 3 months from the vertigo attack. The initial score for the visual (VIS) system test was 74.4 ± 13.6, which improved to 86.5 ± 5.3 3 months from the vertigo attack (p < 0.001). The initial score for the vestibular (VEST) system test was 36.8 ± 29.8, which improved to 67.4 ± 10.4 3 months from the vertigo attack (p < 0.001). The initial score for the preference (PREF) system test was 101 ± 19.5, which was sustained at 100.4 ± 7 3 months from the vertigo attack. Thus, the composite, visual, and vestibular SOT scores improved significantly 3 months from the vertigo attack.
Changes in the caloric test results in AVN
Vestibular function in AVN patients was evaluated at the time of the initial attack and three months later. Using the bi-thermal caloric test, both canal paresis (CP), which indicates unilateral vestibular weakness (UW), and directional preponderance (DP) were estimated in patients with AVN. The mean score for the initial CP was 42.9 ± 35.2, which improved to 29.9 ± 23.5 3 months later (p < 0.01). Thus, objective vestibular function using the caloric test improved significantly 3 months after the vertigo attack (Figure 6).

Vestibular function was evaluated at both the initial attack and 3 months later in patients with acute vestibular neuritis (AVN). Using a bithermal caloric test, both canal paresis (CP), which indicates unilateral vestibular weakness (UW), and directional preponderance (DP) were estimated in patients with AVN. The mean ± standard deviation score for the initial CP was 42.9 ± 35.2, which improved to 29.9 ± 23.5 3 months from the vertigo attack (p < 0.01**). Thus, objective vestibular function using caloric testing improved significantly 3 months from the vertigo attack. Effective vestibular rehabilitation may improve both central and peripheral compensation of the vestibular system.
Changes in the cVEMP test in AVN
Using the cVEMP test, vestibular function was evaluated at the time of the initial attack and 3 months later in patients with AVN (Figure 7). On the pathological side, the initial cVEMP score was 174.4 ± 148.5, which changed to 189.5 ± 139.5 3 months later. On the normal side, the initial cVEMP score was 275.8 ± 164.4 initially, and 205.5 ± 116.3 3 months after the vertigo attack. Both initial and 3-month cVEMP scores between the pathological side and normal side were not significantly different. The inter-aural amplitude difference (IAD) was 0.29 ± 0.22 initially, and 0.25 ± 0.18 3 months after the vertigo attack. The IAD value recovered from 0.29 to 0.25, but the change in IAD after 3 months was not significantly different.
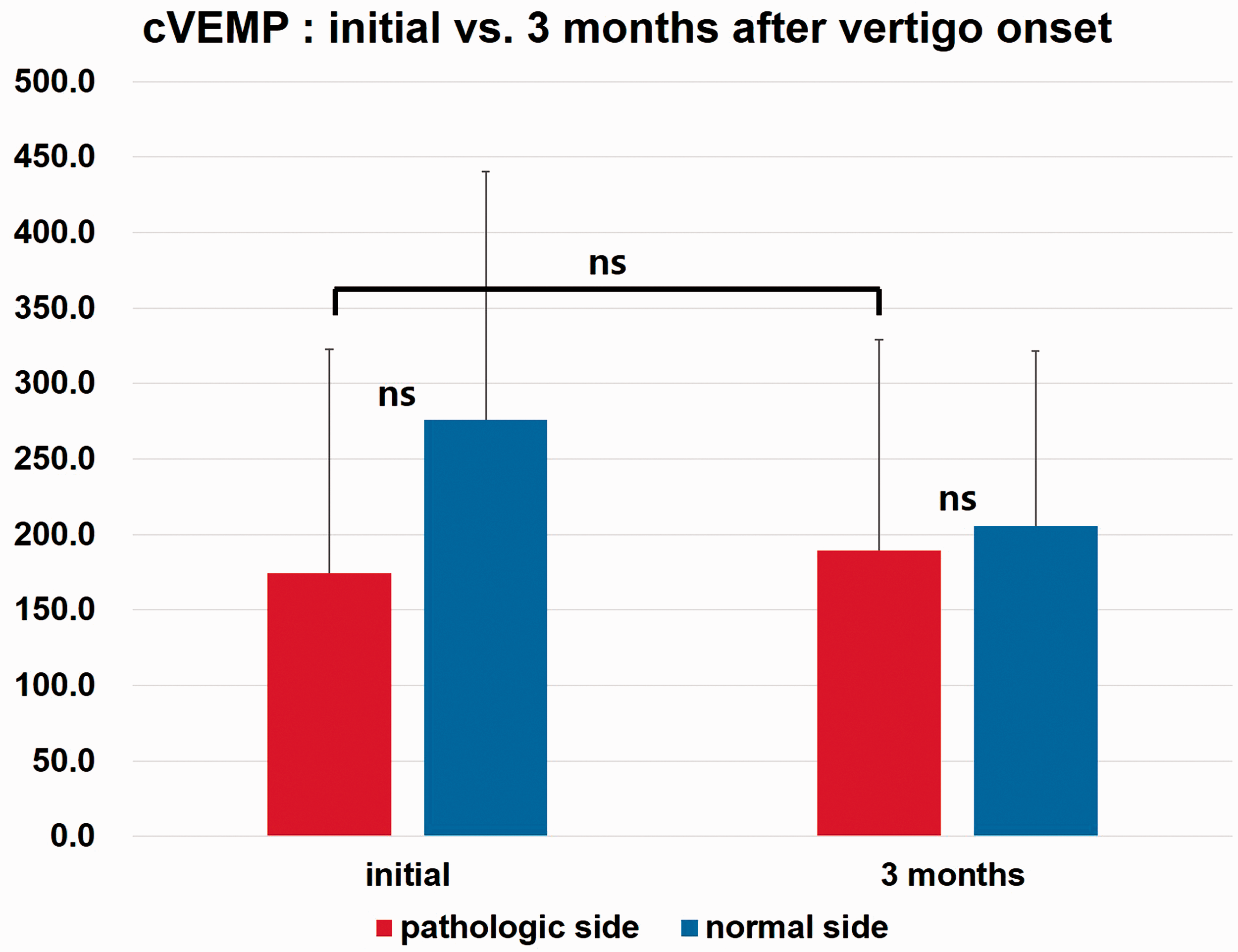
Using cervical vestibular evoked myogenic potentials (cVEMP) assessment, vestibular function was evaluated at the initial attack and 3 months later in patients with acute vestibular neuritis (AVN). On the pathological side, the mean ± standard deviation cVEMP score was initially 174.4 ± 148.5 and showed a non-significant change to 189.5 ± 139.5 3 months from the vertigo attack. On the normal side, the cVEMP score was 275.8 ± 164.4 initially, and 205.5 ± 116.3 3 months from the vertigo attack. Both initial and 3-month cVEMP scores were not significantly different between the pathological and normal sides. Inter-aural amplitude difference (IAD) was 0.29 ± 0.22 initially and 0.25 ± 0.18 3 months from the vertigo attack. The IAD value recovered from 0.29 to 0.25, but the change in IAD between the initial and 3-month value was not significant (ns).
Discussion
With the increasing use of medications for dizziness, the adverse effects of drugs and polypharmacy should be considered for complete control of dizziness. 17 Thus, appropriate consultation or referral and adequate education regarding vestibular suppressants are essential. Furthermore, several medications cause general weakness and even dizziness, especially after long-term use. 9 Physicians must carefully use appropriate medication to treat dizziness, and patients with dizziness should be aware of the effects of these drug.18,19
Falls refer to sudden falling accidents that result in injury and pain to the human body. Fall accidents occur mainly in patients with dizziness or in elderly people, but can occur even in young people who have not adapted to unfamiliar hospital environments.12,13,20 With an aging society, increased numbers of patients with dizziness, and increased use of medical services, the incidence of falls is increasing each year.7,21,22 In the USA, approximately 3 million older people suffered fall accidents in 2016, and approximately 1 million patients are hospitalized each year mainly because of associated head or hip injury. Furthermore, dizziness and falls are the most common causes of traumatic head injury. 23 Fall-related medical costs totaled more than $50.0 billion (US dollars), and overall medical spending for fatal falls was estimated at $754 million in 2015. 24
In our study, DFRAI, a new treatment for dizziness, was associated with improvement in subjective dizziness in AVN patients. Vestibular function according to the SOT results also effectively improved 3 months after acute vertigo in patients with AVN. The improvement in SOT scores was significant for the total composite score, visual score, and vestibular score. The measures for CP and DP in the caloric test, which are objective vestibular values, showed significant improvements 3 months after the onset of vertigo in AVN. Therefore, DFRAI is an effective treatment system for acute dizziness. DFRAI is a comprehensive dizziness control system that considers all factors, such as subjective/objective vestibular surveys, fall prevention, rehabilitation exercises, home environment intervention, and dizziness control using various drugs.9,14
In this study, the cVEMP value improved after treatment for acute dizziness, but the improvement was not significant. This could be attributed to the extremely high SD values because the cVEMP values in patients of various ages in the experimental group differed greatly. Although DFRAI treatment is strongly expected to reduce fall risk in AVN patients, we did not identify a statistically significant effect. One reason for this finding was that the fall probability and reporting rate were quite low; therefore, it was difficult to prove whether fall risk improved, with the small amount of experimental data. In our hospital, the number of hospitalized patients over 5 years (2011–2015) was 215,086, and the reported number of fall patients was 477; thus, the annual reported patient fall rate was estimated at 0.22%.9,14 A large-scale study is needed to prove improvement in fall risk with changes in treatment policy.
In our hospital, 98/477 (20.5%) patients suffered falls due to dizziness. The rate of taking dizziness-inducing drugs (stabilizers, such as benzodiazepines, anti-depressants, anti-anxiety drugs, anti-psychotics, sleeping pills, and hypnotic sedatives) was higher in patients with dizziness-induced falls (42.9%) than in those with falls attributable to other causes (25.3%). 14 Therefore, in patients with dizziness, a detailed survey and adjustment of sedative drugs are essential for preventing falls.
To effectively evaluate and treat acute dizziness, a breakthrough treatment system needs to be implemented. According to the findings in this study, we recommend the potential therapeutic system for dizziness named DFRAI, which comprises a basic survey of patients and their medical history, medications, physiological function, and vestibular function; objective vestibular function tests; home visits by nurses; and interventions for dizziness. The role of a professional nurse is emphasized in this system because nurses provide education regarding vestibular rehabilitation exercises, and because they visit the patients in person to check and improve the environmental risks in the home, which can become risk factors for dizziness and falls. During rehabilitation, emphasis is placed on three aspects: vestibular rehabilitation exercises, strength exercises, and home environment improvement.5,9 The vestibular rehabilitation exercises and strength training are conducted in three stages: supervised, group, and self-rehabilitation.5,25 Because complete recovery of vestibular function does not occur after 3 months, patients should be encouraged to follow-up even if they experience relief from dizziness.
To the best of our knowledge, this is the first study evaluating the assessment and intervention of falls after AVN. However, this study has several limitations. First, this was not a randomized controlled trial, and there was no control group. Therefore, it cannot be stated that DFRAI provided superior results over conventional treatment. Second, video head impulse testing and subjective visual vertical testing, which are useful objective tests to evaluate vestibular function, were not performed. Finally, therapeutic evidence supporting the use of steroids and antiviral agents in this study is controversial.26–28
We believe that applying the DFRAI to patients with AVN will have a positive effect in dizziness recovery and fall prevention. However, important constraints are workforce availability and cost. Currently, insurance coverage does not clearly include dizziness rehabilitation treatment and environmental improvement visits.
Treatment of acute dizziness is not limited to simply administering drugs that control dizziness. It is important to accurately evaluate the patient’s current state by conducting several certified subjective/objective vestibular function tests. Doctors must also thoroughly prevent falls in patients with dizziness and attempt to implement a comprehensive and ideal rehabilitation program comprising vestibular rehabilitation exercises, strength exercises, and home environment improvement.
Footnotes
Acknowledgements
We thank JN Chang for performing the patient education and home visits.
Declaration of conflicting interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a National Research Grant funded by a Korea Medical Device Development Fund grant, which was funded by the Korea government (Ministry of Science and ICT, Ministry of Trade, Industry and Energy, Ministry of Health & Welfare, Ministry of Food and Drug Safety) (Project Numbers: KMDF_PR_20200901_0183-2021-02, 1711138387); Korea government (Ministry of Science, ICT) (NRF-2019M3E5D1A0106899912); Korea Health Industry Development Institute (R1606512, R1621963, R1429733); and Korea University Research Fund (K2005001, K2008511, K2021561, K2100821). These funding sources provided financial support, only, and played no specific scientific role in this study.