
Abstract
Rhabdomyolysis, a potentially life-threatening syndrome, is caused by the breakdown of skeletal muscle cells and leakage of intramyocellular contents into the bloodstream. The treatment of rhabdomyolysis resulting from chronic sacrococcygeal pressure ulcers has been rarely reported. A 62-year-old man developed a high fever and dark-colored urine. For the past 30 years, he had lived with paraplegia, which led to his immobility. Physical examination showed evidence of repeated dehiscence and exudation of the wound on his sacrococcygeal region with loss of skin sensation. Upon corroboration of the physical examination findings and laboratory test results, the patient was diagnosed with rhabdomyolysis with an acute infection resulting from sacrococcygeal pressure ulcers. We first debrided the necrotic tissue and then repaired the chronic ulcer. The wound dressing was changed frequently, and antimicrobial therapy and nutritional support were included in the treatment. The fever and dark-colored urine gradually resolved postoperatively. The patient’s renal function also improved according to the typical laboratory indicators, and the size of the pressure ulcers decreased to some extent. The patient was discharged after 1 month of hospitalization. This case highlights that accurate diagnosis is critical for administration of precise treatment to paraplegic patients with progressive rhabdomyolysis.
Introduction
Rhabdomyolysis, a critical condition characterized by destruction of the membrane integrity of skeletal muscle cells, is caused by a series of factors affecting the membrane, membrane channels, and energy supply of muscle cells. Consequently, intramyocellular components such as myoglobin, creatine kinase (CK), and small molecules are released into the blood circulation. 1 The typical symptoms of this clinical syndrome are muscle pain, muscle weakness, and tea-colored urine. Severe cases can lead to serious problems such as acute kidney injury, disseminated intravascular coagulation, 2 and even death. Rhabdomyolysis syndrome can be caused by factors that result in muscle ischemia, hypoxia, and necrosis, such as crush syndrome, frostbite, leakage, electric shock, burns, severe soft tissue contusion, and limb replantation.3,4 CK and its isoenzymes in the serum of most patients with rhabdomyolysis are markedly elevated, sometimes more than 10 times the normal limit. CK itself is not toxic; however, its increase is an important marker indicating that the muscle cell membrane has been destroyed, and it is also the most specific diagnostic indicator of rhabdomyolysis. The treatment of rhabdomyolysis syndrome should remove inciting factors and prevent complications, mainly through drug and surgical treatment. Early active treatment can achieve better therapeutic effects.
Although rhabdomyolysis is a well-known complication, an internationally accepted definition has not been established, leading to great uncertainty in clinical practice. We herein report a case of rhabdomyolysis and myoglobinuria that resulting from prolonged, unrelieved pressure ulcers in a paralyzed patient. The purpose of the present report is to provide insight, treatment ideas, and clinical evidence for further studies involving rhabdomyolysis.
Case presentation
Chief complaints
On 16 January 2019, a 62-year-old man was transferred to the emergency department of our hospital because of a high fever of 39.0°C and dark urine.
History of present illness
Three months before his admission to our hospital, the patient’s condition had worsened because of repeated dehiscence and exudation of wounds on the sacrococcygeal region. Therefore, the patient was admitted to our department in the horizontal position.
History of past illness
The patient’s medical history showed that he had sustained a lumbar vertebral injury approximately 30 years before his admission to our hospital. Although the patient underwent surgery immediately, he remained paralyzed. Additionally, 10 years before his admission to our hospital, sacrococcygeal bedsores emerged and he underwent debridement and muscle flap application at Hangzhou Hospital of Traditional Chinese Medicine (Hangzhou, China).
Physical examination
Physical examination showed that the size of the infected wound was about 2 × 4 cm, and its depth reached the surface of the sacrum (Figure 1(a)). Amyotrophy of both lower limbs was obvious, with the disappearance of cutaneous expression of sensation. Other examination findings were unremarkable except for the absence of a physiological reaction and pathological character on both lower extremities.

Wound photographs. (a) Preoperative photograph showing the size, depth, and condition of the wounds, among which the infected one was festered. (b–d) Intraoperative photograph showing that the distal wound was debrided and sutured first, and the pus and necrotic muscle was then removed from the proximal wound. (e, f) Postoperative photograph showing that the wounds had healed well after 7 days and 1 month.
Laboratory examinations
Table 1 shows the patient’s laboratory results after admission to our hospital. The CK level was significantly elevated.
Treatment
Because of the patient’s complex and critical condition, we decided to perform debridement the day after consultation with a multidisciplinary team. Intraoperative exploration revealed that the distal wound was not connected to the proximal wound, and there was no obvious necrotic tissue in the wound. Thus, the distal wound was debrided and sutured (Figure 1(b), (c)). We then removed the pus and necrotic muscle within the proximal wound, which was a large cavity under necrotic slough. Fresh granulation tissue could be observed after complete debridement procedures (Figure 1(d)). The patient also underwent frequent dressing changes, antimicrobial therapy, correction of electrolyte imbalances and acidosis, and nutritional support. Three days after the surgery, the suture area was dry and clean without obvious swelling or exudation (Figure 1(e)). The dark urine began to gradually lighten in color the day after the surgery and returned to a normal color on day 5. The patient’s fever resolved on day 3 (Figure 2(a)). His CK level peaked on the first day, gradually decreased postoperatively, and then returned to normal on day 9 (Figure 2(b)). His white blood cell count and C-reactive protein concentration decreased and returned to normal on days 7 and 11, respectively (Figure 2(c), (d)). The patient was finally discharged after 1 month of hospitalization. Three months after the surgery, the wound had healed well and there was no sign of infection (Figure 1(f)).
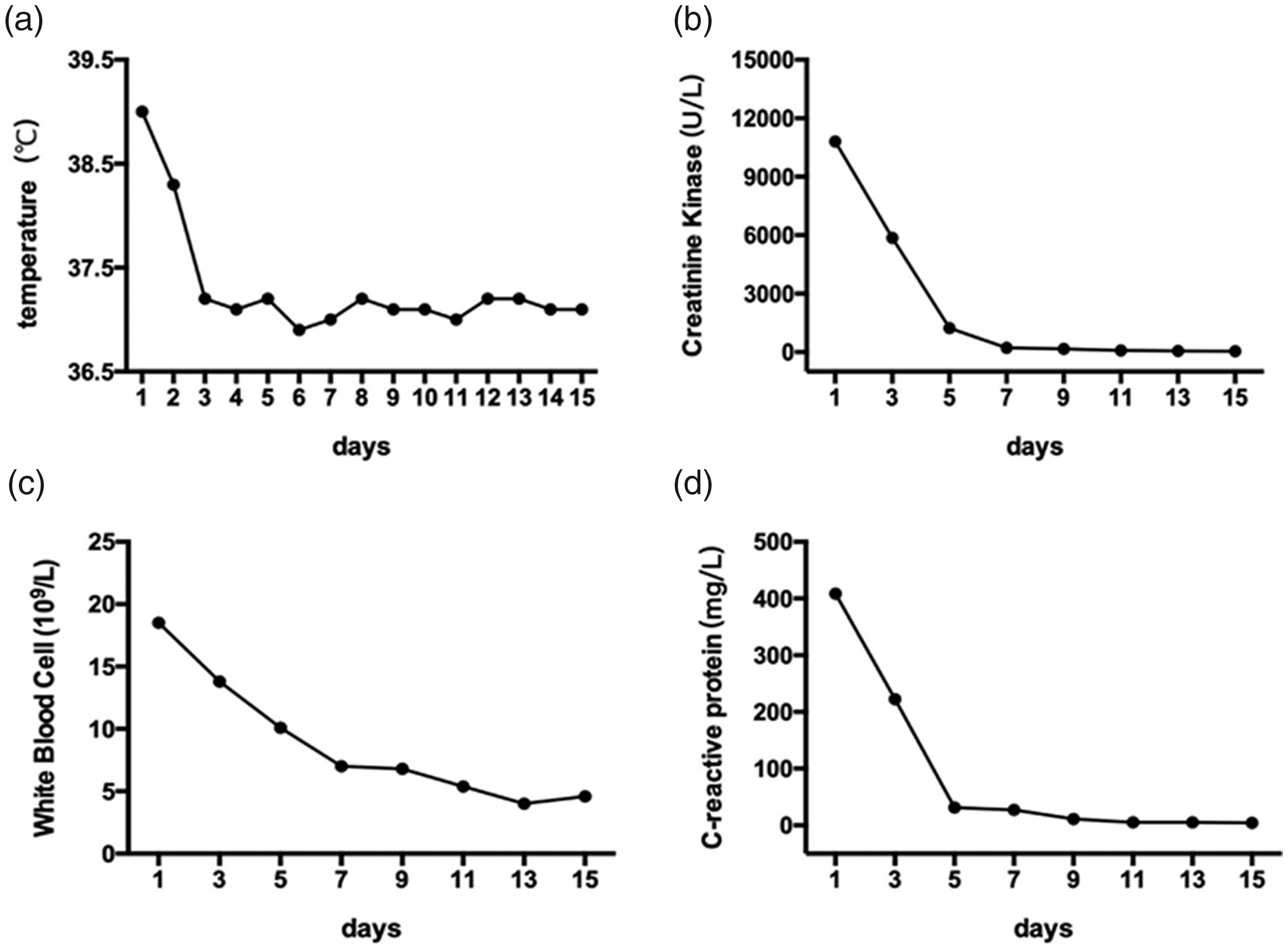
Clinical course of the patient. (a) The body temperature returned to normal on day 3. (b) The creatine kinase level peaked on day 1 and decreased to normal on day 9. (c) The white blood cell count gradually decreased and returned to normal on day 7. (d) The C-reactive protein level decreased and returned to normal on day 11.
Discussion
Rhabdomyolysis, a complicated syndrome with serious potential complications, is associated with acquired or inherited causes. 5 In the present case, rhabdomyolysis was caused by chronic pressure ulcers in a paraplegic patient. Pressure ulcers, also termed pressure sores, bedsores, decubitus ulcers, or pressure injuries, are injuries of the skin and its underlying appendages and soft tissues caused by constant or prolonged pressure exerted on an unspecified part of the trunk, limb, or body region. These lesions mostly occur in people with certain conditions such as coma, drug overdose, surgery, paralysis, and spinal cord injury,6,7 which may lead to decreased mobility and difficulty in postural movement. 8 Therefore, as a serious complication of various chronic diseases, pressure ulcers may result in more severe problems. Common manifestations of rhabdomyolysis include muscle pain, tenderness, swelling, and weakness combined with fever, generalized weakness, increased white blood cell and/or neutrophil counts, and abnormalities in urine appearance. Statistically, about 13% to 50% of patients may develop acute renal failure, 9 leading to oliguria, anuria, or azotemia. However, the accurate incidence rate of rhabdomyolysis is difficult for clinicians to determine, especially in the emergency department, 10 because prospective studies assessing the morbidity of rhabdomyolysis are quite rare. Thus, few cases in the early stages of rhabdomyolysis are diagnosed in the clinical setting. Although numerous researchers study rhabdomyolysis, only a few reports have described the treatment of patients with rhabdomyolysis secondary to pressure ulcers. In one case of rhabdomyolysis caused by acute pressure sores, the patient eventually died. 11
In the present case, before the patient was admitted to our hospital, he was sent to the emergency department of a local hospital and did not receive a definitive diagnosis. However, sacrococcygeal pressure ulcers had been present for more than 10 years, and the wounds from some ulcers had been ruptured for more than 3 months. Notably, not only the patient’s family members but also the clinicians at the local hospitals had no awareness of the risks involved in the care of long-term bedridden patients. Importantly, with respect to prevention of further complications, the vigilance of patients with paraplegia and their family members should be enhanced in regard to identification and treatment of pressure ulcers. 12 As a severe complication of pressure ulcers, rhabdomyolysis needs to be prevented or more effectively identified during the early stages. Thus, education, awareness, and specific training are effective measures in the daily care of these patients.
The treatment of rhabdomyolysis is strictly based on accurate diagnosis. Aside from the fever, dark-colored urine, and metabolic disturbance of our patient, a sensitive indicator of rhabdomyolysis was the CK level, which reached 10,809 U/L. A higher CK level is associated with more severe muscle damage and a higher risk of acute kidney injury. Because of the critical condition and multidisciplinary problems of this case of rhabdomyolysis with acute infection, we organized a multidisciplinary diagnosis and treatment model implemented by the Orthopedics Department with input from the Nephrology Department, Infection Department, and Intensive Care Unit. Several physicians demonstrated that the patient had severe renal dysfunction and acute infection, and they suggested improving his renal function and controlling the infection preoperatively. However, other physicians believed that the necrotic muscle tissues in the sacrococcygeal bedsores were the primary and exact cause of other manifestations, and these physicians stated that debridement should be performed immediately to prevent fatal consequences such as renal failure and sepsis. We eventually adopted the latter opinion and performed debridement immediately. All symptoms and laboratory data gradually resolved or returned to normal postoperatively. To our knowledge, anesthetics mainly cause damage to renal function. In the present case, the patient had a long history of paraplegia, leading to the loss of skin sensation around the operative region. Thus, it was unnecessary to conduct an emergency operation with anesthesia to prevent further damage and reduce the risk of acute kidney injury.
This case illustrates that for patients complicated with rhabdomyolysis after surgery, it is even more important to remove the etiology than to immediately implement symptomatic treatment and infection control. The patient’s symptoms in this case markedly improved with thorough debridement. We believe that this case can provide treatment ideas for further research on rhabdomyolysis.
Conclusion
We have herein described a paraplegic patient who developed rhabdomyolysis and infection because of chronic sacrococcygeal pressure ulcers. Despite the rarity of rhabdomyolysis, it is important for surgeons to be familiar with possible complications. The best available evidence indicates that the prognosis depends on the extension and clinical severity of rhabdomyolysis as well as on early and prompt medical intervention. 13 We have reported this case to aid physicians in the diagnosis of rhabdomyolysis caused by chronic pressure ulcers.
Footnotes
Ethics statements
This study was approved by the Ethics Committee of Tongde Hospital of Zhejiang Province. We have de-identified all patient details in this case report. Written informed consent was obtained from the patient for publication of this report and any accompanying images. The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016). The reporting of this study conforms to the CARE guidelines. 14
Acknowledgments
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Zhejiang Province Public Welfare Technology Application Research Project (LGF21H270004), the Natural Science Foundation of Zhejiang Province (LY20H270002), the Medical Science and Technology Project of Zhejiang Province (2020RC048, 2021KY600), and the Chinese Medicine Research Program of Zhejiang Province (2020ZQ006, 2021ZB060).