
Abstract
Takotsubo syndrome is a condition that mimics acute coronary syndrome. The exact pathogenesis of the condition is unclear but it tends to occur more frequently in elderly women and a large proportion of cases have acute, former, or chronic neurologic or psychiatric disorders. Here we describe a 55-year-old female patient, who was brought to the emergency department presenting with a new-onset manic episode characterized by grandiosity, distractibility, decreased need for sleep, and increased goal-directed behaviours. She experienced chest pain approximately two days later, and non-ST elevation myocardial infarction was observed. The emergent coronary angiogram showed patent coronary arteries, and a diagnosis of Takotsubo syndrome was made. We suggest clinical multidisciplinary vigilance for somatic complaints, especially cardiac ones, in people with psychiatric disorders in order to make timely therapeutic interventions.
Introduction
Takotsubo syndrome (TTS), also known as apical ballooning syndrome or stress cardiomyopathy, is a condition that mimics acute coronary syndrome. 1 The clinical presentation includes chest pain, dyspnoea, ST segment deviation on the electrocardiogram (ECG), and elevation in cardiac biomarkers, but obstructive coronary artery disease is always absent on the coronary angiogram. 1 Although the exact pathogenesis of TTS is unclear, some hypotheses such as catecholamine cardiotoxicity or coronary microvascular impairment have been described. 2 TTS is often triggered by physical or emotional stress and typically occurs in elderly women. 1 The left ventricular dysfunction usually recovers soon after the initial critical event. Although the prognosis of TTS is associated with a favourable outcome and a low incidence of major adverse cardio-cerebrovascular events, the in-hospital mortality rate can be as high as 10%.1–3 If these patients are diagnosed promptly and timely and appropriate treatment are given, then outcomes may improve.
Researchers have found a strong association between pre-existing psychiatric illness, particularly anxiety and mood disorders, and TTS. 3 Occasionally, the clinical presentations of TTS and mood disorder can overlap. Here, we describe a middle-age female, who presented with a manic episode and subsequently was diagnosed with TTS.
Case Report
A 55-year-old female patient without any previous medical or psychiatric history was brought to the emergency room (ER) because of her emotional instability following a serious fight with a bus driver. At the ER, she presented with a demanding attitude, and had irritability, distractibility, and flights of ideas. Her family reported that in the previous three weeks, she exhibited grandiosity, a decreased need for sleep, and increased goal-directed behaviours. Delusions of reference and persecution were also noted without auditory or visual hallucinations. Blood tests, toxicology screen, electrocardiography (ECG), and brain computed tomography (CT) were arranged. The patient and her family requested hospital discharge while the test results were pending. Laboratory data showed non-remarkable blood and biochemistry results, normal thyroid function, a negative toxicology screen and non-remarkable brain CT. The ECG showed normal sinus rhythm but QTc prolongation (489ms) (Figure 1).

Electrocardiogram (ECG) from the patient’s first hospital visit (left panel): normal sinus rhythm with QTc prolongation (489ms).
Approximately 30 hours later, the patient returned to the ER because of challenging irrational thoughts. Following psychiatric consultation, risperidone 1mg/day and valproic acid 700mg/day were prescribed and psychiatric acute ward hospitalization was arranged. However, 16 hours later, while the patient was waiting to be hospitalized, she complained of chest pain, and her ECG showed nonspecific ST-T changes (Figure 1). In addition, she had an elevated troponin-I level (2.97ng/ml). She was diagnosed with non-ST elevation myocardial infarction and the ER doctors activated immediate cardiac catheterization.
A coronary angiogram showed patent coronary arteries (Figure 2) and the patient was admitted to the non-emergency cardiovascular ward. Echocardiography showed mild left ventricular dysfunction and ampulla cardiomyopathy with left ventricular apical mural thrombus (Figure 3). Brain magnetic resonance angiography (MRA) showed a small embolic infarction in the left temporo-occipital cortices, compatible with the cardio-embolism. A diagnosis of Takotsubo cardiomyopathy was made, and losartan 50mg/day and apixaban 10mg/day were prescribed.
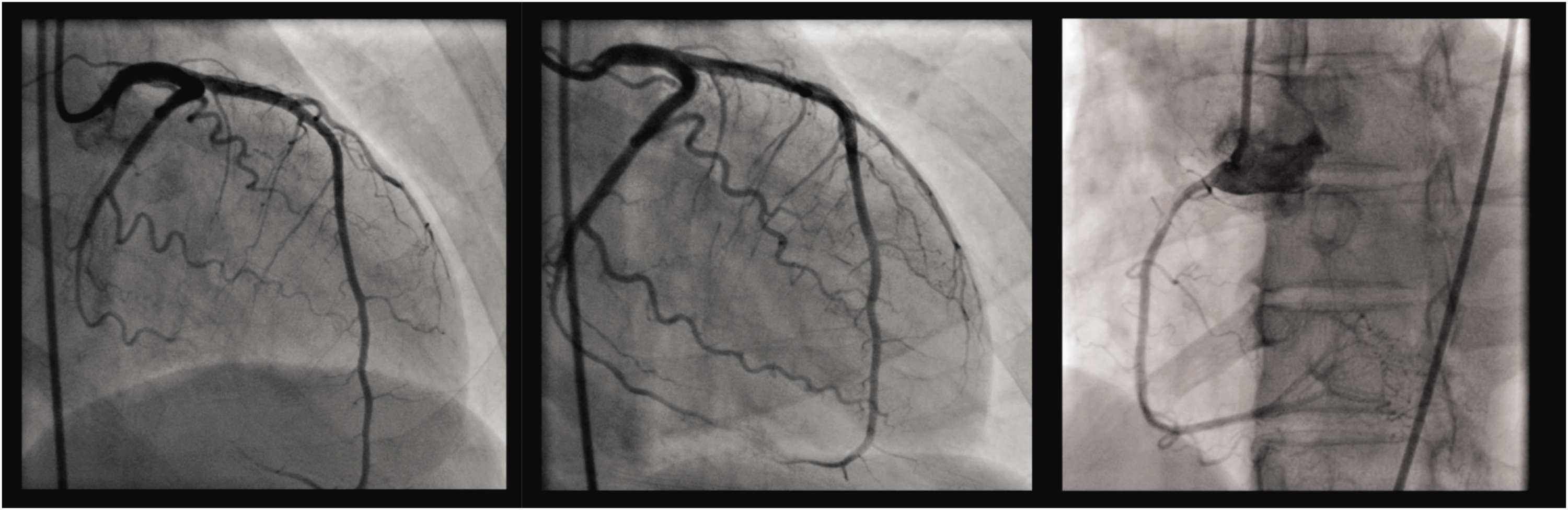
Coronary angiogram showed patent left coronary arteries in left anterior oblique cranial view (left), right anterior oblique caudal view (middle), and patent right coronary artery in left anterior oblique view (right).
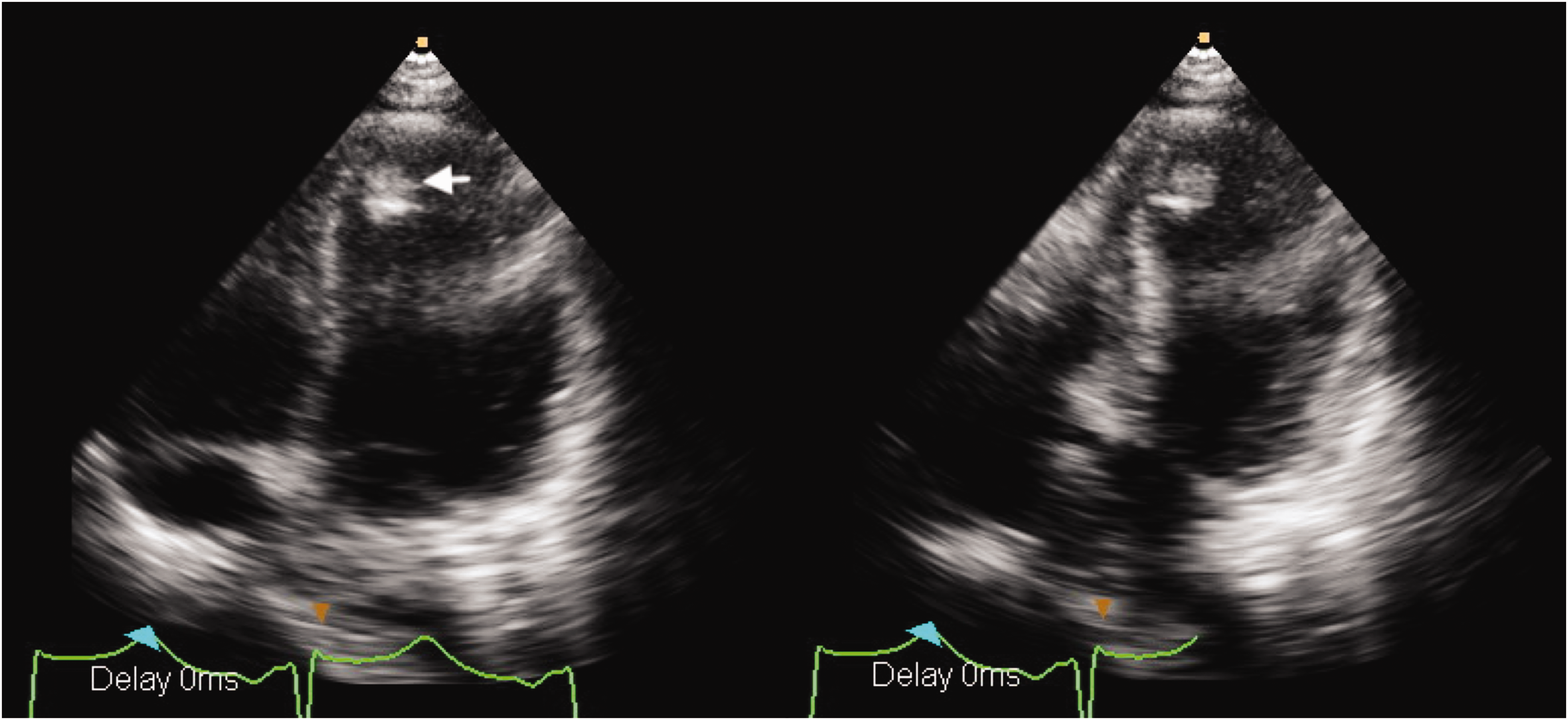
Echocardiography of end-diastolic (left) and end-systolic (right) apical four chamber views. Hyperdynamic basal part and akinetic apical part of left ventricle were observed. An apical thrombus was seen (arrow).
After one week of hospitalization, the patient had improved. A psychiatric consultation was made before the patient’s hospital discharge, and she was found to have increased self-esteem with less irritability, distractibility and racing thoughts. She was prescribed risperidone 1mg/day and valproic acid 500mg/day for her bipolar disorder.
This case report was approved by the Institutional Review Board of Chang Gung Memorial Hospital (protocol number: 202001201B0 and date of approval: July 8th, 2020) and informed consent was not required because it was a retrospective report and used anonymised data.
Discussion
Approximately one-third of patients with TTS have a pre-existing psychiatric illness. 3 Depressive and anxiety disorders are thought to be most related, though the association is controversial. 3 For example, an investigation by The International Takotsubo Registry showed that patients with TTS had significantly higher rates of depression and anxiety compared with controls, 1 while another study reported higher rates of major depressive disorders in TTS patients compared with controls but not anxiety disorders 4 and another study showed higher rates of anxiety but not depression compared with controls. 5
Previous studies have reported cases of TTS related to acute manic attacks6–8 or to an underlying bipolar disorder.9,10 The exact aetiology of TTS is still unknown, but one hypothesis is that psychiatric illness and chronic stress could activate the hypothalamic-pituitary-adrenal (HPA) axis, increasing release of catecholamines, 11 and subsequently causing TTS. 12 Indeed, bipolar disorders are known to lead to increased activation of the catecholamines, especially in manic state. 13 In addition, the use of psychotropic medications, including mood stabilizers or anti-depressants, could also cause TTS. 11 Therefore, it is difficult to distinguish if the cause of TTS is the bipolar disorder, the use of psychotropic medications, or even a combination of both factors.
In the case reported here, the patient, a 55-year-old woman, had an atypical onset. Although she presented with symptoms of bipolar disorder, she had no previous psychiatric history and was not receiving any psychotropic medication. Interestingly, bipolar disorders usually occur at approximately 20 years of age and the first symptom is usually a depressive episode. 14 A complete patient history was not taken so we cannot exclude the possibility that emotional risk factors may have caused her TTS. However, at her first clinic visit, she did not have any cardiac-related complaints and her ECG was normal apart from mild QTc prolongation. Following her return to the ER because of prominent psychiatric symptoms, she was prescribed risperidone and valproic acid and subsequently developed chest pain and ECG abnormalities. One study reported a case of TTS following a suicide attempt with an overdose of phenobarbital and risperidone. 15 However, the authors concluded that there was no evidence of a causal relationship between either drug and TTS. We are not aware of any studies involving use of valproic acid and TTS.
In summary, the patient reported here while presenting with a manic episode, had no previous psychiatric history. She did not have any cardiac-related complaints and only developed chest pain and ECG abnormalities approximately 16 hours after receiving antipsychotic mediation. In our case, the ER doctor astutely detected the patient’s cardiovascular complaints and made timely and appropriate management decisions. We suggest clinical multidisciplinary vigilance is required for people with psychiatric disorders presenting with somatic complaints, especially cardiac ones, because early intervention for TTS will provide a favourable outcome and increase survival rate. 16