
Abstract
Objective
Bilioenteric anastomotic stricture is a serious complication following choledochojejunostomy. Some patients develop intrahepatic lithiasis and biliary tract infection without dilation of the intrahepatic bile duct. The present study was performed to investigate the safety and efficacy of laparoscopy combined with choledochoscopy in patients with bilioenteric anastomotic stricture with access via the jejunal loops.
Methods
The data of 10 patients (7 men and 3 women; mean age, 60.8 ± 9.7 years; age range, 51–76 years) with potential bilioenteric anastomotic stricture without dilation of the intrahepatic bile duct from January 2015 to December 2019 were retrospectively reviewed.
Results
All 10 patients underwent surgery, and their clinical parameters were recorded. The mean surgery time was 181.5 ± 35.4 minutes, and the mean estimated blood loss was 32.0 ± 15.5 mL. No patients developed serious complications during the perioperative period. The short-term outcome analysis at 12 months indicated that the stenosis had been effectively dilated and that the liver function had improved.
Conclusions
The results of the present study demonstrated that laparoscopy combined with choledochoscopy with access via the jejunal loops is feasible in the treatment of bilioenteric anastomotic stricture and intrahepatic lithiasis.
Keywords
Introduction
Bilioenteric anastomotic stricture is a serious complication following choledochojejunostomy. The obstruction of bile excretion causes intrahepatic lithiasis, infection, fever, and biliary cirrhosis. 1
Several procedures have recently been performed to manage bilioenteric anastomotic stricture. Reoperation is traditionally the first choice, whereby the defective anastomosis is removed and replaced with a new anastomosis. However, reoperation is associated with a high risk of restenosis and biliary fistula, and many patients require several surgeries. 2 Thus, minimally invasive treatments are recommended to avoid these risks. Percutaneous transhepatic cholangioscopy (PTCS) is now extensively used to establish a channel to the intrahepatic bile duct via catheterization. Choledochoscopy is subsequently used to remove the stones and dilate the bilioenteric anastomotic stricture. 3 However, PTCS cannot be performed in patients without obvious dilatation of the intrahepatic bile duct because of the difficulties of biliary catheterization.
Thus, entry into the cholangiojejunostomy through other channels has been extensively investigated. For example, some digestive endoscopy specialists use endoscopic retrograde cholangiopancreatography to dilate the bilioenteric anastomotic stricture from the intestinal loop. 4 However, it is difficult to reach the bilioenteric anastomosis for subsequent treatment in patients with a long input loop or in the absence of skilled endoscopy specialists. B-mode ultrasound and computed tomography-guided intestinal loop puncture have also been used to establish a channel. 5 In addition, surgical techniques have been used to preset a subcutaneous intestinal loop for choledochoscopic examination and treatment. 6 Open or laparoscopic-assisted small bowel endoscopy can reportedly be used to revise the anastomosis via the limb of the jejunum. 7 However, the combination of laparoscopy and choledochoscopy in the treatment of bilioenteric anastomotic stricture has not yet been investigated.
In the present study, reoperation was performed in 10 patients with bilioenteric anastomotic stricture and intrahepatic lithiasis without obvious dilatation of the intrahepatic bile duct. The adhesions were separated via laparoscopy, and the jejunal loop was located and perforated. Choledochoscopy was subsequently performed to investigate and dilate the bilioenteric anastomosis. Finally, a T-tube was inserted into the intestinal loop to establish a channel for follow-up treatment. This minimally invasive technique is likely to be implemented in clinical practice.
Methods
Patients
Forty-five patients with intrahepatic lithiasis and bilioenteric anastomotic stricture from January 2015 to December 2019 were retrospectively analyzed. The inclusion criteria were confirmation of the diagnosis by magnetic resonance imaging, ultrasound, or cholangiography; no dilation of the intrahepatic bile duct, preventing PTCS from being performed; and fever, abdominal pain, or other symptoms of biliary tract infection. The exclusion criteria were the absence of a stricture in the anastomosis and the presence of complete occlusion in the anastomosis. The present study was approved by the Ethics Committee of the Second Affiliated Hospital of the School of Medicine of Zhejiang University (approval number: 2020-No. 1111). The requirement for informed consent was waived because the study was retrospective, data were collected using patients’ files, and confidentiality and anonymity were maintained throughout the study process.
Procedure
The whole procedure comprised two steps.
Step 1 (laparoscopic surgery): (1) Pneumoperitoneum was achieved via a subumbilical incision, and laparoscopy was performed. The adhesions were predominantly located in the right upper abdomen; thus, two trocar holes were created in the left abdomen for separation. (2) The adhesions were carefully separated, and the jejunal loop was placed near the lower edge of the liver. (3) An enterotomy was performed at the end of the jejunal loop, and a flexible choledochoscope was passed through to locate the anastomosis. (4) A 22-French T-tube was routinely inserted into the jejunal loop from the incision site to construct the fistula between the skin and jejunal loop (Figure 1).

Step-by-step process for access via jejunal loops during laparoscopy. (a) Abdominal adhesions. (b) Separation of adhesions. (c) Exposure and incision of jejunal loop. (d) Choledochoscopy. (e) Insertion of the T-tube in the jejunal loop. (f) Small incisions on the abdominal wall.
Step 2 (percutaneous choledochoscopy): (1) Step 2 was usually performed 6 weeks after Step 1. The T-tube was removed and a flexible choledochoscope was inserted through the fistula to find the anastomosis. (2) The stricture was dilated and the stones were retrieved using a holmium laser or balloon dilatation (Figure 2).

Dilation of bilioenteric anastomotic stricture via choledochoscopy. (a) Bilioenteric anastomotic stricture. (b) Holmium laser dilation. (c) Balloon dilation. (d) Dilated bilioenteric anastomosis and hepatolithiasis. (e) Investigation of the intrahepatic bile duct through the dilated bilioenteric anastomosis.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows, Version 19.0 (IBM Corp., Armonk, NY, USA). Data are presented as mean ± standard deviation. The Wilcoxon signed-rank test was used to compare differences between the preoperative and postoperative clinical parameters. A P value of <0.05 was considered to indicate a statistically significant difference.
Results
After application of our inclusion and exclusion criteria, the data of 10 patients were collected for this study. The main symptoms were intermittent fever (10/10 patients), abdominal pain (3/10 patients), and jaundice (1/10 patient). Three patients had malignant disease and seven had benign disease. All patients had previously undergone multiple surgeries (average of 1.7 surgeries).
The mean surgery time was 181.5 ± 35.4 minutes, and the mean estimated blood loss was 32.0 ± 15.5 mL. Conversion to open surgery was not performed in any cases, and no serious complications (abdominal hemorrhage, biliary leakage, or intestinal leakage) were recorded following surgery. The mean postoperative hospital stay was 6.6 ± 2.9 days, and the drainage tubes were removed prior to discharge. Choledochoscopy was performed 6 weeks after surgery. All details are presented in Table 1.
Patient characteristics.
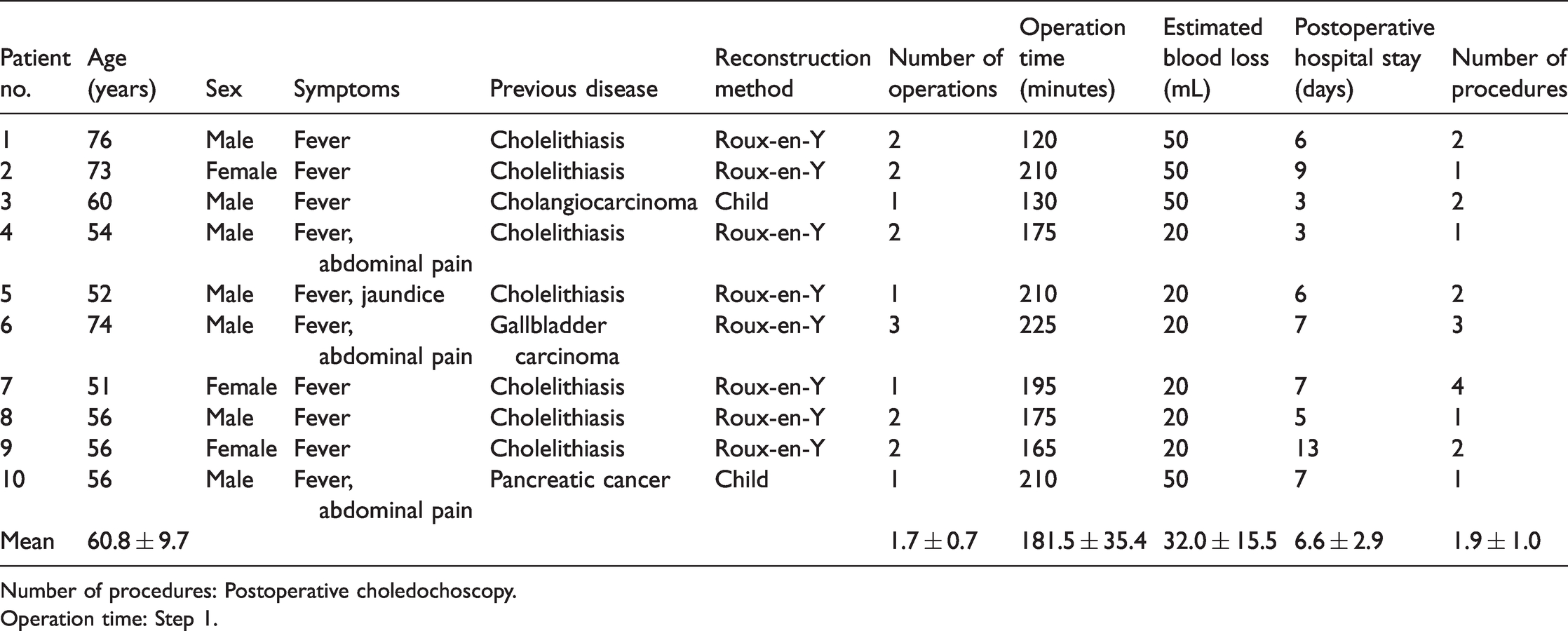
Number of procedures: Postoperative choledochoscopy.
Operation time: Step 1.
Dilation of the bilioenteric anastomosis and clearance of intrahepatic lithiasis were performed during or after Step 1 (usually after) using a holmium laser or balloon dilatation. Whether the strictures and residual stones required treatment was determined by cholangiography or choledochoscopy (Figure 3). Two or three cycles of dilation allowed the bilioenteric anastomosis to reach >0.8 cm, and the T-tube was then removed. All patients were followed up for at least 12 months. Notably, no fever, jaundice, or abdominal pain occurred in nine patients, while one patient developed occasional abdominal pain. The preoperative and postoperative diameters of the bilioenteric anastomosis were also calculated by magnetic resonance imaging or ultrasound, and the results showed that our procedure resulted in effective dilation of the bilioenteric anastomotic strictures (2.6 ± 0.7 vs. 7.1 ± 1.7 mm). Routine blood assessments and liver function indexes were reviewed and compared with those prior to surgery. The results demonstrated no significant differences in the levels of bilirubin, alanine aminotransferase, and aspartate aminotransferase between the two groups. However, the levels of bile enzymes, alkaline phosphatase (543.50 ± 224.43 vs. 271.14 ± 181.72 U/L), and gamma glutamyl transpeptidase (334.05 ± 203.23 vs. 141.12 ± 103.41 U/L) significantly improved after surgery (P < 0.05), suggesting postoperative improvement in liver function. Notably, no significant difference was observed in the leukocyte count or C-reactive protein level between the two groups (Table 2).

Preoperative and postoperative examination. (a) Preoperative magnetic resonance imaging showed the intrahepatic bile ducts. (b) Postoperative cholangiography via the T-tube revealed the bilioenteric anastomosis. (c) Postoperative cholangiography via the T-tube revealed the intrahepatic bile ducts.
Comparison of clinical parameters between preoperative and postoperative periods.
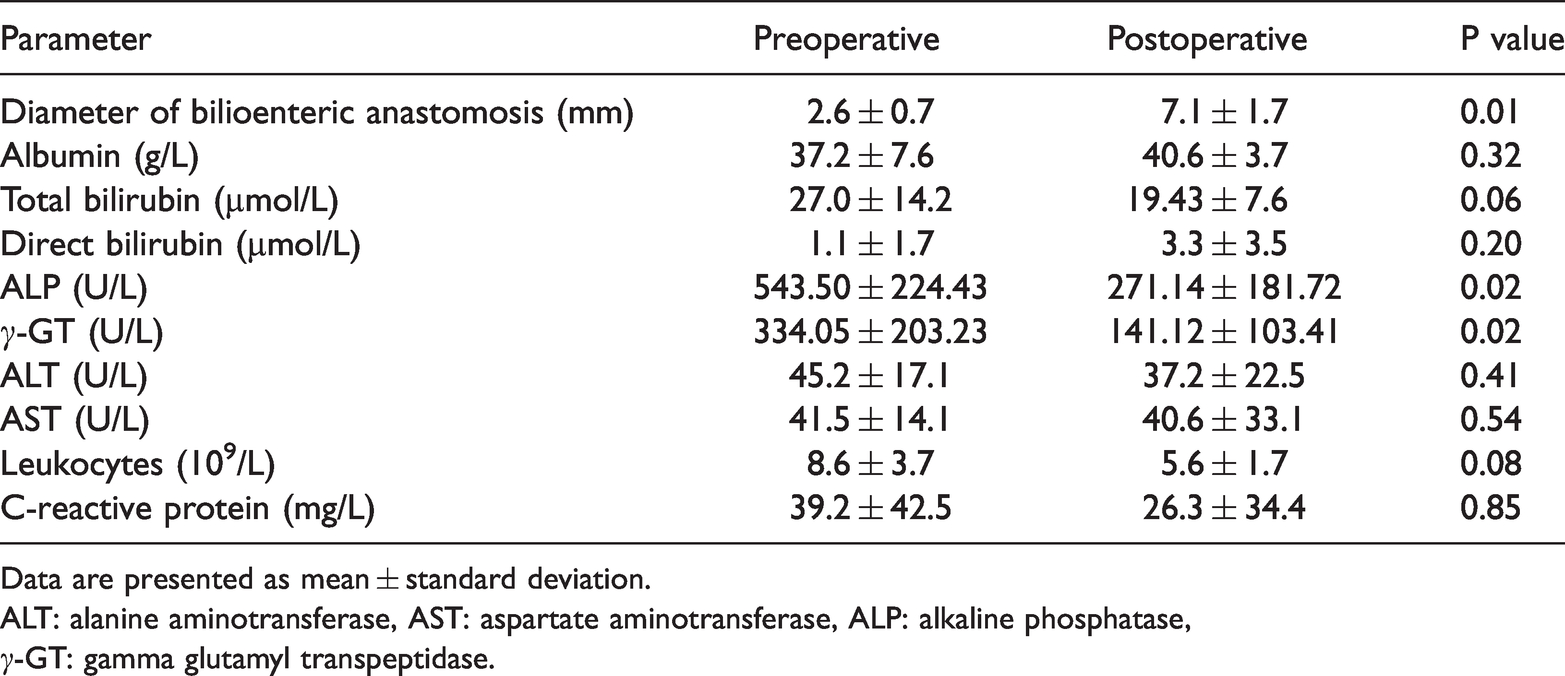
Data are presented as mean ± standard deviation.
ALT: alanine aminotransferase, AST: aspartate aminotransferase, ALP: alkaline phosphatase,
γ-GT: gamma glutamyl transpeptidase.
Discussion
Choledochojejunostomy is an essential procedure that allows bile to flow into the intestine following bile duct resection or injury, and it is extensively applied in the treatment of both benign and malignant diseases. Inflammation often occurs at the bilioenteric anastomosis site because of destruction of the physiological barrier, and the most serious complication is bilioenteric anastomotic stricture. Stricture can cause bile excretion disorder, resulting in the production of intrahepatic bile duct stones, bile duct inflammation, biliary cirrhosis, and other serious complications. 8 Avoiding stricture of the bilioenteric anastomosis remains a major surgical challenge. Despite development of novel methods, overcoming this issue remains difficult. 9
Choledochoscopy is extensively applied in patients with bile duct stones. Choledochoscopy has historically been used to remove bile duct stones during and after open surgery. 10 Laparoscopic choledochoscopy can now also be used to investigate the bile duct. 11 Notably, PTCS combined with choledochoscopy minimizes the invasiveness of treatment of intrahepatic bile duct stones and bilioenteric anastomotic stricture. 3 , 12 In clinical practice, however, patients without a dilated intrahepatic bile duct can also develop biliary tract infection or abdominal pain. Thus, using jejunal loops during choledochoscopy may benefit these patients.
The present study enrolled 10 patients with bilioenteric anastomotic stricture, 8 of whom underwent Roux-en-Y reconstruction and 2 of whom underwent Child reconstruction. In all cases, the intestinal loop passed through the mesocolon and reached the hepatic hilum. The adhesions were separated via laparoscopy, and the jejunal loop of the choledochojejunostomy was exposed in all cases; this suggests that it is feasible to locate the blind end of the jejunal loops under laparoscopy. Intestinal damage occurred during surgery but was repaired during the process of separation. In addition, all patients quickly recovered following surgery via laparoscopy. In previous studies, laparoscopy was used to locate the intestinal loop, and enteroscopy was performed to overcome the stricture of bilioenteric anastomosis in two cases. 7 In the present study, the end of the blind loop was selected as the puncture point. The potential bilioenteric anastomosis was then located by identifying the position of bile outflow under choledochoscopy, and the most commonly used dilation methods were a balloon and a holmium laser. Notably, the intestinal loop incision was directly sutured in previous studies, whereas a T-tube was inserted to form a sinus for future choledochoscopy in the present study. This was performed because restenosis is common and it is difficult to completely remove the intrahepatic bile duct stones via choledochoscopy-assisted laparoscopy. Patients in the present study underwent dilation (at least twice) and clearance of stones to achieve satisfactory results.
The surgical method presented here is not without limitations. First, it was impossible to diagnose the stricture of the bilioenteric anastomosis via cholangiography because of the difficulty of intrahepatic bile duct puncture in these patients. Thus, some patients had no stricture during surgery. The development of fever was likely caused by the reflux of intestinal contents to the intrahepatic bile duct. In addition, the water flow stimulated the jejunal loop and caused intestinal peristalsis, which made it difficult to perform choledochoscopy. Using warm saline water during choledochoscopy helped to avoid peristalsis, and the bile flow in the jejunal loop helped us to find the bilioenteric anastomosis. Furthermore, the T-tube was placed in the jejunum, which caused bile leakage and intestinal leakage around the T-tube. The T-tube in the intestinal loop was fixed using bilateral purse-string suturing to avoid potential leakage.
In conclusion, this novel surgical method presents promising results for the treatment of bilioenteric anastomotic stricture and intrahepatic lithiasis.