
Abstract
Objective
To compare clinical and operative results between laparoscopic primary repair (LPR) alone and LPR with highly selective vagotomy (LPR-HSV) in patients with duodenal ulcer perforation.
Methods
Clinical data from patients who underwent either LPR or LPR-HSV by resecting both sides of the neurovascular bundle using an ultrasonic or bipolar electrosurgical device for duodenal ulcer perforations, between 2010 and 2020, were retrospectively collected. Between-group differences in continuous and categorical variables were statistically analysed.
Results
Data from 184 patients (mean age, 49.6 years), who underwent either LPR (n = 132) or LPR-HSV (n = 52) were included. The mean operation time was significantly longer in the LPR-HSV group (116.5 ± 39.8 min) than in the LPR group (91.2 ± 33.3 min). Hospital stay was significantly shorter in the LPR-HSV group (8.6 ± 2.6 days) versus the LPR group (11.3 ± 7.1 days). The mean postoperative day of starting soft fluid diet was also significantly shorter in the LPR-HSV group (4.5 ± 1.4 days) than in the LPR group (5.6 ± 4 days). No between-group difference in morbidity rate was observed. The learning curve of the HSV procedure showed a stable procedure time after 10 operations.
Conclusions
LPR with HSV may be a safe and feasible procedure for selective cases who are at high risk for ulcer recurrence.
Introduction
Due to the development of proton pump inhibitor (PPI) treatment and Helicobacter pylori eradication therapy, elective surgery for peptic ulcers is rare. 1 However, complications caused by peptic ulcers require emergency surgery, with bleeding (73%), perforation (9%), and obstruction (3%) reported as the most common complications requiring emergency operations in the USA. 2 Of these, perforation accounts for approximately 10% of peptic ulcer complications, but is associated with the highest rate of mortality. 3
If a duodenal ulcer perforates, an emergency operation is needed. In the past, primary repair with truncal vagotomy and pyloroplasty was commonly performed by open surgery, as the procedure is not time-consuming during open surgery.4–7 Due to the development of laparoscopic surgery combined with PPI treatment, and H. pylori eradication, patients now most commonly undergo primary repair only.8,9 However, additional treatments, such as vagotomy, may be required for patients who are currently receiving PPI treatment, who need continuous therapy with nonsteroidal anti-inflammatory drugs (NSAIDs), or who are expected to show poor compliance with ulcer treatment. Highly selective vagotomy (HSV) was first introduced clinically by Holle and Hart in 1967, 10 and laparoscopic HSV for patients with recurrent duodenal ulcer was reported by Dallemagne et al. in 1994. 11 However, laparoscopic surgery for ulcer perforation requires a long time to clean a wide range of contaminants, therefore, additional procedures, such as vagotomy, are burdensome. To shorten the operation time, posterior truncal vagotomy was developed along with seromyotomy and the Hill–Barker procedure.12–14
The aim of the present study was to compare the clinical and operative results between laparoscopic primary repair (LPR) alone or with HSV in patients with duodenal ulcer perforation. To the best of our knowledge, this is the first report of LPR with concurrent anterior and posterior HSV procedures in patients with duodenal ulcer perforation.
Patients and methods
Study population and ethical approval
The clinical data of patients who underwent LPR with or without HSV for duodenal ulcer perforation at either Changwon or Jinju Gyeongsang National University Hospital, between 2010 and 2020, were retrospectively collected from hospital records. The surgeons who performed the operations (SHJ, JHP and THK) were specialists in gastric cancer surgery with experience in performing such procedures.
The inclusion criteria for this study were as follows: (1) duodenal ulcer perforation and (2) laparoscopic primary repair and omental patching with or without HSV. Patients who underwent open conversion or combined gastrectomy were excluded. The indications for open conversion or combined gastrectomy were as follows: (1) unstable vital signs; (2) massive food contamination; (3) difficulty of the primary repair due to a large perforation size; and (4) concurrent antral infarction or perforation.
Data regarding the operation, postoperative complications, and treatment were collected by retrospective chart review after surgery, and all patient data were de-identified prior to data analysis.
All procedures described in this retrospective observational study were designed and conducted in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. The Institutional Review Board of Gyeongsang National University Hospital in Changwon, Korea approved the study (GNUH-IRB-2020-3-32) and waived the requirement of informed consent due to the retrospective study design. The reporting of this study conforms to STROBE guidelines. 15
Decision for HSV in patients with peptic ulcer
Patients with peptic ulcer were selected for HSV when they met the following criteria: (1) Stable vital signs and not showing symptoms of sepsis; (2) ongoing/or history of duodenal ulcer treatment; (3) high-risk of recurrent ulcers: patients who required continuous NSAID medication for underlying medical conditions or were current smokers; or (4) suspicion of noncompliance: high possibility of noncompliance or lack of self-care ability to receive follow-up or postoperative PPI medication (e.g., persons of extremely low socioeconomic status, disabled or bed-ridden patients, or individuals without a paid career).
Operative procedure
Each patient received general anaesthesia in the operating room. The patient was placed in a supine position, and the surgeon and scopist performed surgery from the right side of the patient (Figure 1). The assistant participated in the operation from the left side. In all cases, the first trocar port created the pneumoperitoneum using a Veress needle at the umbilicus. Ports were inserted in the following order: umbilicus 11 mm, right lower 11 mm, right upper 5 mm, and left upper 5 mm. The laparoscope used a flexible scope of 5 mm or 10 mm.
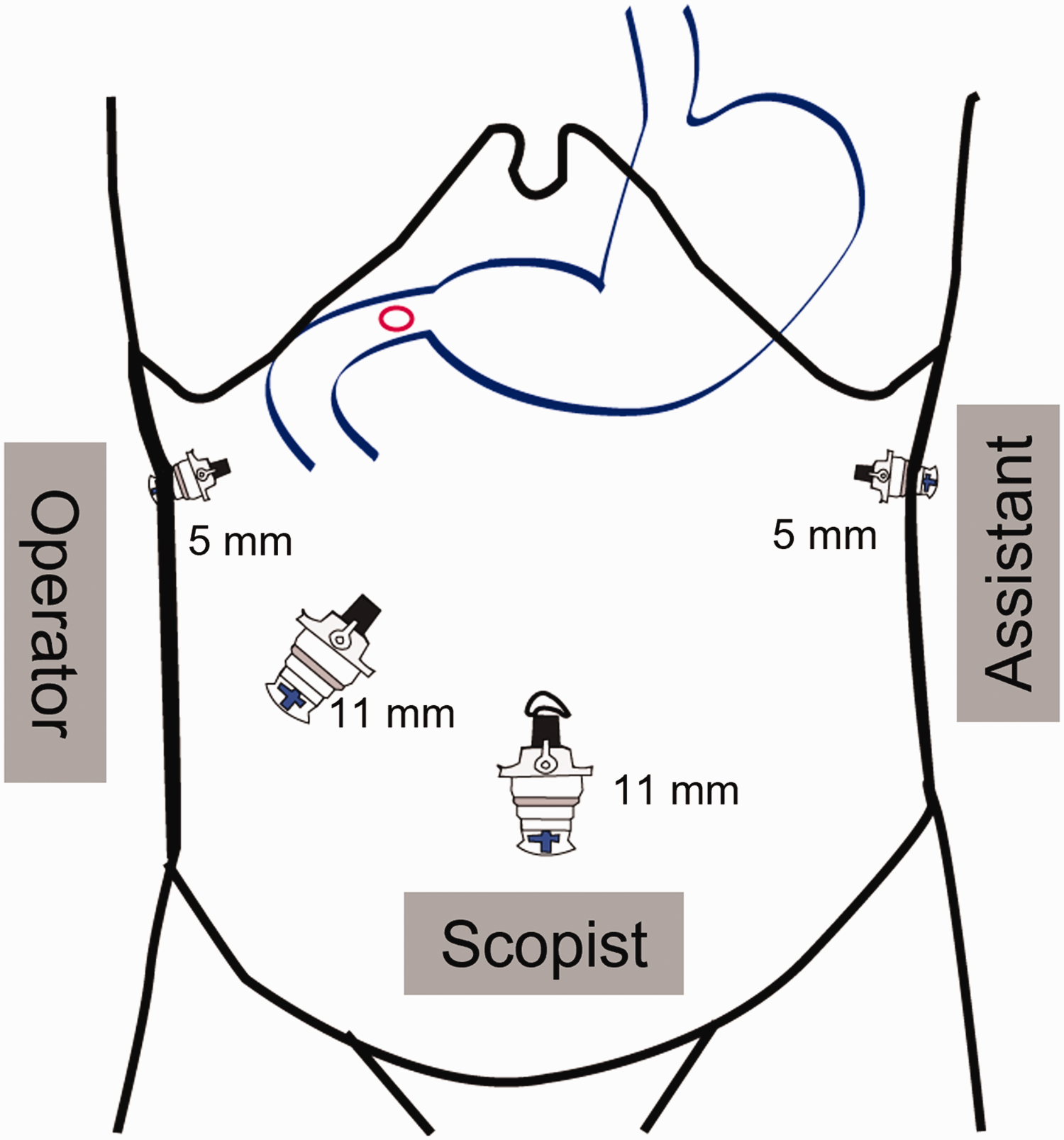
Port site and location of the operation team during laparoscopic primary repair alone or with highly selective vagotomy.
After inserting all of the ports, the degree of contamination and perforation in the abdominal cavity were observed. Stepwise images of the procedure are shown in Figure 2a–j. Continuous suturing was performed using V-loc (V-Loc™; Covidien, Mansfield, MA, USA) for duodenal ulcer perforation (Figure 2b and c). The detailed laparoscopic primary procedure, performed with a barbed suture at the present authors’ centre, has been described previously. 16 There was no risk of additional contamination after suturing of the perforation, and intraperitoneal irrigation was performed. Between 5 000 and 10 000 cc of sterile warm normal saline was used to clean the abdominal cavity.
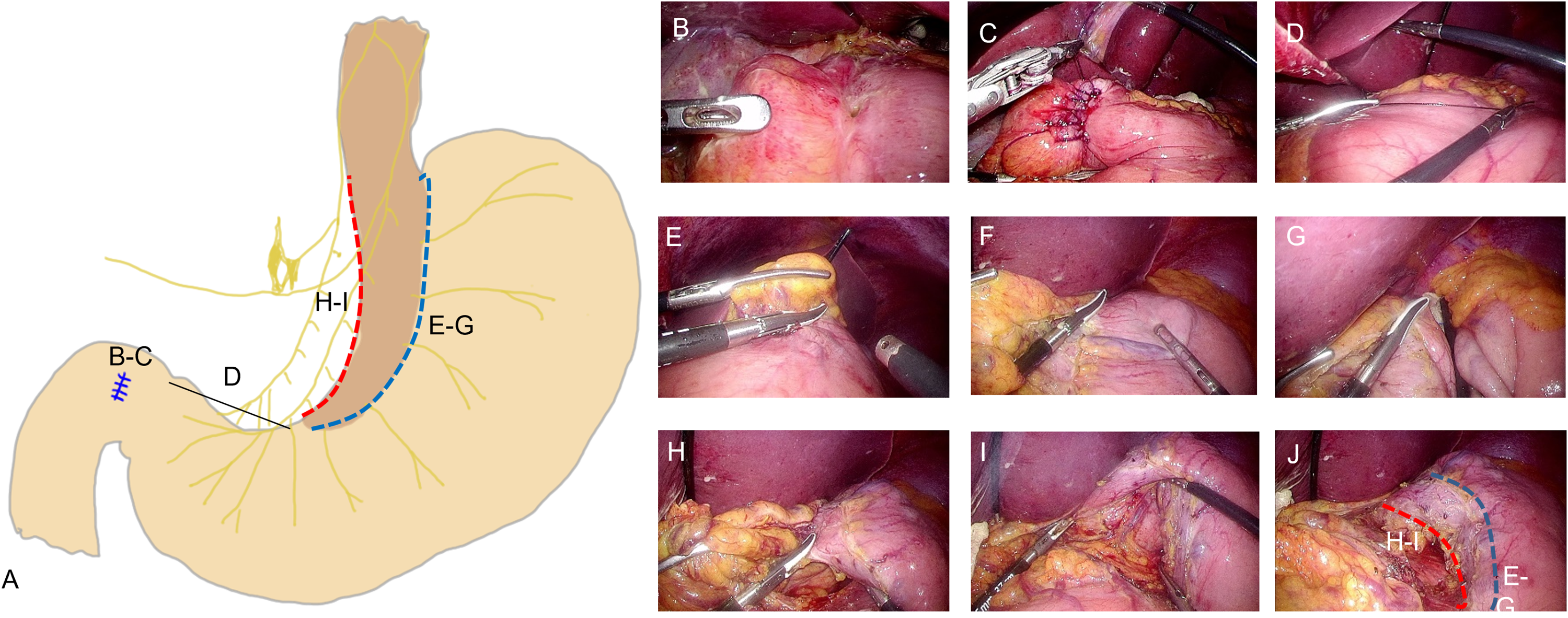
Illustration and stepwise images of laparoscopic primary repair with highly selective vagotomy, showing: (a) overall illustration; (b and c) continuous suture, performed using V-loc for duodenal ulcer perforation; (d) the saved 7 cm of the antrum area; (e–g) denervation of the anterior vagus nerve (blue dotted line on image 2A and 2J); (h–i) denervation of the posterior vagus nerve (red dotted line on image 2A and 2J); and (j) removal of the neurovascular bundle along the upper layer of the stomach muscle following anterior and posterior vagotomy.
HSV procedure
For the HSV procedure, 7 cm of the antrum from the pyloric ring was saved to spare pyloric and antral motility (Figure 2d), and vagotomy was performed 7 cm proximal to the pylorus and elongated near the gastroesophageal junction (GEJ). An ultrasonic device or a bipolar electrosurgical device was used to denervate the anterior vagus nerve (Figure 2a [e–g] and Figure 2j [e–g] blue dotted line) and the posterior vagus nerve (Figure 2a [h–i] and Figure 2j [h–i] red dotted line) of the proximal stomach (Figure 2a–j). During vagotomy, the anterior and posterior sides of the neurovascular bundle along the gastric subserosa layer must be removed (Figure 2j). While preserving the hepatic branch of the right vagus nerve, dissection was performed up to 5 cm above the GEJ of the right anterior oesophagus. Of note, it is important to check and cut the culprit nerve of Grassi running toward the upper posterior part of the stomach during this process (supplemental video 1). This technique is similar to lymphovascular bundle resection for laparoscopic gastric cancer surgery. Additional ligation of the left gastric artery with a surgical clip for bleeding prevention before HSV was performed according to the surgeon’s preference.
Intraoperative gastroscopy was then performed to check for strictures or leaks at the operation site. The omental patch was applied by suturing part of the greater omentum with a V-loc, and fixed with a surgical clip at the duodenal perforated area. The operation was finished after 3–4 surgically closed drain insertions. The surgical procedure is shown in the Supplemental Video.
Hospital course
A nasogastric tube was either not inserted, or if inserted, was removed before the surgery or after intraoperative gastroscopy. Sips of water were attempted between day 2 and 4 postoperatively, according to the degree of peritoneal inflammation. After 2 days of sipping water, the diet was advanced. Antibiotics were discontinued after infectious peritonitis had resolved, and the closed drain was removed after body fluid analysis. Patients were discharged when an advanced diet was tolerated without complications.
H. pylori eradication and antacid medication
The urea breath test (UBT) was performed at the emergency centre in all patients with a suspicion of peptic ulcer perforation. All patients who underwent surgical treatment were treated with PPIs postoperatively for 2 months, and if they were UBT positive, patients were treated with triple H. pylori therapy (PPI + clarithromycin/metronidazole + amoxicillin) for approximately 2 weeks starting before discharge, according to previously stated guidelines. 17 An endoscopy follow-up was recommended, performed 3–6 months after surgery, and if the results were Campylobacter-like organism (CLO) kit-positive, treatment was administered.
Statistical analyses
Data are presented as mean ± SD or n (%) prevalence. Statistical analyses were performed using SPSS Statistics software, version 24 (IBM SPSS, Inc., Armonk, NY, USA). Between-group differences in continuous variables were analysed by Student’s t-test or Mann–Whitney U-test and categorical variables were analysed by Fisher’s exact test or χ2-test, as appropriate. For analysis, missing data points were deleted. A P value <0.05 (two-sided) was considered statistically significant.
Results
Patient demographics
A total of 184 patients were enrolled. Of these, the duration of vagotomy was calculated by video review in 22 cases, and in 30 cases, data were missing and video recording was not possible, due to the volume of emergency surgeries at that time. No strictures or leaks at the operation site were observed during intraoperative gastroscopy.
The mean age of the study population was 49.6 ± 13.2 years, and the group comprised 146 male and 38 female patients (Table 1). The American Society of Anaesthesiologists (ASA) scores were as follows: 41 patients (22.3%); 107 patients (58.2%); 32 patients (17.4%); and four patients (2.2%) scored I, II, III, and IV, respectively. The operation was performed by laparoscopic primary repair with omental patch in 133 patients (71.7%) and by laparoscopic primary repair with omental patch and HSV in 52 patients (28.3%). The overall mean operation time was 98.4 ± 37 min and the mean procedure time for vagotomy was 17.8 ± 10.8 min. A soft fluid diet (SFD) was started at mean postoperative day 5.3 ± 3.5. The mean duration of hospital stay was 10.5 ± 6.3 days and the morbidity rate was 9.2% (17/184 patients). The most common reason for deciding to administer HSV was smoking history (28/52 patients [53.8%]), followed by ulcer treatment history (12/52 patients [23%]) (Table 1).
Demographics of 184 patients with duodenal ulcer perforation who underwent laparoscopic primary repair alone or with HSV.

Data presented as mean ± SD or n (%) prevalence.
ASA, American Society of Anesthesiologists; NSAID, nonsteroidal anti-inflammatory drug; HSV, highly selective vagotomy; SOW, sips of water; SFD, soft fluid diet.
Comparison of clinical and operative results between LPR alone and LPR plus HSV
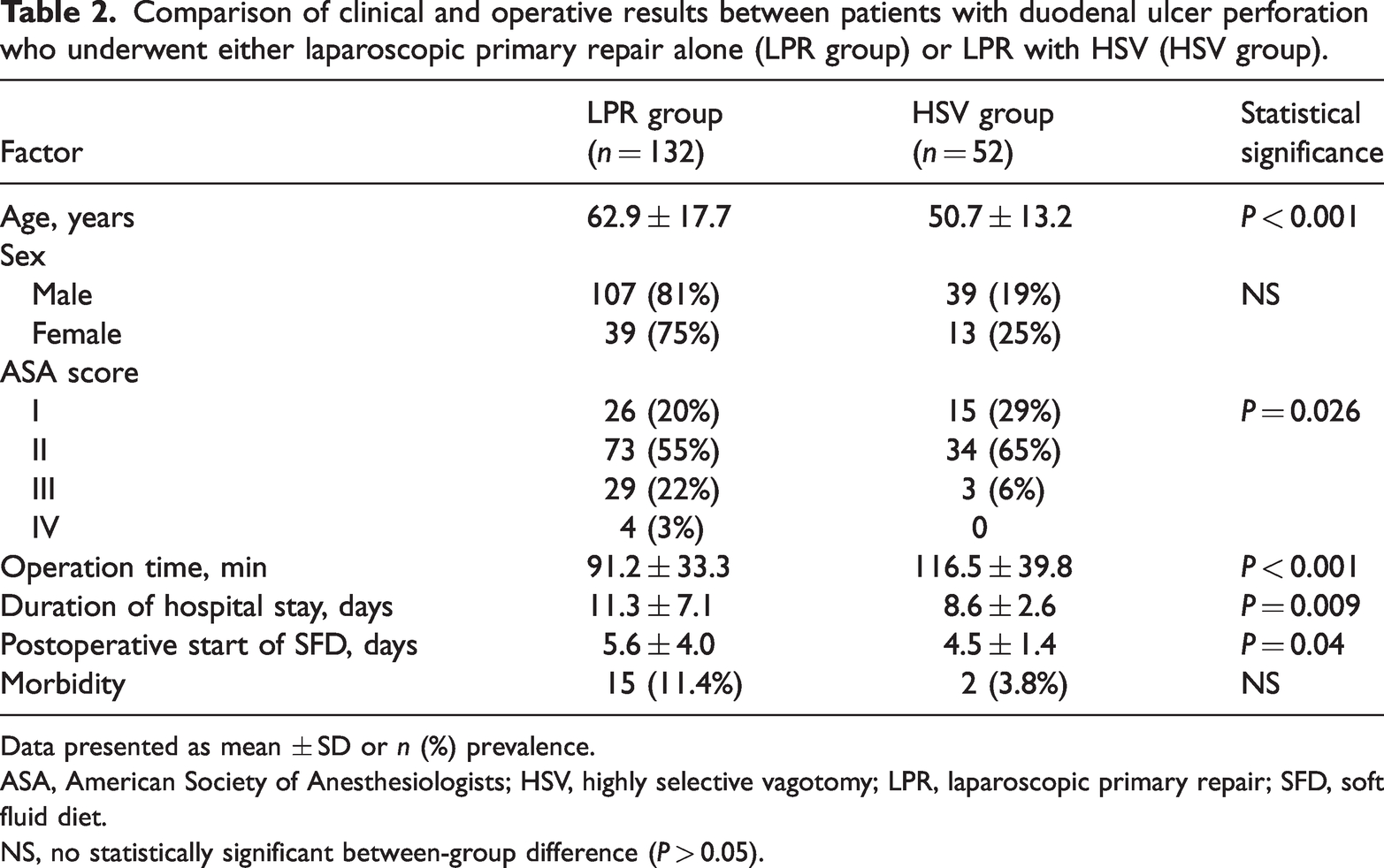
Patients who underwent HSV were significantly younger than those who underwent LPR alone (50.7 ± 13.2 versus 62.9 ± 17.7; P < 0.001; Table 2), but there was no between-group difference in the ratio of sexes (P = 0.419). There were significant between-group differences in ASA scores, with significantly more patients with an ASA score of III in the LPR alone group than in the HSV group, and significantly more patients with ASA scores of I and II in the HSV group (P = 0.026). The mean operation time was significantly longer in the HSV group (116.5 ± 39.8 min) than in the LPR group (91.2 ± 33.3 min; P < 0.001), and hospital stay was significantly shorter in the HSV group (8.6 ± 2.6 days versus 11.3 ± 7.1 days; P = 0.009). The mean postoperative day of starting SFD was also significantly shorter in the HSV group (4.5 ± 1.4 days) than in the LPR group (5.6 ± 4 days; P = 0.04).
Comparison of clinical and operative results between patients with duodenal ulcer perforation who underwent either laparoscopic primary repair alone (LPR group) or LPR with HSV (HSV group).
Data presented as mean ± SD or n (%) prevalence.
ASA, American Society of Anesthesiologists; HSV, highly selective vagotomy; LPR, laparoscopic primary repair; SFD, soft fluid diet.
NS, no statistically significant between-group difference (P > 0.05).
Two cases of morbidity were found in the HSV group and 15 cases in the LPR group, with no statistically significant between-group difference in morbidity rate (P = 0.158; Table 3). The most common complications were pulmonary complications (n = 5), fluid collection (n = 4), postoperative ileus (n = 3), and wound complications (n = 2).
Morbidity rates between patients with duodenal ulcer perforation who underwent either laparoscopic primary repair alone (LPR group) or LPR with HSV (HSV group).

Data presented as n prevalence.
LPR laparoscopic primary repair; HSV, highly selective vagotomy.
No statistically significant between-group differences (P > 0.05).
The study population exhibited a 35.4% (57/161) positive rate for H. pylori infection, which was diagnosed by preoperative UBT (9/131) and/or CLO test (51/133). H. pylori infection was treated by triple therapy in all patients.
Learning curve of the HSV procedure
The two operating surgeons each showed a stable operation time after 10 HSV operations (Figure 3). The HSV operation times were compared between the two surgeons based on a 10-case divide: surgeon 1 had 132 ± 35 min operation time for cases 1–10, which decreased to 95 ± 27 min for case 11 onwards (P = 0.003); and surgeon 2 took 164 ± 36 min for cases 1–10 and 100 ± 22 min for case 11 onwards (P < 0.0001).

Vagotomy learning curve for two surgeons (1 and 2) showing a stable procedure time each after operations in 10 cases each.
Discussion
The aim of the present study was to compare clinical and operative results between LPR alone and LPR with HSV in patients with duodenal ulcer perforation. The HSV group was found to show a significantly shorter hospital stay and mean postoperative day of starting SFD, but a longer operation time and no differences in morbidity compared with the LPR group. These results suggest that laparoscopic HSV is a safe and feasible procedure for selective cases who are at high risk of ulcer recurrence.
Patients with a high risk of ulcer recurrence need additional acid-reducing surgery. The present high-risk group was defined as patients with ongoing treatment/or treatment history for duodenal ulcer, current smoking, requirement of continuous NSAID, high possibility of noncompliance, or lack of self-care ability with their follow-up or postoperative PPI medication. Smoking causes an increase in gastric acid and affects mucosal defence mechanisms, causing peptic ulcer disease. Therefore, tobacco is a representative independent risk factor in patients with peptic ulcer, and ulcers take longer to heal in smokers compared with nonsmokers. 18 Additionally, smoking is associated with H. pylori infection, and continuous smoking increases H. pylori treatment failure rates. 19 Smoking cessation reduces the progression of peptic ulcers and increases healing,20,21 however, smoking is habit-forming and difficult to quit, so is considered a risk factor in ulcer recovery. NSAIDs quadruple the incidence of peptic ulcers.22,23 One patient in the present study was taking NSAIDs for continuous pain after left arm amputation, and presented with perforation even though he was taking a concurrent PPI. HSV was selected to treat this patient due to fewer complications and the ease of performing the procedure.
Due to its complexity, HSV is reported to be a difficult procedure to perform. To shorten the operation time, posterior truncal vagotomy was developed along with seromyotomy and the Hill–Barker procedure.11–14 Most modified procedures comprise posterior truncal vagotomy and anterior HSV to decrease the operation time. In East Asia, laparoscopic gastrectomy with lymph node detection has become the standard operation for early gastric cancer surgery.24,25 The present authors found that there was no technological difference between lymphadenectomy for early gastric cancer and vagotomy for peptic ulcer disease. With the development of ultrasonic devices and bipolar devices, laparoscopic dissection and bleeding control are now becoming relatively easy. Therefore, due to device development, procedures that were difficult in the past are now easily performed, even if the operator is not a gastric surgeon. A method of dissection of the subserosa layer of the stomach is used to dissect the bundle containing the lymphatics, vagus nerve, and left gastric artery and vein, along with the lesser curvature. In addition, to spare the motility of the antrum, dissection in the present study population was conducted 7 cm above the pylorus. 26
There are several technical tips for the safe performance of HSV; whenever laparoscopic subserosal dissection is performed, meticulous small-bite dissection using an energy device is a prerequisite for preventing oesophageal and gastric wall damage. Perigastric perforating small vessels should be easily identified at the same time during this process, to reduce bleeding. In addition, clipping of the left gastric artery first is recommended to reduce bleeding if excessive bleeding occurs during the dissection procedure. Liver retraction must be performed with a retractor or the same method performed in laparoscopic curative surgery for gastric cancer, which is convenient for exposure around the GEJ and accurate vagotomy.27,28 Intraoperative gastroscopy is an essential procedure after primary repair of duodenal ulcers, to check the stability of the suture area and the passage and mobility of the pyloric area, and this procedure may prevent serious postoperative complications, such as leakage and pyloric stenosis. 29 If a problem is found, an additional suture or laparoscopic gastrojejunostomy can be performed. Laparoscopic surgery for ulcer perforation requires a long duration for peritoneal lavage to clean a wide range of contaminants, so additional procedures, such as vagotomy, are burdensome. Additionally, for primary repair, interrupted suturing of the perforation site requires considerable surgical time for the beginner. However, in previous studies, operating times have been reduced from an average of 131 minutes to 87 minutes by performing continuous suturing using a barbed suture. 16 Thus, the present authors saved time for performing additional HSV procedures on patients in the high-risk group for ulcer recurrence. Both surgeons in the present study reduced the mean operation time to less than 100 minutes after performing the procedure in 10 cases each, suggesting that the procedure would be easy to implement if a surgeon is familiar with laparoscopic gastrectomy techniques.
The present results may be limited by several factors. The investigation was a retrospective study and included a relatively small number of cases. The results may be subject to selection bias, due to more severe and unstable patient cases in the LPR alone group than LPR with HSV group. A long-term follow-up study with a larger sample size is necessary to validate the present results, which the present authors plan to conduct in the future. To the best of our knowledge, this is the first report of laparoscopic primary repair with concurrent anterior and posterior HSV procedures performed in patients with duodenal ulcer perforation. Additionally, the study provided evidence of the long-term effect of HSV in open surgery.
In conclusion, although LPR plus HSV showed a significantly longer operation time, LPR plus HSV was associated with a shorter hospital stay and mean postoperative duration to starting SFD, with no differences in morbidity, compared with LPR alone. Laparoscopic HSV may be a safe and feasible procedure for selective cases who are at high risk for ulcer recurrence.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605231206319 - Supplemental material for Concurrent laparoscopic highly selective vagotomy with closure of duodenal ulcer perforations show good clinical results as primary repair alone
Supplemental material, sj-pdf-1-imr-10.1177_03000605231206319 for Concurrent laparoscopic highly selective vagotomy with closure of duodenal ulcer perforations show good clinical results as primary repair alone by Ji-Ho Park, Jin‑Kwon Lee, Dong-Hwan Kim, Jae-Seok Min, Tae-Han Kim, Eun-Jung Jung, Taejin Park, Jae Yool Jang, Jung-Woo Woo, Han Shin lee, Miyeong Park and Sang-Ho Jeong in Journal of International Medical Research
Supplemental Material
sj-mp4-2-imr-10.1177_03000605231206319 - Supplemental material for Concurrent laparoscopic highly selective vagotomy with closure of duodenal ulcer perforations show good clinical results as primary repair alone
Supplemental material, sj-mp4-2-imr-10.1177_03000605231206319 for Concurrent laparoscopic highly selective vagotomy with closure of duodenal ulcer perforations show good clinical results as primary repair alone by Ji-Ho Park, Jin‑Kwon Lee, Dong-Hwan Kim, Jae-Seok Min, Tae-Han Kim, Eun-Jung Jung, Taejin Park, Jae Yool Jang, Jung-Woo Woo, Han Shin lee, Miyeong Park and Sang-Ho Jeong in Journal of International Medical Research
Footnotes
Author contributions
SH Jeong, JH Park and JK Lee wrote the main manuscript text; JS Min, TH Kim and EJ Jung collected and analysed the data; TJ Park, JK Lee, JY Jang and JW Woo supervised the study and analysed data; and HS Lee and MY Park prepared Figures 1–![]() . All authors reviewed the manuscript.
. All authors reviewed the manuscript.
Data availability statement
The datasets generated during and/or analysed during this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.