
Abstract
Background
Anemia can negatively affect the outcome of many diseases, including infections and inflammatory conditions.
Aim
To compare the prognostic value of hemoglobin level and the neutrophil/lymphocyte ratio (NLR) for prediction of coronavirus disease 2019 (COVID-19) severity.
Methods
In this retrospective cohort study, clinical data from patients with laboratory-confirmed COVID-19 were collected from hospital records from 10 April 2020 to 30 July 2020.
Results
The proportions of patients with mild, moderate, and severe COVID-19 differed significantly in association with hemoglobin levels, neutrophil counts, lymphocyte counts, NLR, and total leukocyte counts. Patients with severe COVID-19 had significantly lower hemoglobin levels than those with moderate or mild COVID-19. There were statistically significant negative associations between hemoglobin and D-dimer, age, and creatinine. The optimal hemoglobin cut-off value for prediction of disease severity was 11.6 g/dL. Using this cut-off value, hemoglobin had higher negative predictive value and sensitivity than NLR (92.4% and 51.3%, respectively). The specificity of hemoglobin as a prognostic marker was 79.3%.
Conclusion
Both NLR and hemoglobin level are of prognostic value for predicting severity of COVID-19. However, hemoglobin level displayed higher sensitivity than NLR. Hemoglobin level should be assessed upon admission in all patients and closely monitored throughout the disease course.
Keywords
Introduction
The current pandemic of coronavirus disease 2019 (COVID-19) has affected countries all over the world. 1 Inflammation plays a crucial role in the pathogenesis of COVID-19: the cytokine storm that occurs in patients with severe disease can result in multiorgan failure and death. This hyper-inflammatory condition is associated with high level of inflammatory markers such as C-reactive protein (CRP), interleukin (IL)-6, and ferritin.2,3
White blood cells (monocytes, lymphocytes, and neutrophils) play vital roles in the systemic inflammatory responses underlying multiple conditions such as infection, trauma, and shock. 4 The neutrophil-to-lymphocyte ratio (NLR) is obtained by dividing the neutrophil count by the lymphocyte count. 5 The NLR is a marker of the systemic inflammatory response and has been validated as a prognostic marker in various disorders including cardiac conditions, solid tumors, sepsis, pneumonia, and acute respiratory distress syndrome.6,7
Inflammation is characterized by distinctive modifications of iron homeostasis. During inflammation there is an increase in iron acquisition and retention inside macrophages and a decrease in its absorption from the intestine. 8 Consequently, there is a reduction in circulating levels of iron and in the availability of this essential mineral for erythropoiesis and hemoglobin production. Moreover, cytokines released during the inflammatory response result in further inhibition of erythropoiesis, shortening of the erythrocyte half-life, and reduced activity of the erythropoietin hormone. All of these changes contribute to the development of anemia. 9 Anemia negatively impacts the outcome of many diseases, including infections and inflammatory conditions.10–14 Anemia is commonly associated with poor prognostic outcomes and a higher risk of mortality among patients with respiratory diseases including community-acquired pneumococcal pneumonia.15,16
Several studies have found that severe COVID-19 (including fatal cases) was associated with higher neutrophil counts, lower lymphocyte counts, and higher neutrophil/lymphocyte ratios (NLRs) compared with non-severe disease. 17 Moreover, it has been reported that anemia and changes in iron homeostasis were exacerbated in hospitalized COVID-19 patients and that hemoglobin can contribute to risk stratification of patients. Patients suffering from anemia at the beginning of the disease course were proposed to have higher risk of mortality. 18
The present study aimed to compare the prognostic value of hemoglobin level and the NLR for prediction of COVID-19 severity.
Methodology
The study protocol was approved by the Ain Shams University Faculty of Medicine Research Ethics Committee (REC) (approval number FWA 00017585).
Patients and setting
This was a retrospective cohort study. Clinical data for patients with laboratory-confirmed COVID-19 were collected from the El-Obour Ain Shams University Isolation Hospital from 10 April 2020 to 30 July 2020. Comorbidities such as diabetes mellitus or hypertension, intensive care unit (ICU) admission, and treatments received were documented. The study followed the STROBE Guidelines. 19
All included patients had laboratory-confirmed COVID-19 using reverse transcription polymerase chain reaction (RT-PCR). The patients were divided into three groups based on disease severity according to the Ain Shams University Hospitals Consensus Statement on Management of Adult COVID-19 Patients. 20 Mild COVID-19 was defined as patients who were either: (i) asymptomatic with abnormal laboratory findings (D-dimer <1 mg/L, absolute white blood cell count <800/μL, ferritin <500 ng/mL, liver function within normal) or computed tomography (CT) findings of COVID-19 pneumonia, or (ii) symptomatic with no CT findings of COVID-19 pneumonia. Moderate COVID-19 was defined as patients who were symptomatic with clinical signs of non-severe pneumonia (e.g., fever, cough, dyspnea) as well as CT findings of COVID-19 pneumonia and/or abnormal laboratory findings. Severe COVID-19 was defined as patients with clinical signs of severe pneumonia (e.g., respiratory rate > 30 breaths/minute, severe respiratory distress, or SpO2 <93% on room air) and CT findings of COVID-19 pneumonia.
The data collected and analyzed in the current study included sociodemographic data, detailed medical and drug history, presence of co-morbidities, and laboratory investigations. Laboratory investigations included complete and differential blood cell count, blood group, CRP level, serum D-dimer level, ferritin level, liver function tests, and kidney function tests.
CT protocol and grading
Chest CT scans were performed with a single inspiratory phase using a commercial multi-detector CT scanner (Activion™ 16 Multislice CT System, Toshiba, Tokyo, Japan.). Patients were asked to hold their breath to decrease motion-induced artifacts. CT images were taken using the following parameters: tube voltage, 100 to 120 kVp; effective tube current, 110 to 250 mAs; detector collimation, 0.625 mm; slice thickness, 1 mm; and slice interval, 0.8 mm. Typical CT findings included ground-glass opacities, consolidation, crazy-paving, cavitation, mediastinal lymphadenopathy, and pleural effusion. Radiological severity was determined using the method developed by Chung and collaborators. 21 The number of involved lung lobes and the distribution of lesions were also used to assess radiological severity.
Each lung lobe was assessed using the following scoring system: 0, no involvement (0%); 1, minimal involvement (1%–25%); 2, mild involvement (26%–50%); 3, moderate involvement (51%–75%); and 4, severe involvement (76%–100%). A total score was obtained by summing the five lobe scores (range of possible scores: 0–20). The severity of lung involvement on CT scans was classified on a 4-point ordinal scale: grade 0, score 0 (no abnormalities present on CT); grade 1, score 1 to 5; grade 2, score 6 to 15; grade three, score 16 to 20.
Statistical analysis
Data were processed, coded, then analyzed using IBM SPSS for Windows Version 20.0 (IBM Corp., Armonk, NY, USA). Qualitative data were presented as frequencies and percentages. Quantitative data were presented as means and standard deviations (SDs). An independent sample t-test or Mann–Whitney U test was used to assess differences between the means of two groups. Analysis of variance or the Kruskal–Wallis test were used to assess differences among quantitative variables with three categories. The chi-square or Fisher's exact test were used to assess differences between qualitative variables. Values of p < 0.05 were considered statistically significant.
Results
From 10 April 2020 to 30 July 2020, 338 patients were admitted to El-Obour Ain Shams University Specialized Hospital for Isolation (Table 1). Among them, 323 (95.6%) tested positive for COVID-19 by RT-PCR. However, patients with negative RT-PCR results had CT findings suggestive of COVID-19. Of the 338 patients, 189 (55.9%) had mild COVID-19, 109 (32.2%) had moderate COVID-19, and 40 (11.8%) had severe COVID-19. The mean age of patients was 46.8 years (SD 16.24 years, range: 10–85 years). Of the 338 patients, 182 (53.8%) were male and 156 (46.2%) were female. Only 25 (7.4%) were smokers while 110 (32.5%) were healthcare workers. Most patients (316, 93.5%) reported contact with a confirmed COVID-19 case before diagnosis and hospital admission. The most common comorbidities were hypertension (69 patients, 20.4%), diabetes mellitus (59 patients, 17.5%), and chronic kidney disease (25 patients, 7.4%). Only two patients (0.6%) had compensated liver cirrhosis. Fever was the most common presenting symptom (135 patients, 39.9%) followed by dyspnea (133 patients, 39.3%). Table 1 summarizes complete blood counts and kidney function tests. Hemoglobin levels ranged from 6.9 to 17.3 g/dL (mean ± SD 12.70 ± 1.93 g/dL). The median neutrophil count was 3.88 × 103/µL (range: 2.7–5.7 × 103/µL), the median lymphocyte count was 1.47 × 103/µL (range: 0.9–2.08 × 103/µL), and the median NLR was 2.52 (range: 1.45–5.5).
Characteristics of patients with COVID-19 including complete blood counts, kidney function tests, and radiological severity on admission.

COVID-19: coronavirus disease 2019; PCR, polymerase chain reaction; DM, diabetes mellitus; CLD, chronic liver disease; CKD, chronic kidney disease; CRP, C-reactive protein; CT, computed tomography; SD, standard deviation; IQR, interquartile range; FEU, fibrinogen equivalent units.
In terms of radiological severity, 168 (49.7%) patients had grade 0 severity scores indicating no abnormalities present on CT. Five patients (1.5%) had grade 1 severity scores, 160 (47.3%) had grade 2 severity scores, and five (1.5%) had grade 3 severity scores (Table 1).
Table 2 summarizes correlations between different complete blood count parameters and COVID-19 severity (mild, n = 189; moderate, n = 109; severe, n = 40). There were statistically significant differences between patients with mild, moderate, and severe COVID-19 in terms of hemoglobin levels, neutrophil counts, NLR, and total leukocyte counts (p < 0.001, p = 0.009, p = 0.002, and p = 0.006, respectively). Patients with severe COVID-19 had significantly lower hemoglobin levels than those with moderate or mild COVID-19. Patients with severe COVID-19 had significantly higher neutrophil counts, total leukocyte counts, and NLRs than patients with moderate or mild COVID-19. In addition, patients with mild COVID-19 had significantly higher levels of lymphocytes than both patients with moderate and severe COVID-19 (p = 0.021).
Correlations between complete blood count parameters and COVID-19 severity (mild, moderate, and severe).

*: Chi-square test; •: One way analysis of variance; ‡: Kruskal–Wallis test.
COVID-19, coronavirus disease 2019; SD, standard deviation; IQR, interquartile range; FEU, fibrinogen equivalent units.
Table 3 summarizes correlations between different complete blood count parameters and disease severity (group 1, mild or moderate COVID-19, n = 289; group 2, severe COVID-19, n = 40). There were statistically significant differences between group 1 and 2 patients in terms of hemoglobin levels, neutrophil counts, NLR, and total leukocyte counts (p < 0.001, p = 0.004, p = 0.013, and p = 0.002, respectively). Patients with severe COVID-19 had significantly lower hemoglobin levels than those with mild or moderate COVID-19. Patients with severe COVID-19 had significantly higher neutrophil counts, total leukocyte counts, and NLRs than those with moderate or mild COVID-19. There was no significant difference in lymphocyte count between the two groups.
Correlations between complete blood count parameters and COVID-19 severity (mild or moderate vs. severe).

COVID-19, coronavirus disease 2019; SD, standard deviation; IQR, interquartile range; FEU, fibrinogen equivalent units.
Negative correlations were observed between hemoglobin and CRP, D-dimer, age, monocyte count, and creatinine. However, only the correlations between hemoglobin and age, D-dimer, and creatinine reached statistical significance (Table 4 and Figures 1, 2 and 3).
Correlations between hemoglobin level and CRP, ferritin, D-dimer, age, complete blood count parameters and kidney function tests.

*: Chi-square test; •: One way analysis of variance; ‡: Kruskal–Wallis test.
CRP, C-reactive protein; FEU, fibrinogen equivalent units.

Correlation between hemoglobin level and D-dimer level. Hemoglobin level was inversely correlated with D-dimer level. As the D-dimer level increased there was a corresponding significant decrease in the hemoglobin level.
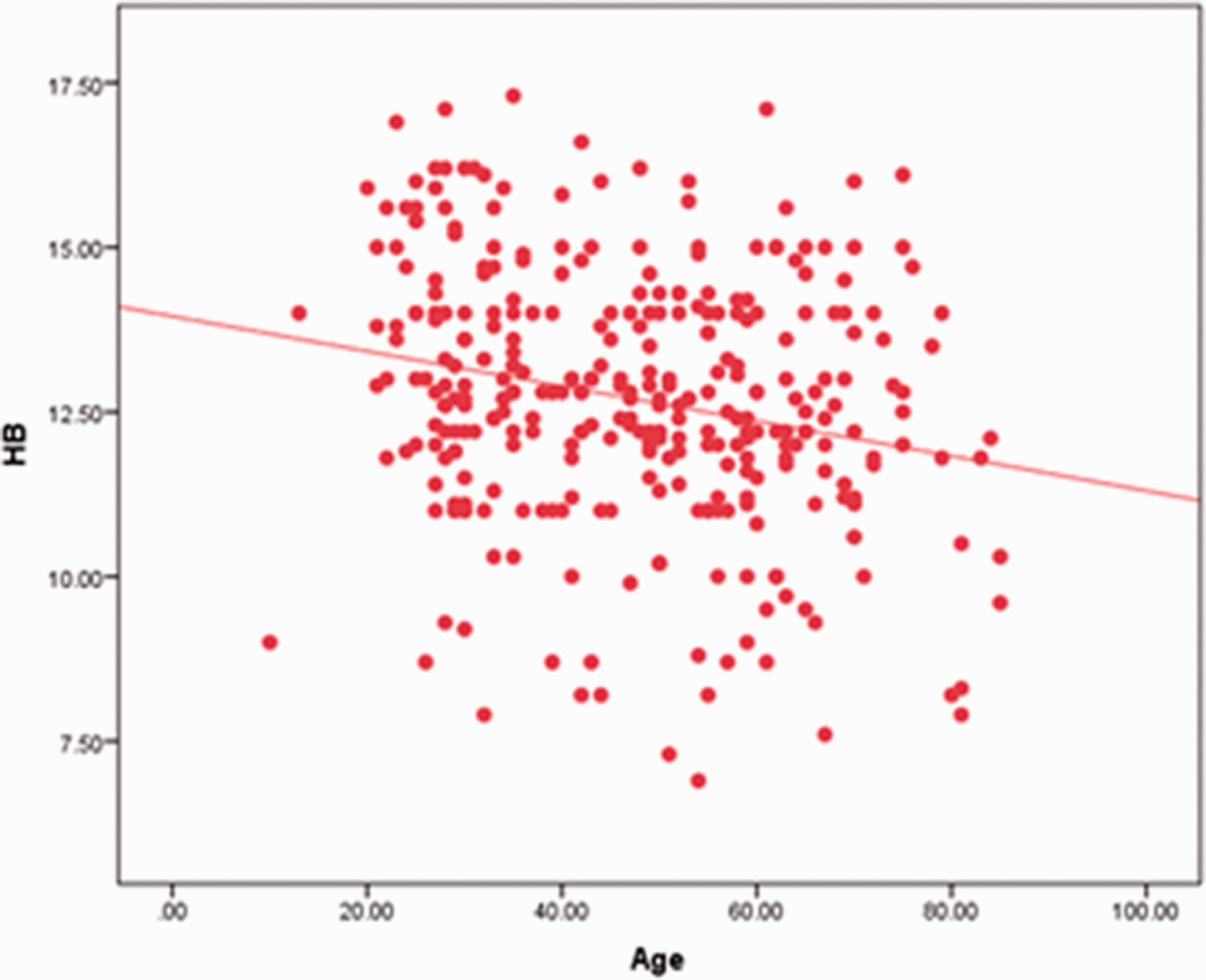
Correlation between hemoglobin level and age. Hemoglobin level was inversely correlated with age. As age increased there was a corresponding decrease in hemoglobin level.

Correlation between hemoglobin level and creatinine level. Hemoglobin level was inversely correlated with creatinine level. As the creatinine level increased there was a corresponding decrease in the hemoglobin level.
The optimal cut-off value of hemoglobin was identified as 11.6 g/dL with an area under the curve (AUC) of 0.663. Using this cut-off, hemoglobin had a sensitivity of 51.28%, a specificity of 79.31%, and a negative predictive value of 92.4% for prediction of COVID-19 severity (Table 5 and Figure 4). The optimal cut-off value for neutrophil count was 4.0429 with an AUC of 0.644. The optimal cut-off value for lymphocyte count was 1.4750 with an AUC of 0.535. The optimal cut-off value of the NLR was 7.53 with an AUC of 0.644. Using this cut-off, the NLR had a sensitivity of 34.62%, a specificity of 87.21%, and a negative predictive value of 89.8% for prediction of COVID-19 severity (Table 5 and Figure 5).
Summary of receiver operating characteristic curve analysis of potential prognostic factors for mild/moderate vs. severe COVID-19.

COVID-19, coronavirus disease 2019; AUC, area under the curve; PPV, positive predictive value; NPV, negative predictive value; NLR, neutrophil to lymphocyte ratio.

Receiver operating characteristic curve of hemoglobin level as a predictor of COVID-19 severity (mild/moderate or severe).

Receiver operating characteristic curve of the neutrophil to lymphocyte ratio as a predictor of COVID-19 severity (mild/moderate or severe).
Discussion
The immune system plays a major role in combating viral infections. White blood cell populations (monocytes, lymphocytes, and neutrophils) are cornerstones in the systemic inflammatory response and can be used as indicators of the severity of the immune response. These parameters are easily measurable, widely available, cost-effective, and reliable. 4 Neutrophilia and lymphocytopenia are physiological responses of the innate immune system to systemic inflammation. These processes lead to elevation of the NLR.22,23 Hence, the NLR reflects the systemic inflammatory response and is associated with poor prognosis of infectious diseases.7,23 Anemia usually exacerbates the severity of respiratory diseases. Few studies have assessed the prognostic value of hemoglobin level for predicting COVID-19 severity. The present study aimed to compare the prognostic value of hemoglobin level and the NLR for prediction of COVID-19 severity.
The current study included 338 patients admitted to hospital with positive RT-PCR tests for COVID-19. Most patients were non-smokers, with a slight female over-representation. Most patients were not diabetic or hypertensive. Most patients had mild or moderate COVID-19 with CT grades between 0 and 2. We observed highly significant positive relationships between COVID-19 severity and neutrophil levels, total leukocyte counts, NLR, and hemoglobin levels. We also observed a significant negative association between lymphocyte levels and COVID-19 severity. Hemoglobin was significantly negatively associated with age, D-dimer, and creatinine.
Multiple studies have proposed that lymphopenia could be of significant prognostic value in predicting COVID-19 severity.24–27 The results of several previous studies agree with the data reported here, showing that severe COVID-19 (including fatal cases) was associated with higher neutrophil counts and lower lymphocyte counts compared with mild or moderate COVID-19.28–30 Wang and collaborators conducted a retrospective study of 131 patients with a median age of 64 years; among those patients, 12 (9.2%) died in hospital. Their study revealed that NLR on admission was significantly higher among non-survivors compared with survivors (p < 0.001). A NLR of 3.338 was linked to a higher risk of mortality; using this cut-off, NLR showed a sensitivity of 100.0% and a specificity of 84%. 7
Similar results were obtained by Qun and collaborators. They proposed that NLR was a rapid, effective marker of inflammation and was significantly predictive of COVID-19 course and severity. 23 The findings of Sayed and co-workers agreed with our results and showed that NLR was of prognostic value in COVID-19 patients and should thus be closely monitored. 28
The occurrence of neutrophilia, lymphocytopenia, and elevated NLR in patients with COVID-19 could be attributed to expression of angiotensin-converting enzyme 2, the primary receptor for causative virus of COVID-19, on lymphocytes, resulting in their infection and loss. 31 Loss of immune cells increases the risk of bacterial infection, leading to an increase in neutrophil count. 32 Because the cytokine storm plays a crucial role in the pathogenesis of COVID-19, cytokines including IL-10, IL-6, and tumor necrosis factor-α may trigger neutrophil activation and proliferation as well as lymphocyte apoptosis and destruction of lymphatic tissue.33–35
In patients with COVID-19, inflammation is characterized by distinctive modifications of iron homeostasis and erythropoiesis that lead to the development of anemia. 9 Several studies have assessed links between anemia and COVID-19 severity or mortality. Potential associations may result from decreased oxygen delivery to the tissues along with anemia as well as the presence of comorbidities such as impaired kidney function, older age, or advanced inflammation.9,36 With COVID-19 progression and an increase in viral replication, impairment of the epithelial–endothelial barrier occurs and results in exacerbation of the inflammatory response, activation of coagulation, and depletion of clotting factors. Subsequently, D-dimer levels become elevated.37,38
A few retrospective cohort studies showed that patients suffering from anemia were prone to severe COVID-19 and had higher mortality rates.18,39–41 Dinevari and collaborators conducted a prospective study of 1274 hospitalized patients with COVID-19 in Iran to investigate associations between anemia and patient outcomes. Their results showed that anemia was more prevalent among older patients (p = 0.02) and among patients with chronic kidney disease (p < 0.05). The mortality rate of anemic patients was 23.9% compared with 13.8% in nonanemic patients. The percentage of anemic patients requiring ICU admission was 27.8% compared with 14.7% of nonanemic patients (p < 0.001). Regression analysis showed that low hemoglobin was independently associated with mortality (odds ratio [OR] 1.68, 95% confidence interval [CI]: 1.10–2.57, p = 0.01) and probability of ICU admission (OR 2.06, 95% CI: 1.46–2.90, p < 0.001). Moreover, they identified negative correlations between anemia and both age and chronic kidney disease (p = 0.02 and p < 0.001). 40
In contrast, Yang and collaborators performed a study to describe the clinical picture and outcomes of critically ill patients with COVID-19 and found no correlation between low hemoglobin levels and mortality risk. 27 This discrepancy with the current results could be attributed to the small sample size of this study (52 patients) and differences between the study populations. The study of Yang and colleagues included only critically ill patients and they did not investigate the prognostic value of hemoglobin level among non-critically ill patients.
The present study is the first to compare the prognostic value of neutrophil counts, NLR, D-dimer level, and hemoglobin level in predicting COVID-19 severity. The optimal cut-off value of hemoglobin level was identified as ≤11.6 g/dL. Using this value, hemoglobin level had higher sensitivity and lower specificity than the NLR and a negative predictive value of 92.4%
Our study had some limitations. First, it was a retrospective study, and we did not assess alterations in the hemoglobin levels of patients with COVID-19 prospectively over the course of the disease. Second, most patients included in the study had mild or moderate disease. Third, data on hemoglobin levels prior to COVID-19 onset were not available. Fourth, we did not investigate erythropoietin levels, serum iron levels, transferrin levels, or transferrin saturation ratio.
Conclusion
Both NLR and hemoglobin level are prognostic of COVID-19 severity. However, hemoglobin level displayed higher sensitivity than NLR. Hemoglobin level should be assessed on admission in patients with COVID-19 and closely monitored over the disease course.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors’ contributions
MFA, SHF, and MM designed the study. SIT, SHF, MM, AH, and SWR performed sample collection. AAO performed the analysis and grading of CT images. MFA performed the statistical analysis. SHF and MFA wrote the draft of the manuscript. SWR performed critical review of the manuscript. All authors reviewed and approved the final version. All authors read and approved the final manuscript.
Availability of data and materials
All the data needed to support the study findings are found in the manuscript.
Consent for publication
Not applicable.