
Abstract
A De Garengeot hernia is a rare type of femoral hernia that involves a vermiform appendix within a femoral hernia sac. Because of the rarity of this disease, a standard surgical procedure has not been established, and most cases are diagnosed intraoperatively. Preoperative diagnosis of a De Garengeot hernia is quite difficult. Computed tomography is the most sensitive and specific technique among the available imaging tests for preoperative diagnosis of a De Garengeot hernia. Although a standard surgical procedure is lacking, prompt surgery has become the consensus. The most common procedure is the open anterior approach; this allows exploration of the hernia sac and rapid treatment of its contents, routine appendectomy through a single incision, and preperitoneal repair of the femoral hernia.
Introduction
Femoral hernias represent 3% to 4% of all groin hernias. Among femoral hernias, 0.5% to 5.0% involve a vermiform appendix within the femoral hernia sac. Such hernias are termed De Garengeot hernias, named after Rene Jacques Croissant De Garengeot (1688–1759), a Parisian surgeon who first described the rare phenomenon in 1731. 1 Fewer than 200 cases have been reported to date. These hernias show a female preponderance, with a male-to-female ratio of 1:5.2,3 Computed tomography has certain diagnostic value, but most cases are diagnosed intraoperatively. Accurate preoperative diagnosis can assist the surgeon in evaluation of the risk and difficulty of surgery and selection of the most appropriate surgical method and approach. In this way, the operation time can be shortened, the incidence of postoperative complications can be reduced, and the severity of pain may be alleviated. We herein present an unusual case involving a 69-year-old man who presented with an incarcerated right femoral hernia containing a purulent appendix and describe our surgical management of this hernia.
Case report
A 69-year-old man with 1-year history of a retractable mass in the right groin arrived at our emergency department with a 5-day history of progressively aggravated right inguinal pain associated with the appearance of an incarcerated right femoral hernia. He denied abdominal pain and distension, nausea and vomiting, fever, and any other signs of bowel obstruction. He had no other relevant medical history. His vital signs were normal, and his body mass index was 18.0 kg/m2. Physical examination revealed a non-reducible tender lump in the right groin below the level of the right inguinal ligament. The lump was approximately 6 × 4 cm in size, warm, and erythematous. Routine blood examination revealed a white cell count of 8.62 × 109/L and neutrophilic granulocyte percentage of 75.7%. A computed tomography scan revealed a quasi-circular hypodense lesion of approximately 6.0 × 4.0 × 4.0 cm located medial to the right femoral vessels and connected to the abdominal intestines (Figures 1–3). There were no signs of intestinal obstruction.

Computed tomography revealed a quasi-circular hypodense lesion of approximately 6.0 × 4.0 × 4.0 cm located medial to the right femoral vessels.

Computed tomography revealed a quasi-circular hypodense lesion of approximately 6.0 × 4.0 × 4.0 cm located medial to the right femoral vessels.

Computed tomography revealed a quasi-circular hypodense lesion of approximately 6.0 × 4.0 × 4.0 cm located medial to the right femoral vessels.
The patient was preoperatively diagnosed with a right incarcerated inguinal hernia and taken to the operating room for surgery under general anesthesia after providing written consent for treatment. Preoperative prophylactic antibiotics were administered. An oblique incision was made above the inguinal ligament in the right groin, and an anterior approach was performed. Dissection in layers revealed an incarcerated right femoral hernia under the inguinal ligament, and the hernia could not be reduced from below. The peritoneum was dissected through Hesselbach’s triangle, revealing a non-reducible appendix in the femoral canal without signs of peritonitis. The tip of the appendix was purulent and swollen. After yellow-white purulent fluid was extracted by fine needle puncture from the hernia sac, the tip of the appendix was still unable to be reduced because the femoral ring was narrow and the tip of the appendix was purulent and swollen. We cut off the inguinal ligament and then raised the hernia sac and appendix (Figures 4 and 5). Open appendicectomy was performed, and the right femoral hernia sac was resected. We closed the peritoneum with absorbable suture and repaired the hernia by suturing the conjoint tendon to Cooper’s ligament with PDS-II suture. The inguinal ligament was then repaired using PDS-II suture. Finally, a negative-pressure drainage tube was placed in the inguinal canal.

The inguinal ligament was cut off and the hernia sac and appendix were raised.
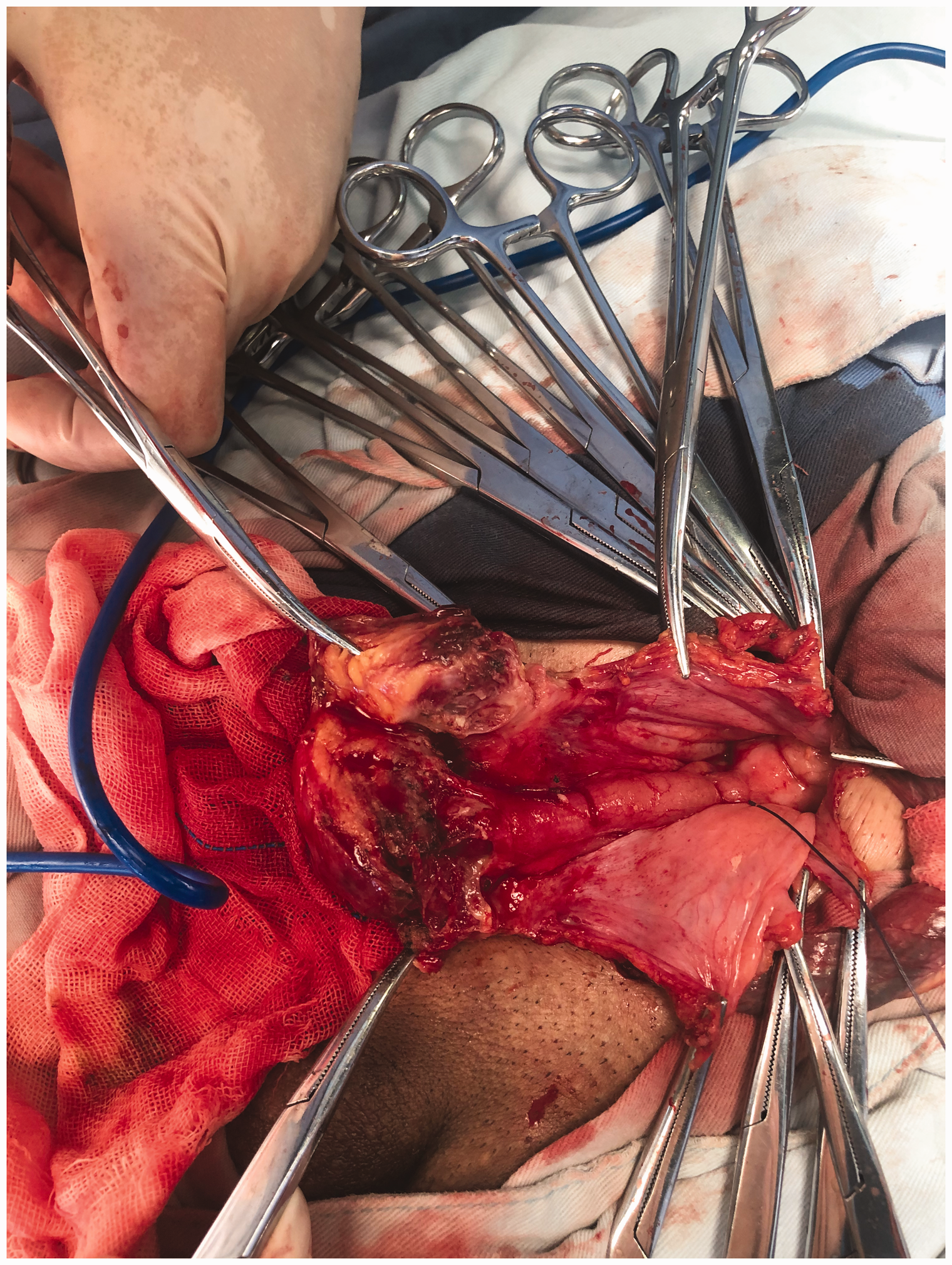
The inguinal ligament was cut off and the hernia sac and appendix were raised.
Postoperatively, the patient received intravenous antibiotics for 5 days and stayed in bed for 7 days. The negative-pressure drainage tube was removed on postoperative day 4. The histopathologic examination confirmed purulent appendicitis. The patient recovered uneventfully and was discharged on postoperative day 8 in good general condition.
The reporting of this study conforms to the CARE guidelines. 4
Discussion
The proportion of De Garengeot hernias among all femoral hernias is only 0.5% to 5.0%, and its low incidence means that we have little experience in its diagnosis and treatment, especially in male patients. 1 We know that the femoral canal has a special anatomy and is prone to incarceration, which can rapidly lead to a strangulated hernia. However, the femoral canal is a relatively closed anatomical structure. Even when the appendix in a De Garengeot hernia perforates, local obvious pain may be the only symptom. Our patient had no fever, abdominal tenderness, rebound pain, or guarding. In addition, because the diameter of the femoral canal generally does not allow the appendix and intestine to be incarcerated at the same time, intestinal obstruction is rare.
Thus, achieving a preoperative diagnosis of a De Garengeot hernia is quite difficult, and in some cases, delayed diagnosis and treatment can lead to adverse outcomes such as ischemic necrosis of the hernia contents, septicemia, abscess formation, secondary ileus, and necrotizing fasciitis. Typical clinical symptoms, such as an irreducible mass in the inguinal region accompanied by local redness and swelling, have a certain suggestive effect on the diagnosis. The white blood cell count and neutrophil percentage may be elevated, but lack of elevation is also common. In our patient, only the percentage of neutrophils was slightly elevated. Computed tomography is reportedly the most sensitive and specific technique among the available imaging tests for preoperative diagnosis of a De Garengeot hernia. 5 Nevertheless, its sensitivity is only 40% and specificity is about 60% to 70%.6,7 In our case, we failed to achieve an accurate preoperative diagnosis because of the lack of knowledge of De Garengeot hernias among both our surgeons and radiologists.
A standard surgical procedure has not been established because of the rarity of this disease, but prompt surgery has become the consensus. 8 The surgical approach should be determined by the surgeon’s individual experience and the specific characteristics of the case. The most common procedure is the open anterior approach; this allows exploration of the hernia sac and rapid treatment of its contents, routine appendectomy through a single incision, and preperitoneal repair of the femoral hernia. 2 If the hernia sac is irreducible, a second incision using McEvedy’s high approach can facilitate reduction of the hernia after division of the lacunar ligament.9,10 McBurney incision and subumbilical midline laparotomy are also common additional incisions. 2 Based on the surgeon’s expertise, laparoscopy can be attempted and converted to open surgery if a more complicated hernia is found. 11
In a meta-analysis of 90 patients, the percentage of complications in 79 patients was 11%, including wound infection, postoperative ileus, postoperative seroma, and reintubation. The follow-up time was generally short, no conclusions can be drawn regarding recurrent hernias. There was no mortality. 3
In our case, through the open preperitoneal approach, we cut off the inguinal ligament and then raised the hernia sac and appendix through the single incision. After resection of the appendix and hernia sac, we repaired the hernia by suturing the conjoint tendon to Cooper’s ligament and then repaired the inguinal ligament with PDS-II suture, which can maintain its intensity for 6 to 12 months and reduce the risk of postoperative infection. In this case, considering the inflammation of the appendix, we refrained from the use of mesh and placed a negative-pressure drainage tube in the inguinal canal. Postoperatively, the patient stayed in bed for 7 days because McVay repair may have the highest tension among anatomical repair techniques and we cut off the inguinal ligament in this case. The open preperitoneal approach may be a good option to consider in patients with a De Garengeot hernia.
Conclusion
A De Garengeot hernia is a rare subtype of femoral hernia that lacks specific clinical symptoms and signs, leading to a difficult preoperative diagnosis. Among the available imaging tests, computed tomography shows the best results. Surgery should be performed as soon as possible to avoid further complications. The open preperitoneal approach may be a good option to consider in patients with a De Garengeot hernia. When severe inflammation is present, anatomical repair is imperative. Cutting off the inguinal ligament is an effective method if the hernia sac is irreducible. An additional incision is also feasible. Therefore, there is no consensus on the optimal surgical approach, and the surgeon should choose the most suitable surgical method for the patient based on the preoperative and intraoperative findings and his or her own experience.
Footnotes
Acknowledgments
We thank our colleagues from Dalian Third People’s Hospital Affiliated to Dalian Medical University, who provided insight and expertise that greatly assisted in the writing of this paper.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics
This research was approved by the Ethics Committee of Dalian Third People’s Hospital Affiliated to Dalian Medical University (Approval number: 2020-LW-001). Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by Dalian Third People’s Hospital Affiliated to Dalian Medical University.