
Abstract
Background
Recent studies have reported associations between, human bocavirus (HBoV), and respiratory tract diseases in children. However, there is limited information on the epidemiology of HBoV in infants. This prospective study investigated the prevalence and clinical characteristics of HBoV infection in infants with acute lower respiratory tract infection (ALRTI) in eastern China.
Methods
Nasopharyngeal aspirates and throat swab samples were collected from infants with ALRTI and age-matched healthy infants between January 2016 and December 2019. HBoV was identified by polymerase chain reaction. Laboratory data and clinical characteristics were analyzed.
Results
Of 2510 infants, 145 tested positive for HBoV. The highest prevalence of HBoV was detected during the winter. Co-infection was frequently observed during this period of high viral transmission. There were no HBoV-positive infants in the control group. Clinical signs and symptoms included cough, wheezing, fever, nasal discharge, vomiting, diarrhea, hypoxemia, and tachypnea. Co-infections included: Streptococcus pneumoniae, Staphylococcus aureus, Mycoplasma pneumoniae, Chlamydophila pneumoniae, respiratory syncytial virus, and adenovirus.
Conclusions
HBoV was frequently detected in infants with ALRTI in China. The prevalence of HBoV was highest in winter. Co-infection was common, especially in infants requiring intensive care unit admission. Comprehensive clinical evaluation may facilitate optimal treatment.
Keywords
Introduction
Acute lower respiratory tract infection (ALRTI) is the leading cause of illness and death in infants worldwide, 1 especially in developing countries. 2 However, most respiratory tract infections remain undiagnosed. 3 Previous studies have detected human bocavirus (HBoV) in human nasopharyngeal aspirates (NPAs) from children with respiratory tract infections. Comprehensive sequencing and phylogenetic analyses revealed that HBoV belongs to the Parvoviridae family. 4 Recent reports have demonstrated a strong correlation between HBoV and upper and lower respiratory tract infection, 5 asthma exacerbation, 6 bronchiolitis, 7 and acute otitis media. 8 The results of these studies have been contradictory as they focused entirely on the viral pathogens and disregarded the characteristics and clinical features of the study population, resulting in high variation in prevalence estimates (0.6%, 9 19%, 10 and 24% 11 ). Infants younger than 2 years of age are thought to be at high risk of HBoV infection because they are no longer protected by maternal antibodies. 12 , 13 Infants younger than 1 year of age have even higher risk of respiratory tract infections, but little is known regarding the incidence of HBoV infection in this age group. To fill this HBoV research gap, we conducted a 3-year prospective study in infants younger than 1 year hospitalized with ALRTIs.
Materials and methods
This was a prospective study. The study population comprised infants of Chinese Han nationality who were hospitalized with ALRTIs at Ningbo Women and Children’s Hospital between January 2016 and December 2020. We also collected samples from a control group of age-matched healthy infants from the health examination clinic service (sample size estimation: p = 0.03, ε = 0.1, α = 0.05, Z1-α/2 = 1.96, N = 1794). The study protocol was approved by the Ethics Committee of Ningbo Women and Children’s Hospital with approval number 2019-ky-041. Signed informed consent was obtained from the parents of each infant. We collected data on the epidemiological, clinical, and laboratory characteristics of HBoV-positive infants during the study period. We collected NPAs and throat swab samples from both HBoV-positive and control infants. The study followed the STROBE-NI guidelines. Specimens were transported to the virology laboratory within 24 hours and stored at −80°C. Additionally, the presence of respiratory syncytial virus, adenovirus, rhinovirus, and influenza virus A was assessed by polymerase chain reaction. Serum samples were obtained to measure levels of antibody against Mycoplasma pneumoniae and Chlamydia pneumoniae by ELISA. The ELISA kit was from Shanghai Sangon Bioengineering (Shanghai, China). We recorded biochemical data and clinical findings for all hospitalized infants.
Samples from both groups were tested for HBoV using a reverse transcription polymerase chain reaction
14
kit and two primer sets specific for the NP1and NS1 genes
4
(Nippon Chemi-Con, Tokyo, Japan). The QIAamp DNA Mini Kit (Qiagen, Hilden, Germany) was used to extract DNA from samples following the manufacturer’s protocol. The first set of primers (F: 5′-
Bacterial specimens were collected on the day of admission. Deep sputum was obtained by negative pressure before antibiotics were administered. After the infant was admitted to hospital, oropharyngeal and nasopharyngeal secretions were cleaned, and then a disposable sterile sputum suction tube was fully inserted into the subglottic airway to extract sputum from the deep trachea. Sputum was cultured on M2H agar with various antimicrobial susceptibility disks (Oxoid, Basingstoke, UK). The isolation and identification of strains was carried out according to conventional methods and in strict accordance with the operating instructions of the VITEK232 automatic microbial analyzer (bioMérieux, Marcy-l'Étoile, France).
Parametric data were described as means ± standard deviations. All analyses were performed using SPSS 22.0 (IBM, Armonk, NY, USA). The chi square test and Student’s t-test were used to assess differences between groups. Values of p < 0.05 were considered statistically significant. The Research Registry Number was: researchregistry6791.
Results
A total of 2510 infants hospitalized with ALRTIs between January 2016 to December 2020 as well as 1255 age-matched healthy infants were enrolled in the study. There were no significant differences in age or sex between the infants with ALRTIs (age 8.9 ± 2.1 months, male:female ratio 1.67:1) and the control group (age 7.4 ± 1.7 months, male:female ratio 1.73:1). Approximately 20 samples were obtained each month. HBoV DNA was detected in 145 (5.78%) of 2510 NPA samples. The median age of HBoV-positive infants was 8.4 months (range: 3 to 11 months); 89 (61.4%) were male and 56 (38.6%) were female. The male:female ratio was 1.6:1. HBoV-positive NPA samples were detected in every season, with the highest prevalence observed during the winter months. No samples from healthy control infants were HBoV-positive (Figure 1).

Number of HBoV-positive infants by month.
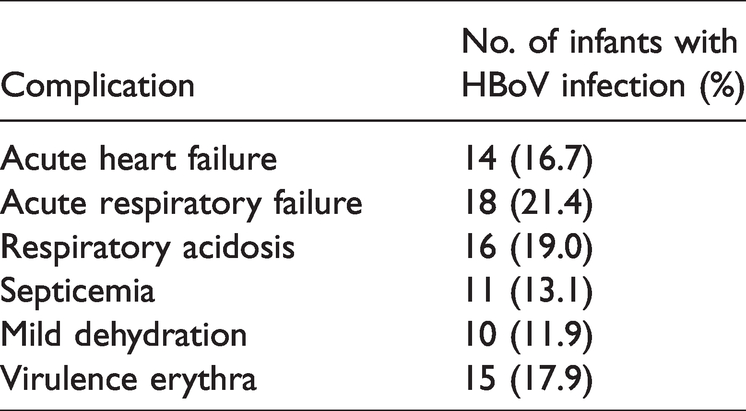
In HBoV-positive infants, cough (130 infants, 89.7%), wheezing (92 infants, 62.1%), and fever (76 infants, 52.4%) were frequent symptoms. Abnormal chest radiography findings were present in all HBoV-positive infants, while 95 infants had pneumonia, 50 had acute bronchitis or bronchiolitis as shown by X-ray examination, 18 had focal pulmonary atelectasis, and 13 had localized pulmonary emphysema. A total of 39 infants had pO2 < 94% (all of whom were admitted to the intensive care unit [ICU]; among then, 11 infant had pO2 < 90%. In 14 infants, HBoV was complicated by acute heart failure and in 12 infants, HBoV was complicated by respiratory failure. Septicemia was diagnosed and Staphylococcus aureus isolated from one infant with ALRTI. Tables 1 and 2 summarize the clinical presentation of the infants.
Clinical presentation of infants with HBoV infection.

*Cough, wheezing, and fever showed no differences between infants with HBoV infection alone or infants with co-infection.
ND, not done.
Complications in infants with HBoV infection.
Co-infection was frequently detected in winter. M. pneumoniae and respiratory syncytial virus were the most common pathogens responsible for co-infection. Three infants with severe ALRTI had two or more co-infections (Table 3). Presence of multiple co-infections was associated with ICU admission (p < 0.05) (Table 4).
Pathogens responsible for co-infections in infants with HBoV infection.

Frequency of co-infection in infants with HBoV infection in the pediatric ward and the ICU.

Abbreviations: ICU, intensive care unit.
Discussion
Here, we studied the epidemiological characteristics of infants with ALRTI in eastern China. The prevalence of HBoV was 5.58%, consistent with recent studies conducted in eastern China and southeast Asia15–20 but lower than prevalence estimates from Singapore 21 and Japan. 12 Differences among these estimates could be attributable to sample size.
Studies of the prevalence of HBoV infection in Asia showed that prevalence maxima were observed in different seasons across different regions, 12 ,16–19, 22 , 23 with no distinctive seasonal pattern. 20 Our data revealed that although HBoV could be detected throughout the year, a higher HBoV prevalence was observed in the winter months (November, December, January). In HBoV-positive infants, co-infection was frequently observed and mainly occurred during periods of high viral transmission. We also observed a few cases of HBoV co-infection in pediatric patients with M. pneumoniae and C. pneumoniae. The etiological characteristics of co-infection require further investigation.
In this study, bronchitis, bronchiolitis, and pneumonia were frequently diagnosed in infants with cough, wheezing, and fever. Other symptoms included nasal discharge, vomiting, diarrhea, and tachypnea. Infants with severe infection had complicated dysphoria, respiratory exacerbation, and hypoxemia, and some developed respiratory acidosis, respiratory failure, and acute heart failure. Pathogens involved in co-infection included S. pneumoniae, S. aureus, M. pneumoniae, C. pneumoniae, respiratory syncytial virus, and adenovirus. Co-infection was observed in all infants with severe infection, suggesting a correlation with clinical severity. Our findings suggested that respiratory tract co-infection was a potential risk factor for HBoV-positive infants. However, HBoV was probably not an independent etiological factor in infants with severe ALRTI, as was previously reported in Switzerland. 24 Although most cases of HBoV infection are mild, some may be severe. In our study, some HBoV-positive infants developed sepsis, heart failure, and respiratory failure. Previous studies have reported other severe complications of co-infection with HBoV and other viruses such as pneumothorax, acute otitis media, encephalitis, and pneumomediastinum. Our results were consistent with those of previous studies carried out worldwide. Chia-Yunn et al. 25 found that HBoV infection peaked during winter and spring. Aykut et al. 26 found that in Turkey, children with coinfection had higher risks of ICU admission compared with those with HBoV mono-infection. In another study carried out in Turkey, co-infections by HBoV and other viruses were frequently detected. 27 A study in Finland showed that HBoV persisted in the respiratory tract for long periods, increasing the chance of co-detection with other viruses. 28 Emanuels et al. also found a high prevalence of HBoV and other pathogens in Nepal. 29 Nada et al. found that in Kuwait, the incidence of HBoV infection was highest among children <1 year old. Co-infection was detected in 56.8% of patients. 30 The prevalence of HBoV is greatly affected by geographical location. In Italy, Cangiano et al. reported a prevalence of 1.8% over 10 consecutive years, 31 while Sobkowiak et al. 32 found a HBOV prevalence of 27% in wheezy children under age 2 years in Poland. In Portugal, Huguenin reported a HBoV prevalence of 37.1%. 33
There were several limitations to our study. The number of HBoV positive infants was relatively small, and differences in the clinical manifestations of infection need to be further studied. The symptoms of infants were described by their parents and might not have been completely objective. The study was conducted in eastern China, and data from hospitals in other geographical areas are needed to extend our results. Further studies are required to determine the role of HBoV infection in different regions and in children of different ages. Moreover, there were no HBoV-positive infants in the control group. Further studies are needed to explore HBoV epidemiological characteristics in healthy individuals.
In conclusion, this study found a high HBoV prevalence during winter among infants in eastern China. Our data suggest that the clinical severity of disease in hospitalized infants with ALRTI might not be independently associated with HBoV infection. However, co-infection might be a risk factor for severe clinical infection.. Further studies need to be conducted to explore the clinical epidemiology of HBoV infection.