
Abstract
Objective
Tracheal intubation using a direct laryngoscope is difficult to teach. The McGrath videolaryngoscope, a Macintosh-like device with a camera, can be used as a direct laryngoscope to educate novices under supervision using the screen. We compared the effect on Macintosh laryngoscopy skills following training with a McGrath videolaryngoscope as a direct versus indirect laryngoscope.
Methods
Thirty-seven participants were randomized into direct and indirect groups according to the training method using a McGrath videolaryngoscope. Participants attempted Macintosh direct laryngoscopy in normal and difficult airway scenarios. The primary endpoint was the intubation time, and the rate of successful intubation, dental trauma, and difficulty were secondary outcomes.
Results
The intubation time after education decreased significantly in both groups and was significantly shorter in the direct group than in the indirect group across time. The difficulty degree in the direct group was lower than that in the indirect group across time; however, the rate of dental trauma was not significantly different.
Conclusion
Both direct and indirect laryngoscopy using a McGrath videolaryngoscope improved the performance of Macintosh direct laryngoscopy in novices, while direct laryngoscopy using a McGrath videolaryngoscope demonstrated better educational effects than indirect laryngoscopy.
Registered at ClinicalTrials.gov (NCT03471975).
Keywords
Introduction
Tracheal intubation using a direct laryngoscope is an essential skill for airway management.1–3 However, this skill is difficult to teach and supervise because the instructor cannot share the trainee’s direct view during intubation.4–6 Thus, it is difficult to recognize problems that trainees encounter during direct laryngoscopy, which limits the instructor’s ability to provide proper feedback and delays the trainee’s learning curve for tracheal intubation. 7
Several videolaryngoscopes have been introduced and are used for learning direct laryngoscopy. There are two teaching methods using the videolaryngoscope system, and the first method incorporates a video system into the direct laryngoscope. In this system, the trainee performs direct laryngoscopy using a direct view, and the instructor provides feedback using the images observed on the video system. This method has been reported to enhance teaching ability.7–10 In the second method, indirect videolaryngoscopy is used by both the instructor and trainee, so that they share the same onscreen view during intubation. Recently, indirect videolaryngoscopic intubation was reported to improve skills in direct laryngoscopy. 11 , 12 However, to our knowledge, no study has evaluated which teaching method is more effective for acquiring the skill of direct laryngoscopy.
The McGrath videolaryngoscope is a Macintosh-type videolaryngoscope that can be used as an indirect videolaryngoscope or a direct laryngoscope. 13 This dual function can be used when educating novices, using the two methods mentioned previously. In this study, we aimed to compare the effect on skill improvement of Macintosh direct laryngoscopy following training with a McGrath videolaryngoscope as a direct laryngoscope versus an indirect laryngoscope.
Methods
This study was a single-center, prospective, cluster-randomized controlled trial with two parallel groups performed at our institution from March 2018 to July 2018. The trial was approved by our institutional review board (20 February 2018) and was registered at ClinicalTrials.gov (NCT03471975).
Eligible participants were medical students and novices at direct laryngoscopy. Thirty-seven medical students in their second clinical year of education at our medical school participated in this educational intervention during a 1-week rotation in the anesthesiology department, after providing written informed consent. All of the participants agreed to have their performance evaluated and their results used anonymously for scientific and educational purposes. Most of the participants had one or two prior experiences performing direct laryngoscopy on a manikin during a lecture at medical school. The rotation groups constituted 11 groups of three to four students. The groups were randomly divided into direct and indirect laryngoscopic groups at a 1:1 ratio by the cluster randomization method, using a computer-generated random number table (Figure 1). The allocation process was conducted by a colleague who was not involved in this research project. The randomization result was concealed within serially-numbered opaque envelopes, which were opened prior to teaching. One group was trained using direct laryngoscopy with a videolaryngoscope (direct group), and the other group was trained using indirect videolaryngoscopy with a videolaryngoscope (indirect group). Cluster randomization was adopted to eliminate contamination between students owing to individual randomization within each rotation. Blinding of participants and instructors was not possible owing to the nature of the interventions.

Study flow diagram.
The study took place on the first day of the rotation. First, an initial evaluation of the students’ intubation skills was performed on a standardized manikin (Laerdal® Airway Management Trainer; Laerdal, Stavanger, Norway) using a Macintosh laryngoscope (Diamond range, blade size 3; Penlon, Abingdon, UK). The instructor evaluated each attempt and provided no feedback. Then, the students received a lecture on airway anatomy, evaluation, and Cormack–Lehane classification (degree of glottis exposure), as well as airway management, followed by tutorial videos showing the direct laryngoscopy technique and introducing the McGrath™ MAC videolaryngoscope (Medtronic, Minneapolis, MN, USA). A teaching demonstration with the McGrath™ MAC videolaryngoscope followed the lecture. All participants performed five intubations using the manikin and the McGrath™ MAC videolaryngoscope with the instructor’s direct feedback. The direct group intubated using the videolaryngoscope as a direct laryngoscope, where only the instructor could observe the video screen and provide feedback. The indirect group used the videolaryngoscope as an indirect laryngoscope, so that the student shared the video view with the instructor and received feedback (Figure 2).

Illustrations showing how to use the McGrath videolaryngoscope as a direct vs indirect laryngoscope. In both groups, the instructor used the monitor to provide feedback. (a) Direct group: participants used the McGrath videolaryngoscope as for a Macintosh direct laryngoscope. (b) Indirect group: participants used the McGrath videolaryngoscope as an indirect videolaryngoscope, using the monitor.
A final evaluation was performed in which the students performed tracheal intubation using the Macintosh direct laryngoscope in the same manikin in the following scenarios: 1) normal airway in the supine position and 2) cervical immobilization with a semi-rigid foam neck collar (Philadelphia cervical collar; A-Mi Global, Busan, South Korea). Each student performed the intubation twice for each scenario, and the instructor evaluated each attempt. For all intubation attempts, a standard beveled Portex® tracheal tube (7.0 mm internal diameter, 9.6 mm outer diameter; Smiths Medical, Hythe, UK) was used with a stylet inserted in the tube. The tube was bent into a “hockey-stick” configuration. The outcome assessors were not involved in the training and were blinded to the allocation.
The primary endpoint was the intubation time, defined as the time from insertion of the blade between the teeth until inflating the tube cuff. Unilateral bronchial intubation was considered successful for the purpose of this study. Failed intubation was defined as not completed within 120 s or esophageal intubation. Additional data constituted the rate of successful tracheal intubation, dental trauma, and the degree of difficulty. Dental trauma was recorded according to the number of audible teeth clicks (0, 1, and 2) in the Laerdal airway trainer. After the students completed the intubation attempts, they were asked to score the degree of difficulty using each device with a 10-point numeric rating scale (NRS; 0 = easy, 10 = difficult).
Sample size estimation was performed using α = 0.05 and β = 0.2 with 10 s as the clinically relevant difference in intubation time with a standard deviation (SD) of 21 s, in accordance with a similarly designed study from our department that has been submitted for publication. We estimated that at least 17 participants were needed in each group.
All statistical analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA). Data are presented as the mean and SD when normally distributed, as the median and interquartile range when non-normally distributed, and as a percentage when appropriate. We used a linear mixed effects model to analyze intubation times and the degree of difficulty. We used a generalized linear mixed model with binomial distribution and generalized estimating equations to analyze the intubation success rates. As fixed effects, we included baseline intubation time, age, sex, group, manikin scenario, time, and time by group interactions. As random effects, we used a random intercept and slope for intubation time after education and a random intercept only for the degree of difficulty. The variance-covariance structures were chosen with the smallest Akaike information criterion. Quasi-likelihood under the independence model criterion was used to assess the goodness-of-fit when selecting the working correlation matrix in the generalized estimation equations model. We also specified and partitioned different variance-covariance structures for each level of intubation difficulty using the manikin. To compare intubation times before training with those after training, we used the paired t-test, Mann–Whitney U test, or McNemar’s test, as appropriate. A p-value <0.05 was considered statistically significant.
Results
Thirty-seven medical students were recruited and consented to participate in this study. Thirty-one of the students had performed intubation once in a manikin, while six had performed intubation twice in a manikin. There were no statistical differences between the groups regarding the effect of the students’ demographics and baseline data on laryngoscopy and intubation (Table 1). All of the participants attempted five tracheal intubations, and no data were excluded from the analysis. There were no harmful events during this trial.
The participants’ baseline characteristics.

Values are presented as number or number (percentage) or mean ± standard deviation.
M, male; F, female.
The incidences of successful intubation in successive intubation attempts are presented in Table 2; there was no significant difference between the groups.
Incidence of successful intubation using a Macintosh direct laryngoscope.
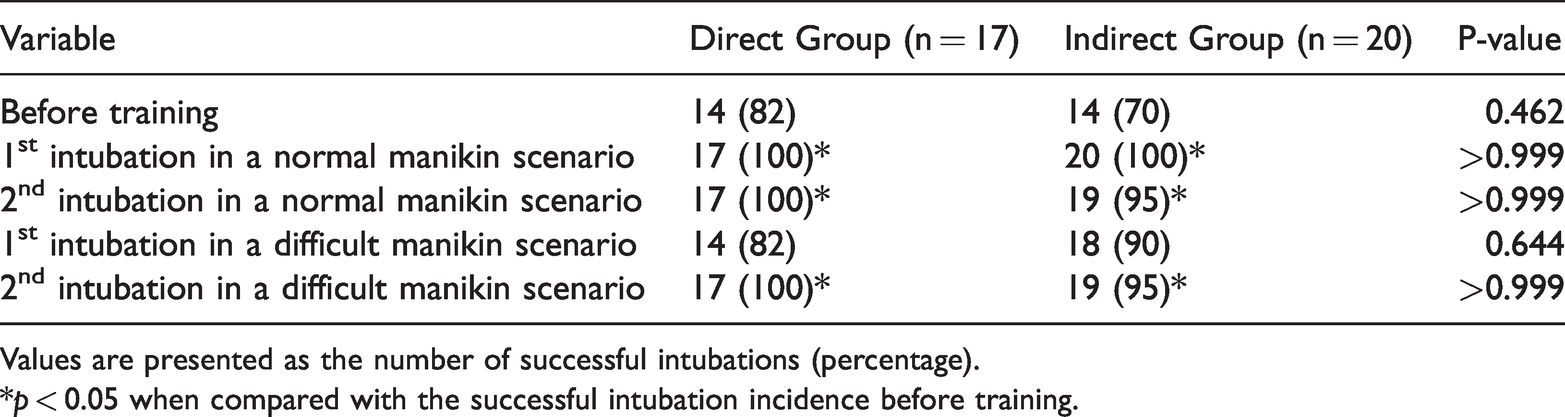
Values are presented as the number of successful intubations (percentage).
*p < 0.05 when compared with the successful intubation incidence before training.
The intubation times are presented in Table 3 and Figure 3. The mean intubation time for the intubation attempt before education was 54.7 s (SD, ± 24.0 s) in the direct group and 56.8 s (SD, ± 35.1 s) in the indirect group. Graphically, the intubation time after education was noticeably shorter compared with that before education. After education, the intubation time in the direct group was shorter than that in the indirect group. We then compared the differences between groups regarding changes at successive time points. We found a statistically significant decrease in intubation time over the four trials (group effect, p = 0.04), while the time-by-group interaction was not statistically significant. Because this interaction indicates that group differences depend on the time point considered, the intubation time difference between groups was not time-related. However, there was a significant effect of time (time effect, p = 0.01) on intubation time after adjusting for the group.
Intubation time.

Values are presented as mean ± standard deviation.
*p < 0.05 compared with intubation time before training. †p < 0.05 compared with intubation time at specific time points between the groups. ‡p < 0.05 compared with ‘intubation time over time’ between the groups.

Intubation times using a Macintosh direct laryngoscope. A0 = before education; A1 = 1st intubation attempt in a normal airway manikin scenario; A2 = 2nd intubation attempt in a normal airway manikin scenario; A3 = 1st intubation attempt in a difficult airway manikin scenario; A4 = 2nd intubation attempt in a difficult airway manikin scenario. †, significantly different compared with before education (A0) in each group; ‡, significantly different between the two groups at specific time point.
The NRS values related to intubation difficulty are presented in Table 4 and Figure 4 and show similar trends to those for intubation time. The NRS value for the intubation attempt before education was 7.3 (SD, ± 2.1) in the direct group and 7.4 (SD, ± 1.8) in the indirect group. Graphically, NRS values after education decreased noticeably compared with those before education. After education, the NRS values in the direct group were lower than those in the indirect group across time. We then compared the differences between groups in the changes in intubation time at successive time points. We found a marginally significant reduction in the NRS values over the four trials, while the time-by-group interaction was not significant, suggesting that the difference in NRS values between the groups was not time-related. However, there was a significant effect of time (time effect, p < 0.001) on NRS values after adjusting for the group.
Intubation difficulty.

Values are presented as mean ± standard deviation.
*p < 0.05 compared with intubation difficulty before training. †p < 0.05 compared with intubation difficulty at specific time points between the groups.

Degree of difficulty using a Macintosh direct laryngoscope. A0 = before education; A1 = 1st intubation attempt in a normal airway manikin scenario; A2 = 2nd intubation attempt in a normal airway manikin scenario; A3 = 1st intubation attempt in a difficult airway manikin scenario; A4 = 2nd intubation attempt in a difficult airway manikin scenario. †, significantly different compared with before education (A0) in each group; ‡, significantly different between the two groups at specific time points.
The number of dental clicks during intubation was lower in the direct group than in the indirect group; however, the difference was not statistically significant (Table 5).
Dental clicks during intubation attempts using a Macintosh direct laryngoscope.

Values are presented as the number of students for each number of dental clicks during intubation (0/1/2).
Discussion
This study demonstrated that the McGrath videolaryngoscope facilitated teaching and supervision of novices during the intubation process and improved their intubation skill using the Macintosh direct laryngoscope in normal and difficult manikin intubation scenarios. Furthermore, education using the McGrath videolaryngoscope as a direct laryngoscope improved the novices’ intubation skills better than when using the videolaryngoscope as an indirect laryngoscope, as demonstrated by a significant reduction in intubation time over the four trials (group effect, p = 0.04).
Direct laryngoscopy using a videolaryngoscope has several advantages over indirect laryngoscopy, for learning. First, the trainee’s direct view provides a similar and familiar experience with the Macintosh direct laryngoscope. In a previous study, direct laryngoscopy using a videolaryngoscope showed poor performance as longer intubation time, higher difficulty score, and higher Cormack–Lehane grade compared with performance using indirect videolaryngoscopy and Macintosh direct laryngoscopy. 13 These results imply that direct laryngoscopy may be unsuitable, clinically; however, from an educational point of view, there may be an advantage for learning because direct laryngoscopy allows the novice to experience a higher Cormack–Lehane grade. Second, the video screen allows the instructor to observe the intubation procedure in real-time, thereby assessing the view of the vocal cords, position of the laryngoscope tip, amount of anteriorly-directed force, confirmation of tracheal tube placement in the larynx, and final position of the tracheal tube between the vocal cords, resulting in efficient instruction to novices.7–9 In previous studies, similar systems, such as the video Macintosh intubating laryngoscope system, direct laryngoscope with attached fiberoptic bronchoscope, BERCI DCI® video laryngoscope (Karl Storz, Tuttlingen, Germany), C-MAC videolaryngoscope (Karl Storz), and GlideScope Direct® (Verathon Inc., Bothell, WA, USA), were proven useful for improving direct laryngoscopic skills. 2 , 3 ,7–10, 14 , 15 The current study demonstrated that a video laryngoscope can be used similarly for direct viewing, and that direct videolaryngoscopy was more efficient than indirect videolaryngoscopy, for learning.
The effect of indirect videolaryngoscopy for learning direct laryngoscopy has been reported. 11 , 12 These studies showed that experience with indirect videolaryngoscopy using the King Vison laryngoscope (KVVL; King Systems, Noblesville, IN, USA) and GlideScope can be transferred to direct laryngoscopic skills, even though the intubation technique differs from that of direct laryngoscopes, namely the indirect view is uncorrelated with the direct view, lack of alignment of the three anatomic axes (oral, laryngeal, and pharyngeal), midline insertion, and manipulation of a styletted tube. 2 Nonetheless, skill improvement in direct laryngoscopy occurs because the video screen more easily demonstrates important anatomical structures (subtle visual clues during laryngoscopy) and the correct technique. 16 In this study, after training with indirect videolaryngoscopy, the novices’ performances in Macintosh direct laryngoscopy improved compared with that prior to training. Although the learning effect was less than that with direct laryngoscopy using a videolaryngoscope, indirect videolaryngoscopy can be still considered for educational purposes, with the advantages that it is easier for a novice to learn,17–19 and supervision can be performed easily and safely on the same video screen. Therefore, we recommend using direct viewing when a Macintosh type-video laryngoscope is used and indirect viewing when videolaryngoscopes that are not similar to the Macintosh laryngoscope are used for learning.
The limitations of this study are that we used a manikin’s airway, which differs from intubation in actual people. The success rate of intubation before training in this study was higher than that in actual people, implying that the manikin’s airway was easier to intubate. Furthermore, there are numerous additional situations that make intubation difficult, clinically. Therefore, caution is necessary when applying the results of studies using manikin models to clinical situations. Further clinical studies are required to evaluate laryngoscopic teaching methods.
In conclusion, both direct and indirect laryngoscopy using a McGrath videolaryngoscope improved Macintosh direct laryngoscopy in normal and difficult manikin intubation scenarios. Learning direct laryngoscopy using a McGrath videolaryngoscope was more effective than using indirect laryngoscopy; however, the effect on learning in actual people must be further evaluated.
Footnotes
Acknowledgement
The authors thank Eun Young Lee (Office of Biostatistics, Ajou Research Institute for Innovation Medicine, Ajou University Medical Center) for her invaluable statistics advice in this study.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.