
Abstract
Objective
To collect computed tomography data of the laryngeal anatomy of Chinese men and to determine the feasibility of using the size 4 Ambu AuraOnce laryngeal mask (Ambu A/S, Copenhagen, Denmark) in Chinese men weighing >70 kg.
Methods
This prospective study involved men who underwent surgery from May 2018 to January 2019 at Jinshan Hospital. Pharyngeal and laryngeal parameters were measured by computed tomography. The laryngeal mask insertion success rate, requirement for tracheal tube insertion, laryngeal mask insertion time, fiberoptic bronchoscopy grading, air leakage pressure, and pharyngeal complications were analyzed.
Results
In a comparison of the size 4 and 5 Ambu AuraOnce devices, the first insertion success rate was 100% and 87% and the three-times insertion success rate was 100% and 93%, respectively, with no significant differences. However, the insertion time was significantly different at 19.6 ± 5.9 versus 31.1 ± 11.2 s, respectively, and the proportions of fiberoptic grading levels were also significantly different. There were no significant differences in the air leakage pressure or pharyngeal complications.
Conclusion
The size 4 Ambu AuraOnce is more adequate than the size 5 for Chinese men weighing >70 kg, with a shorter insertion time and higher fiberoptic bronchoscopic grading.
Introduction
A laryngeal mask airway (LMA) is a supraglottic device (either single-use or reusable) that is used to temporarily maintain an open airway for the administration of anesthesia or during life-saving procedures.1–4 An LMA is designed to be inserted blindly into the hypopharynx through the mouth (as the hypopharyngeal space where the device will be seated cannot be directly observed 5 ) and to create a seal immediately above the glottis opening.1–4 Diverse methods of LMA size selection are available, including methods based on the patient’s actual weight, standard weight, sex, height, distance between the nose and chin, tongue width, 6 distance between the mandibular second molars, 7 or distance between the cricoid cartilage and chin. 8 Sorbello and Petrini 5 found that an important determinant of choosing the correct size of LMA is the patient’s height before (or together with) their weight. Especially in difficult cases involving patients with edentulism or restricted mouth opening, these concepts might also explain the different performances of silicone (more adaptable) and polyvinyl chloride (stiffer) cuffs of inflatable (more adjustable) rather than non-inflatable or self-inflatable (non-adjustable or partially adjustable) supraglottic airway devices. 5 In accordance with manufacturers’ recommendations, the most commonly used method for selecting the appropriate LMA size is by the patient’s actual weight: size 3, 4, and 5 LMAs are used for adults weighing 30 to 50 kg, 50 to 70 kg, and >70 kg, respectively.
Nevertheless, when the LMA size is selected by the patient’s actual weight, satisfactory ventilation under the controlled ventilation mode cannot be achieved in men who weigh >70 kg using a size 5 LMA, and air leakage may even occur.9–12 High body weight is a risk factor for failed LMA insertion in Chinese patients. 13 In addition, LMAs were designed and are manufactured by Western companies based on Caucasian cadaveric specimens; in contrast, data are lacking regarding selection of the proper LMA size according to the anatomical structure of the larynx in the Chinese adult population. Therefore, whether LMA selection according to the patient’s actual weight is suitable for Chinese men weighing >70 kg remains unknown,6,9–11 and more evidence is needed.
We hypothesized that the laryngeal anatomy of Chinese men might affect LMA size selection and that a smaller LMA (size 4) might be more suitable than a size 5 LMA for Chinese men weighing >70 kg. Therefore, this study was performed to collect computed tomography (CT) data of the laryngeal anatomy of Chinese men weighing >70 kg based on three-dimensional reconstruction images and to determine the feasibility of using a size 4 LMA in these patients.
Methods
Study design and patients
This prospective pilot study was approved by the Ethics Committee of Jinshan Hospital, Fudan University (Scientific Research on Ethics of Jinshan Hospital, 2018-06-01). All patients provided written informed consent. The study was performed in accordance with the Declaration of Helsinki.
Consecutive patients were selected from May 2018 to January 2019. The inclusion criteria were an age of 20 to 65 years, American Society of Anesthesiologists (ASA) physical status of I or II, Mallampati class of I or II, male sex, and body weight of either 50 to 70 kg or >70 kg. All patients were scheduled to undergo routine non-laparoscopic surgery under general anesthesia with an LMA (mainly orthopedic, general, and urological surgery with an estimated operation time of <2 hours). The exclusion criteria were unwillingness to cooperate, known or predicted difficult airway, mouth opening of <2.5 cm, and a risk of regurgitation or aspiration. Each patient underwent a plain CT scan of the throat before surgery. Next, according to a random number table, patients weighing >70 kg (Group B, n = 30) were divided equally into Group B1 (size 4 LMA group, n = 15) and Group B2 (size 5 LMA group, n = 15). The LMA used in this study was the Ambu AuraOnce laryngeal mask (Ambu A/S, Copenhagen, Denmark).
CT scan
All patients underwent a plain CT scan of the throat before surgery. A SOMATOM Definition AS CT system (Siemens, Erlangen, Germany) was used to scan each patient from the skull base to the trachea. The scanning side was parallel to the true vocal cords; the layer thickness was 1.5 mm, and the intervals were 0.75 mm. After three-dimensional reconstruction, the films were read and measured. All plain CT scans were performed by the same competent technician with >5 years of experience. All CT readings were performed by the same associate chief radiologist with >15 years of experience.
Use of Ambu AuraOnce laryngeal mask
The patients weighing >70 kg (Group B, n = 30) entered the operation room and underwent venous infusion of lactated Ringer’s solution. Noninvasive blood pressure and pulse oxygen saturation monitoring were routinely performed. The patients were induced with sufentanil (0.2 µg/kg), propofol (2 mg/kg), and cisatracurium (0.1 mg/kg) by an attending anesthesiologist. The Ambu AuraOnce was inserted, and the cuff was inflated to 30 cmH2O. The insertion time (from picking up the Ambu AuraOnce to connection of the Ambu AuraOnce to the anesthesia machine for a manual air leakage test) was recorded.
Placement of the Ambu AuraOnce was tested according to the following criteria established by Keller et al. 14 : the Ambu AuraOnce was inserted smoothly, the chest contour fluctuated well, no air leakage was heard, and the breath sounds of both lungs were symmetrical and clear during auscultation on the manual ventilation mode. On the mechanical ventilation mode, the waveform of carbon dioxide exhalation and the gas pressure were normal. A bronchoscope was then inserted into the Ambu AuraOnce tube to grade the throat anatomy as follows: level 1, the vocal cords are not visible; level 2, the front of the vocal cords and epiglottis can be seen; level 3, the distal vocal cords and epiglottis can be seen; and level 4, only the vocal cords can be seen. 15 The ideal anatomical positions were levels 3 and 4, while levels 1 and 2 were considered non-ideal anatomical locations. Pharyngeal pressure leakage of the Ambu AuraOnce was tested at 5 minutes after insertion. 15 In the manual mode, the adjustable pressure-limiting valve was set to 70 cmH2O, the oxygen flowmeter was adjusted to 3 L/minute, and the rise of the pressure gauge was observed until a constant sound of air leakage could be heard. If the pressure reached 30 cmH2O without audible leakage, the test was terminated and the air leakage pressure was considered to be 30 cmH2O. The Ambu AuraOnce was removed and re-inserted if the chest contour fluctuated abnormally, obvious air leakage could be heard in the manual ventilation mode, or an abnormal carbon dioxide exhalation waveform or gas pressure was observed. If the re-insertion failed three times, the Ambu AuraOnce was deemed inappropriate and a tracheal tube was inserted.
After it had been placed in an appropriate position, the Ambu AuraOnce was fixed with tape and connected to the anesthesia machine in the mode of synchronous intermittent mandatory ventilation. After surgery, the Ambu AuraOnce was removed when the patient was fully awake and could respond correctly to instructions. The Ambu AuraOnce was checked for the presence of blood as the basis for mucous membrane injury. All the above procedures were performed by the same attending physician with >5 years of experience in use of the Ambu AuraOnce.
Follow-up and data collection
The patients were followed up for 24 hours after the operation by a person who was unaware of the specific size selection of the LMA. Any discomfort, such as sore throat or hoarseness, was recorded. Age, height, weight, body mass index (BMI), ASA physical status, Mallampati classification, and interincisor distance were collected by a 5-year senior resident before randomization. The following parameters were measured: the length of the epiglottic tongue surface (the straight-line distance from the end of the epiglottic tongue surface to the root on the median sagittal plane of the CT image) (Figure 2), the root width of the epiglottic tongue surface (the straight-line distance from the root of the epiglottic tongue surface on the cross section of the CT image) (Figure 3), the distance from the root of the epiglottic tongue surface to the entrance of the esophagus (the straight-line distance from the root of the epiglottic tongue surface to the entrance of the esophagus on the median sagittal plane of the CT image) (Figure 2), and the distance between the lateral margin of the piriform fossa on both sides (in order from top to bottom of the CT image when the bilateral superior horns of the thyroid cartilage first appear on the cross section of the CT image) (Figure 4). The first insertion success rate, three-times insertion success rate, insertion time, throat anatomy grade under bronchoscopy, oropharyngeal leak pressure, and mucous membrane injury were recorded.
Statistical analysis
IBM SPSS Statistics for Windows, Version 19.0 (IBM Corp., Armonk, NY, USA) was used for the statistical analysis. Continuous data are presented as mean ± standard deviation and were analyzed using Student’s t-test. Categorical data are presented as number and frequency and were analyzed using the chi-square test. Two-sided P-values of <0.05 were considered statistically significant.
Results
Patients’ characteristics
Sixty-two patients met the inclusion criteria and were enrolled; among them, however, two patients weighing 50 to 70 kg were unwilling to cooperate. Therefore, 30 patients weighing 50 to 70 kg were assigned to Group A and 30 patients weighing >70 kg were randomized to Group B1 (size 4 LMA group, n = 15) and Group B2 (size 5 LMA group, n = 15) (Figure 1). There were no statistically significant differences in age, height, weight, BMI, ASA physical status, Mallampati classification, or interincisor distance between Groups A and B (Table 1) or between Groups B1 and B2 (Table 2).

Patient flow chart. Group A: patients weighing 50 to 70 kg. Group B1: patients weighing >70 kg with size 4 LMA. Group B2: patients weighing >70 kg with size 5 LMA.
Characteristics of all patients.
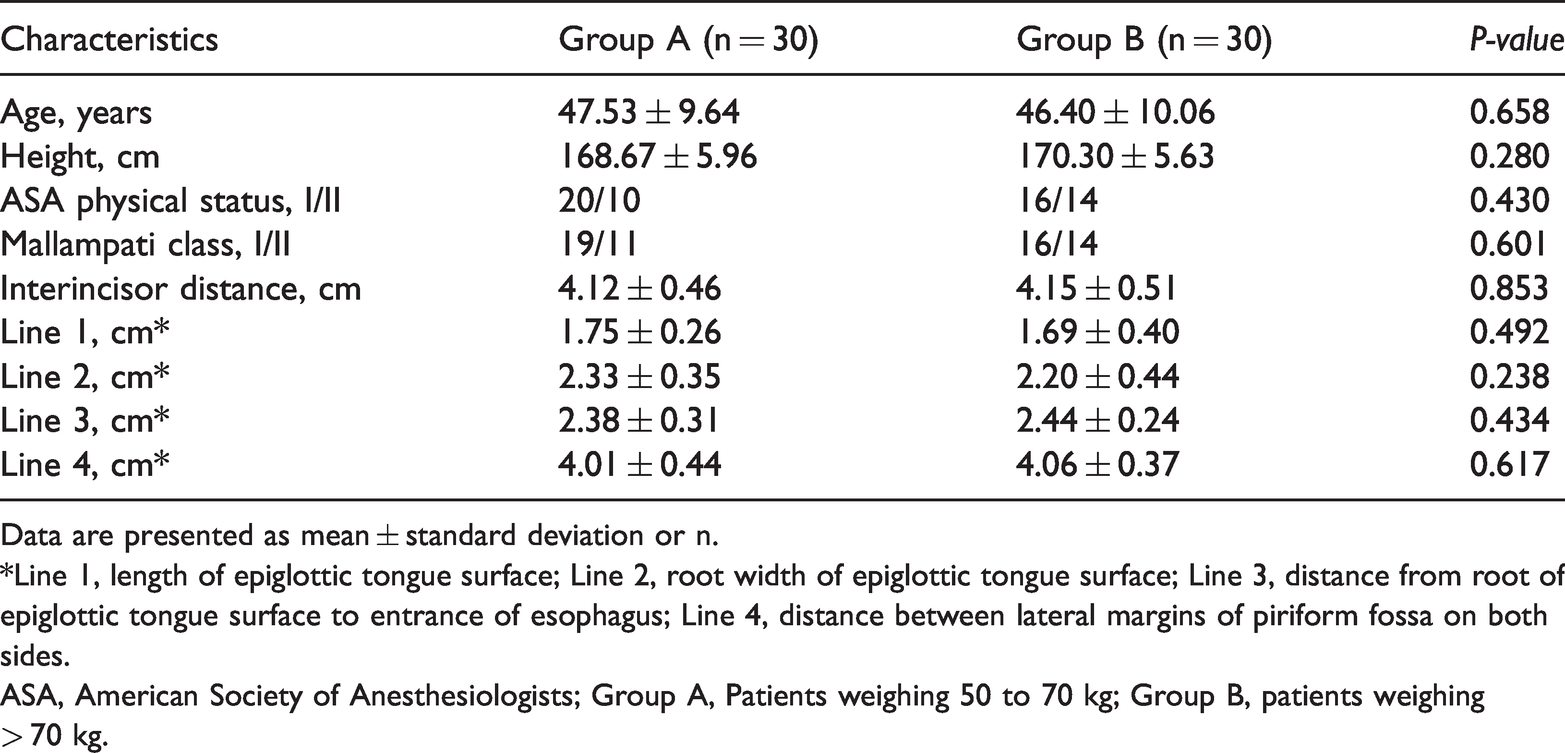
Data are presented as mean ± standard deviation or n.
*Line 1, length of epiglottic tongue surface; Line 2, root width of epiglottic tongue surface; Line 3, distance from root of epiglottic tongue surface to entrance of esophagus; Line 4, distance between lateral margins of piriform fossa on both sides.
ASA, American Society of Anesthesiologists; Group A, Patients weighing 50 to 70 kg; Group B, patients weighing> 70 kg.
Characteristics of Groups B1 and B2.

Data are presented as mean ± standard deviation or n.
*Line 1, length of epiglottic tongue surface; Line 2, root width of epiglottic tongue surface; Line 3, distance from root of epiglottic tongue surface to entrance of esophagus; Line 4, distance between lateral margins of piriform fossa on both sides.
BMI, body mass index; ASA, American Society of Anesthesiologists; Group B1, size 4 Ambu AuraOnce; Group B2, size 5 Ambu AuraOnce.
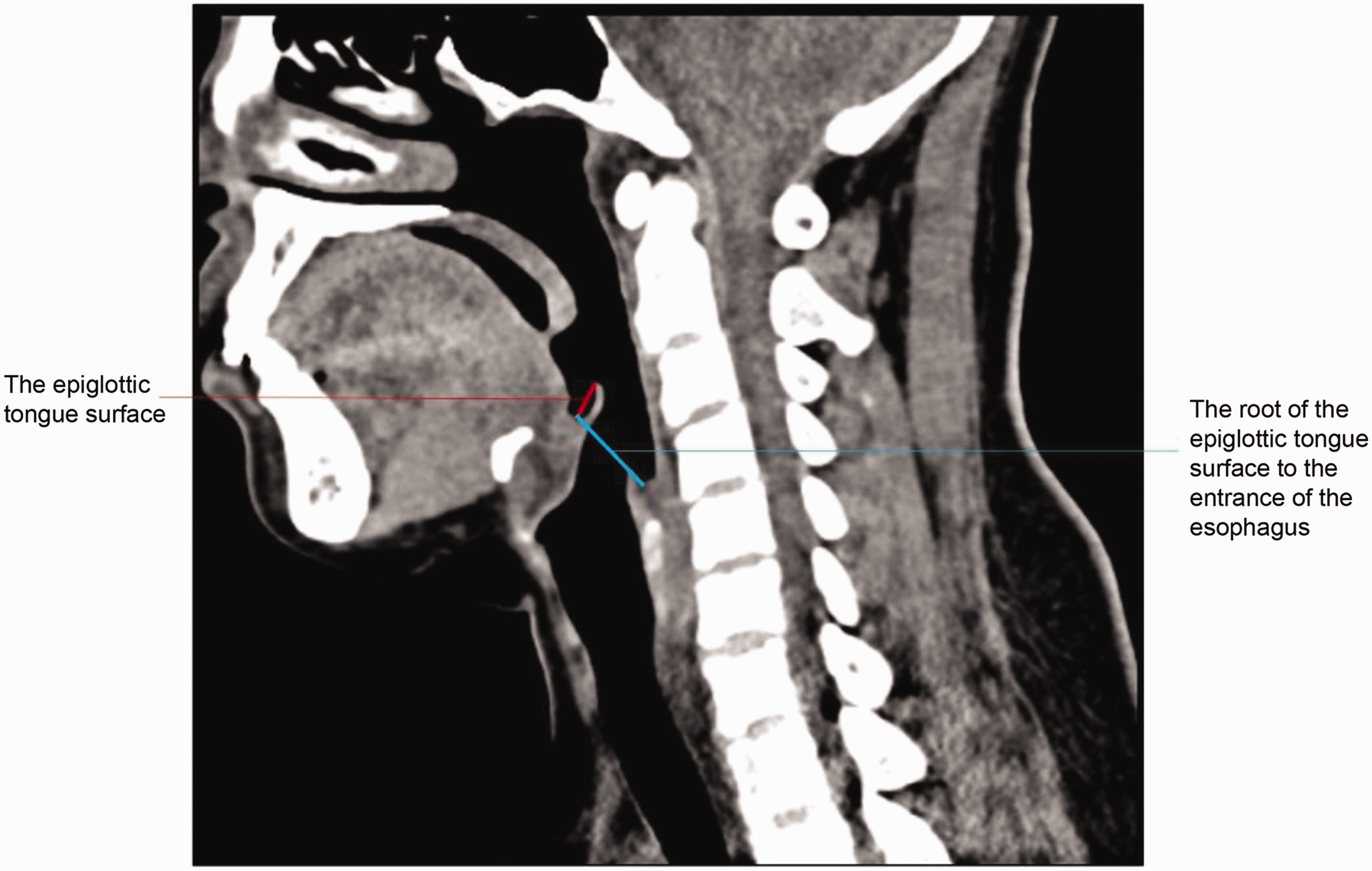
Length of the epiglottic tongue surface and the distance from the root of the epiglottic tongue surface to the entrance of the esophagus.

Root width of the epiglottic tongue surface.

Distance between the lateral margins of the piriform fossa on both sides.
Pharyngeal and laryngeal parameters
When comparing the length of the epiglottic tongue surface, the root width of the epiglottic tongue surface, the distance from the root of the epiglottic tongue surface to the entrance of the esophagus, and the distance between the lateral margin of the piriform fossa on both sides based on the three-dimensional CT reconstruction image, there were no statistically significant differences between Groups A and B (Table 1) or between Groups B1 and B2 (Table 2). Based on the similarity of the pharyngeal and laryngeal parameters between Groups A and B, we speculated that the size 4 Ambu AuraOnce, which is suitable for Chinese men weighing 50 to 70 kg, might be adequate for Chinese men weighing >70 kg.
Insertion success
The first insertion success rate of the Ambu AuraOnce in Groups B1 and B2 was 100% and 87%, respectively, and the three-times insertion success rate was 100% and 93%, respectively. Only one patient required a tracheal tube in Group B2 (Group B1 vs. B2: 0% vs. 7%, respectively). The insertion time was significantly shorter in Group B1 than B2 (19.6 ± 5.9 vs. 31.1 ± 11.2 s, respectively; P = 0.002). The proportion of fiberoptic grading levels was also significantly different between Groups B1 and B2 (P = 0.017). There was no significant difference in the air leakage pressure between Groups B1 and B2 (29.6 ± 1.6 vs. 26.9 ± 5.1 cmH2O, respectively) (Table 3).
LMA insertion parameters in Groups B1 and B2.
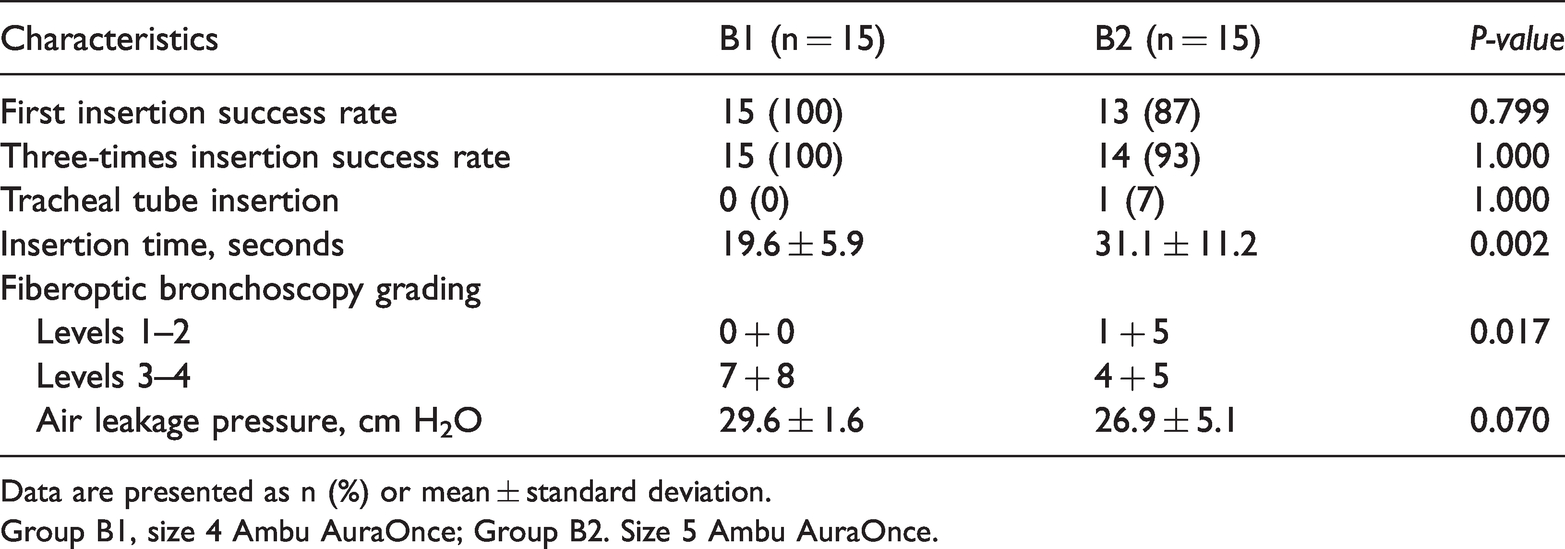
Data are presented as n (%) or mean ± standard deviation.
Group B1, size 4 Ambu AuraOnce; Group B2. Size 5 Ambu AuraOnce.
Pharyngeal complications after surgery
No patients in Group B1 or B2 developed sore throat or hoarseness. There was no statistically significant difference in the incidence of laryngopharyngeal mucosal injury between Group B1 (n = 0) and Group B2 (n = 1).
Discussion
Various types of LMAs are available for adult patients in clinical practice.6–8 Additionally, various LMA selection methods may be used to choose the most suitable LMA for the patient’s laryngeal anatomy.1–4 An unsuitable LMA may lead to leaks, unsatisfactory ventilation, or injury.1–4 The LMA size in adults is usually determined by weight, but this method could be inappropriate for Chinese men who weigh >70 kg.1–4 In the present study, we used the Ambu AuraOnce laryngeal mask. It is a first-generation supraglottic airway device constructed from a single-piece polyvinyl chloride mold and incorporates a 70° preformed curvature that better approximates the airway anatomy. It features an inbuilt curve in the airway tube designed to allow the head to remain in a more natural position and to reduce stress on the upper jaw, and it lacks epiglottic bars. This device provides the safety and convenience of a sterile, single-use product. Many studies of adult populations have demonstrated that it has the capability of easy insertion, high oropharyngeal leak pressure, and low complication rates with few postoperative complaints. The patient’s actual weight is also used for selecting the most appropriate Ambu AuraOnce laryngeal mask size according to the manufacturer’s recommendation: size 3, 4, and 5 LMAs are used for adults weighing 30 to 50 kg, 50 to 70 kg, and >70 kg, respectively.
We hypothesized that the laryngeal anatomy of Chinese men might affect the size selection of the Ambu AuraOnce laryngeal mask. Most laryngeal masks were designed and are manufactured by Western companies, mainly based on Caucasians; thus, an LMA might not fit perfectly in Chinese patients when following the size selection rules. Indeed, differences in morphology can be observed.16–18 The present study was performed to measure the relevant anatomical diameter lines according to the ideal anatomical position of the Ambu AuraOnce. First, the straight-line distance from the end of the epiglottic tongue surface to the root on the median sagittal plane of the CT image was measured as the length of the epiglottic tongue surface. This diameter line should be less than the major axis of the mask; if the line is too long, air leakage or ventilation difficulties may occur. Next, the straight-line distance from the root of the epiglottic tongue surface on the cross section of the CT image was measured. To ensure that the Ambu AuraOnce is ideally positioned, the root of the epiglottic tongue surface must be covered by the Ambu AuraOnce; otherwise, air leakage will occur. The straight-line distance from the root of the epiglottic tongue surface to the entrance of the esophagus on the median sagittal plane of the CT image was then measured. Under ideal conditions, this diameter line should be less than the major axis, or air leakage will occur.
The fourth line measured was the distance between the lateral margins of the piriform fossa on both sides. Under ideal conditions, this diameter line should be less than the horizontal axis of the mask. In the present study, there were no differences in those four diameters between Chinese men weighing 50 to 70 kg and those weighing >70 kg, suggesting that an identically sized Ambu AuraOnce could fit the two groups of patients. Because of the limited space of the anatomical structure of the larynx, even if the size 5 Ambu AuraOnce is larger and can seal the glottis better than smaller masks, 19 there is not enough space for the size 5 Ambu AuraOnce to be adjusted in an ideal position in relation to the glottis. The seal could be easier to achieve with the epiglottis reflexed and blocking the glottis. Moreover, the larger size 5 Ambu AuraOnce may lead to more pharyngeal complications when inflated with air. 20 Especially during a long surgical operation, the size 4 Ambu AuraOnce might be safer than the size 5.
In this study, we compared insertion of the Ambu AuraOnce in 30 patients who were randomized to receive either a size 4 or 5 Ambu AuraOnce. There were no significant differences in the patient characteristics between the two groups. Nevertheless, there were statistically significant differences in Ambu AuraOnce insertion time. The size 4 Ambu AuraOnce was inserted more rapidly than the size 5. In addition, the fiberoptic bronchoscopy grading level was higher with the size 4 than size 5 Ambu AuraOnce, indicating that the positioning of the mask was more adequate with the size 4 Ambu AuraOnce. Because the size 4 Ambu AuraOnce is smaller than the size 5, it is easier to insert in the correct position in Chinese men weighing >70 kg.
In addition, only one patient randomized to the size 5 Ambu AuraOnce group required tracheal intubation after three failed attempts to insert the Ambu AuraOnce. We also found that the Ambu AuraOnce was stained with blood and oral secretion in this patient. This might have been due to the size 5 Ambu AuraOnce being too large.
This study has several limitations. This was a pilot study, the sample size was small, and an initial power analysis was not performed. Using the patient’s body weight might not be accurate if the body height is not considered, and future studies should consider the BMI. The results of the present study can only be explained by the fact that the CT parameters were similar between the Chinese men weighing 50 to 70 kg and those weighing >70 kg. The results only show that the size 4 Ambu AuraOnce is suitable for patients who weigh >70 kg, not whether this size is the best option. Additional studies are still necessary.
In conclusion, this study provides CT data of the laryngeal anatomy of Chinese men weighing 50 to 70 kg and >70 kg. There were no differences in the CT parameters of the larynx between the two groups. In addition, compared with the size 5 Ambu AuraOnce, the smaller size 4 might be more adequate for Chinese men weighing >70 kg, with a shorter insertion time and higher fiberoptic bronchoscopic grading. Therefore, use of the size 4 Ambu AuraOnce is feasible in Chinese men weighing >70 kg.
Footnotes
Acknowledgements
The authors acknowledge the help of their colleagues and teachers in the Department of Anesthesiology and Radiology, Jinshan Hospital, Fudan University.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the General Program of Jinshan District of Shanghai Municipal Commission of Health and Family Planning (JSKJ-KTMS-2017-07). The funding body had no role in the study design; in the collection, analysis, or interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
Author contributions
C.C. and C.J. conceived of the study, collected the data, and conducted the data analyses. All authors contributed to the writing of the manuscript.