
Abstract
After reviewing the diagnosis and treatment process of a patient with active cancer who experienced wake-up stroke, we have summarized the clinical manifestations, laboratory examination results, imaging features, pathological results, and treatment in this report. Patients with active cancer who experience wake-up stroke often have mild neurological deficits at the time of onset. For the patient in this study, laboratory test results were mainly characterized by abnormal coagulation function and elevated tumor markers. The brain magnetic resonance imaging (MRI) images were characterized by involvement of both the arterial and venous systems. Thrombolytic therapy during the window period can improve the symptoms of neurological deficits. Overall, anticoagulation therapy was safe and effective in our patient.
Keywords
Introduction
The morbidity and mortality rates associated with cancer are among the highest in the world when compared with other diseases. Currently, clinicians have gradually established the close relationship between cancer and acute ischemic stroke (AIS). 1 Alteplase is always administered to patients with AIS within the time window. 2 Wake-up stroke refers to when a patient wakes up and develops new stroke symptoms not seen before falling asleep. It is difficult to determine the exact time of stroke onset in patients who experience wake-up stroke. Unfortunately, there have been no studies conducted on using intravenous thrombolysis treatment for patients with active cancer who experience wake-up stroke. Here, we report the therapy course of a patient with active cancer who experienced wake-up stroke, as well as a relevant literature review. The patient gave written consent to both the treatment described below and the publication of this article.
Case report
A 61-year-old male patient was admitted to Hainan Hospital of Chinese PLA General Hospital following motor aphasia and visual field defects that occurred for 2.5 hours after waking up. The patient had been healthy in the past. A brain computed tomography (CT) scan was urgently examined, but no abnormal signal was found. After a systemic nervous examination, the patient’s National Institutes of Health stroke scale (NIHSS) score was 5 points. The diagnosis was AIS and a sufficient amount of alteplase (0.9 mg/kg) was given intravenously for treatment. The patient's speech ability returned to normal after 24 hours and his NIHSS score decreased to 1 point. A brain magnetic resonance imaging (MRI) scan revealed acute infarct lesions in both the left frontal and right occipital lobes

Brain diffusion-weighted imaging of a magnetic resonance imaging (MRI) scan revealed acute infarct lesions in the left frontal lobe and right occipital lobe.

Brain fluid attenuated inversion recovery imaging and T2 weighted imaging of a magnetic resonance imaging (MRI) scan revealed acute infarct lesions in the left frontal lobe and right occipital lobe.
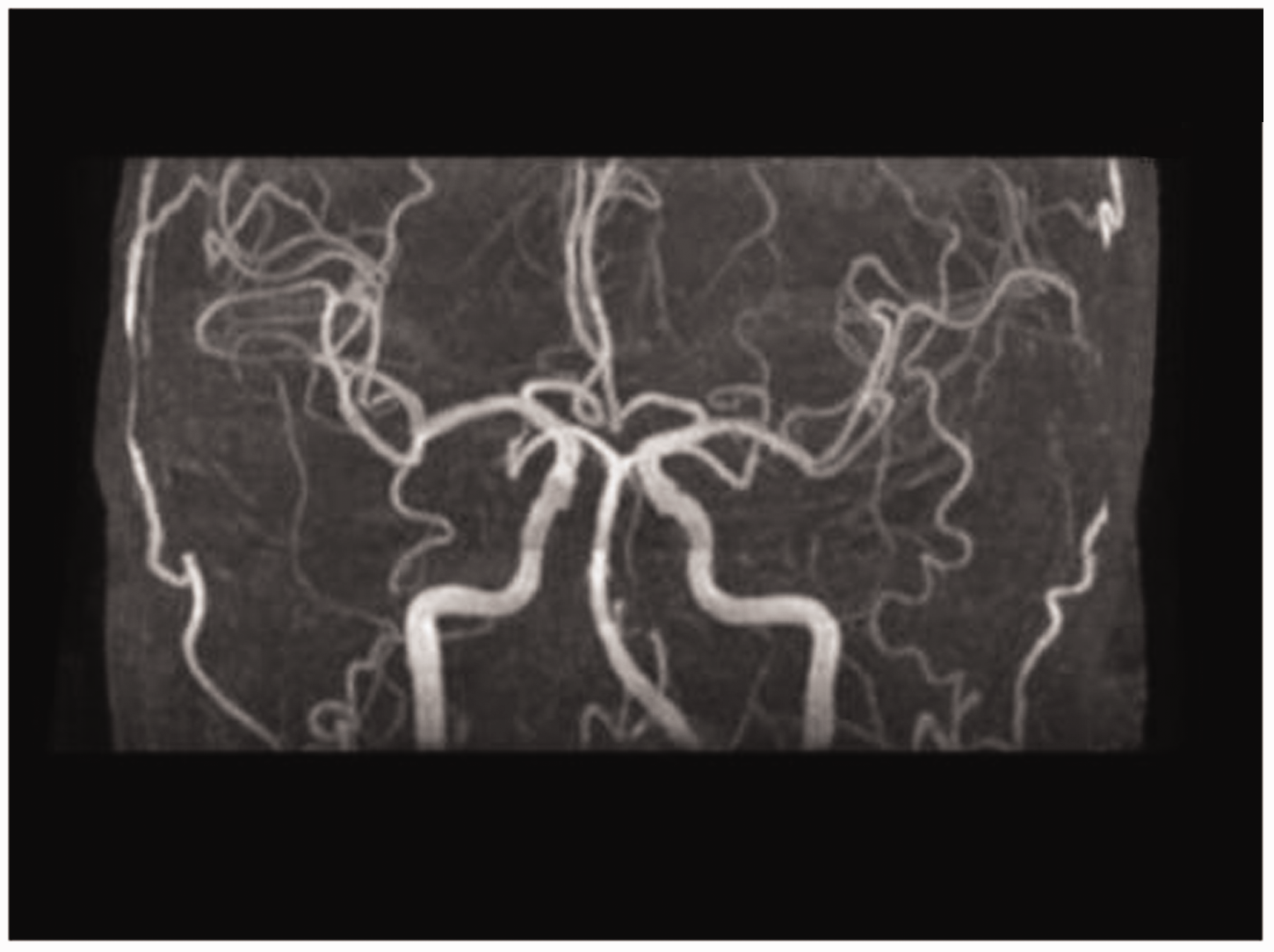
No stenosis of the intracranial artery was found in the brain magnetic resonance angiography (MRA) images.

Positron emission tomography-computed tomography (PET-CT) scans indicated abnormal metabolism in the duodenum.

Positron emission tomography-computed tomography (PET-CT) scans indicated abnormal metabolism in the liver and lymph nodes adjacent to the duodenum.

Electronic endoscopy indicated lesions in the descending duodenal mass.

Pathological results suggested chronic duodenum inflammation of the small intestinal mucosa and diffuse distribution of adenocarcinoma cells, including visible tumor giant cells under the epithelium with obvious heterogeneity.
Discussion
Cancer is closely related to ischemic stroke. An autopsy study of patients with cancer found that 14.6% had ischemic stroke and about 50% of them had clinical neurological deficit symptoms. 3 Some scholars considered that, compared with patients without cancer, thrombolytic therapy in patients with cancer may be more likely to lead to hemorrhagic transformation and adverse outcomes. 4 Wake-up stroke is one of the most common forms of AIS. Epidemiological studies found that wake-up strokes account for 8% to 28% of total strokes in patients with AIS.5–7 However, there was no systematic evaluation of thrombolysis in patients with active cancer who experience wake-up stroke, and even relevant case reports were very rare.
In the case presented here, we could not find any common risk factor of AIS or wake-up stroke. Therefore, we considered the patient to have cancer-associated AIS, as active cancer may also be a risk factor of wake-up stroke. The mechanism controlling cancer-associated AIS is complicated, mainly involving platelets, inflammatory cytokines, tissue factors, and vascular endothelial factors. 8 There may be different biological markers in different cancer types. Risk factors for the onset of AIS in patients with intestinal cancer are D-dimer, CEA, and neutrophils. 9 Studies have considered that as the levels of D-dimer, CEA, and neutrophils increase, the risk of AIS also increases. However, our patient with wake-up stroke was not similar to patients with AIS who have common intestinal cancer. The patient’s laboratory results suggested D-dimer, thrombin time, CA125, CA19-9, and CYFRA21-1 were significantly abnormal, which were similar to the risk factors of lung cancer-associated AIS.10,11 In terms of imaging findings, the AIS lesions involved bilateral cerebral hemispheres and anterior and posterior circulation, which meet the characteristics of cancer-associated AIS. 12
A randomized controlled study found that the initial symptoms of neurological deficits in patients with wake-up stroke were usually mild. However, the final prognosis was not significantly different from the patients without wake-up stroke. 13 The study suggested that the condition of patients with wake-up stroke may worsen after it occurs. The safety and effectiveness of thrombolysis treatment for patients with wake-up stroke with active cancer are not very clear. During the therapy course of the patient in this case, we did not observe any thrombolysis-associated adverse events. The patient’s neurological symptoms improved following treatment. Thus, we believe thrombolytic therapy may be safe for cancer patients who meet thrombolytic standards.
Platelets play an important role in the growth and metastasis of cancer. 14 Some scholars have hypothesized that antiplatelet therapy can control tumor progression. However, antiplatelet drugs, including aspirin and clopidogrel, did not improve the hypercoagulable state of the body caused by cancer. 15 Anticoagulation therapy can improve this hypercoagulable state to some extent. Traditional anticoagulant drugs are mostly administered by subcutaneous injection. However, for long-term use of anticoagulant drugs, daily subcutaneous injections are often difficult to achieve. New oral anticoagulants are often selected as secondary prevention drugs for patients who have suffered ischemic stroke. Our patient received thrombolytic and anticoagulation therapies while hospitalized. After discharge from the hospital, we recommend the application of new oral anticoagulant drugs as a secondary prevention strategy. No hemorrhagic transformation occurred during the treatment or follow-up periods. Our previous research suggested that the median survival time of patients with lung cancer-associated AIS was only 5 months. 10 However, we followed up with the patient for 10 months and AIS did not occur again.
Through diagnosing and treating this patient, we found that active cancer may also be a risk factor in patients with wake-up stroke. In the time window, it may be safe to give sufficient alteplase in patients with active cancer who experience wake-up stroke. In addition to the arterial system-related examination, patients with a hypercoagulable state still need to improve the venous system examination. Anticoagulant therapy may be safe and effective in patients with active cancer and wake-up stroke.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hainan Provincial Natural Science Foundation of China, Foundation NO: 818QN320.