
Abstract
Objective
For patients with atherosclerotic renal artery stenosis (ARAS), the role of percutaneous transluminal renal angioplasty (PTRA) remains inconclusive. This study aimed to comparatively evaluate the benefits of best medical therapy (BMT) plus PTRA and BMT alone in treating ARAS.
Methods
We performed a systematic review and meta-analysis, and searched for all randomized, controlled trials that reported patients with ARAS. The effectiveness and safety in the BMT plus PTRA and BMT alone groups were estimated, taking into account hypertension, stroke, renal events, cardiac events, and mortality.
Results
Nine randomized, controlled trials involving 2309 patients were included. In the BMT plus PTRA group, the incidence of refractory hypertension was significantly lower compared with that in the BMT alone group (odds ratio 0.09; 95% confidence interval 0.01, 0.70). However, there were no significant differences in the rates of stroke, renal events, cardiac events, cardiac mortality, and all-cause mortality between the two groups.
Conclusions
PTRA plus BMT improves blood pressure in patients with ARAS, but there is insufficient evidence for this therapy in improving stroke, renal events, cardiac events, and cardiac and all-cause mortality.
Keywords
Introduction
Renal artery stenosis is caused by atherosclerotic disease in 90% of cases and by fibromuscular dysplasia in 10%. 1 Among patients aged older than 66 years, the incidence of atherosclerotic renal artery stenosis (ARAS) has reached 6.8%. 2 ARAS is defined as at least 50% to 70% stenosis. 3 Hemodynamically significant ARAS is a leading cause of refractory hypertension, progressive deterioration of renal function, ischemic renal events, cardiac diseases, such as aortic syndrome, recurrent hyperemia heart failure, and acute coronary syndrome, and even death.4–7 In patients with refractory hypertension, ARAS is the most common secondary cause of refractory hypertension (2%–5%) which could lead to severe stroke. However, there is frequently no indication of any cause of ARAS.2,8 Approximately more than half of these patients show aggravation of stenosis within 5 years of diagnosis, of whom 15% to 20% develop end-stage renal failure or require replacement therapy. 9 Among patients undergoing cardiac catheterization owing to suspected coronary artery disease, the prevalence of ARAS varies from 25% to 30%.10–14
The treatment of ARAS includes medical therapy and surgery. Currently, open surgery has been increasingly replaced with endovascular surgery because of severe trauma.15,16 Generally, percutaneous transluminal renal angioplasty (PTRA) is regarded as endovascular surgery, and is commonly accompanied by stenting. Nevertheless, the indications of PTRA remain debatable. Previous observational studies have shown that PTRA might be beneficial17–19 or detrimental20,21 to patients with ARAS. Therefore, this systematic review aimed to comparatively assess the effectiveness and safety between best medical therapy (BMT) plus PTRA and BMT alone.
Methods
Search strategy
The review protocol was developed by the steering committee and approved by the ethics review committee of Tianjin Medical University General Hospital. This meta-analysis was registered with PROSPERO (CRD42020150880). The PRISMA statement 22 was followed in our literature research. Following Population, Intervention, Comparison, Outcomes, and Study design, different researchers (Y-HC and H-RP) searched PubMed, EMBASE, Web of Science, Wanfang database, and the Cochrane Library using various combinations of key words, such as “stents”, “endovascular”, “angioplasty”, “drug”, “medicine”, “medical”, “renal”, “kidney”, “stenosis” and “randomized”. Detailed search strategies are shown in Supplemental Tables 1 to 5. We were able to access five databases, including Core Collection, KCI-Korean Journal Database, Medline, Russian Science Citation Index, and SciELO Citation Index through searching the Web of Science. Additionally, a reference search was carried out to identify additional publications by screening reference lists. Only studies written in English were considered in this meta-analysis.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) diagnosis of ARAS; (2) the experimental group was BMT plus PTRA (with stents necessary) and the control group was BMT alone; (3) randomized, controlled trials (RCTs); and (4) published studies. The exclusion criteria included the following: (1) no information was available; (2) there was a significant difference in variables at baseline; (3) repeated publication data; and (4) non-RCTs. Studies that met none of the inclusion criteria or any of the exclusion criteria were excluded.
To ensure the accuracy and completeness of the data, two researchers (Y-HC and H-RP) screened all studies independently. Additionally, a third researcher (G-ZL) intervened in case of dispute arising between inclusion and exclusion criteria.
Data extraction
Data were extracted from the patients at baseline, as well as bias risk indicators, endpoint events, and conclusions. For those studies that lacked some requisite information, the author was contacted by e-mail. We also focused on baseline differences, hemodynamic assessment during follow-up, determination of endpoint events, laboratory or imaging assessment, withdrawal, and funding sources.
Statistical analysis
Review Manager 5.3 software (Cochrane Collaboration, London, United Kingdom) was used for analysis. The quality of selected studies was evaluated using the risk of bias as recommended by the Cochrane instructions. Odds ratios (ORs) and 95% confidence intervals (CIs) were adopted to evaluate the outcomes. The evaluation methods for heterogeneity used in this study included the forest plot (showing Q and I2 statistics) and the funnel chart. The fixed model was applied if I2 was <50%. Conversely, if I2 was >50%, the level of heterogeneity was treated as significant. In this circumstance, the random model was used for meta-analysis. The full text was reviewed to identify the source of the heterogeneity and subgroup analysis was conducted. Subgroup analysis was also implemented in RCTs at different follow-up time and baselines.
Results
Study selection and characteristics
A total of 4410 studies were selected from various online databases, including 1559 articles in PubMed/Medline, 356 articles in Embase, 1271 articles in the Web of Science databases, 1214 articles in the Wanfang database, and 10 articles in the Cochrane Library. One record was identified in a search of references. A total of 9 RCTs (EMMA, 23 SNRASCG, 24 DRASTIC, 25 STAR, 26 RASCAD, 27 CORAL, 28 RADAR, 29 NITER, 30 and ASTRAL 31 ) involving 2309 patients were chosen. Figure 1 shows a flowchart illustrating the search strategy for RCTs on PTRA and BMT in patients with ARAS.

Detailed flowchart showing the search strategy for randomized, controlled trials on percutaneous transluminal renal angioplasty and best medical therapy in patients with atherosclerotic renal artery stenosis.
The baseline participants’ characteristics are shown in Table 1. There was a difference in sample size among the studies. Except for the total sample of the CORAL 28 and ASTRAL 31 studies, which exceeded 800, most of the other studies (EMMA, 23 SNRASCG, 24 RASCAD, 27 and RADAR 29 ) included less than 100 people. With regard to the mean degree of stenosis of the kidney, the RADAR study 29 exceeded 80% and DRASTIC exceeded 70%, while the others showed a similar degree of stenosis >50%. The remaining features were not significantly different among the studies. The patients’ inclusion criteria in each selected study are shown in Table 2.
Participants’ baseline characteristics of nine included randomized, controlled trials.
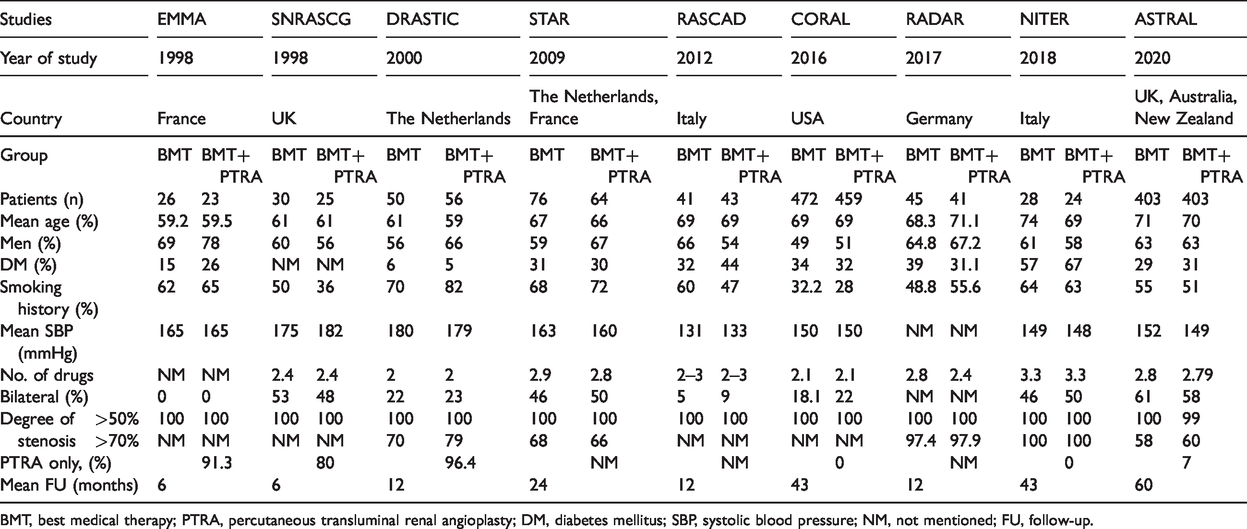
BMT, best medical therapy; PTRA, percutaneous transluminal renal angioplasty; DM, diabetes mellitus; SBP, systolic blood pressure; NM, not mentioned; FU, follow-up.
Brief inclusion criteria in each selected study.

Ccr, creatinine clearance.
Risk of bias
The risk bias of the nine RCTs was determined by the risk of bias as recommended in the Cochrane instructions (Figure 2). Most of the items were identified as low in risk, except for some studies that were assessed as posing a high risk in performance bias and detection bias.

Risk of bias graph of the nine included randomized, controlled trials.
Meta-analysis results
We found that BMT plus PTRA significantly reduced the incidence of refractory hypertension compared with BMT alone within 2 years of follow-up (OR 0.09; 95% CI 0.01, 0.70; P=0.02) (Figure 3). There was no significant difference in stroke at 1 year (OR 0.44; 95% CI 0.11, 1.79) or with at least 2 years of follow-up (OR 0.87; 95% CI 0.57, 1.34) between BMT plus PTRA and BMT alone (Figure 4).

Refractory hypertension within 2 years of follow-up

Stroke in 1 year and with at least 2 years of follow-up
There was no significant difference in renal events at 1 year ( (OR 0.85; 95% CI 0.32, 2.31) or with at least 2 years of follow-up (OR 0.99; 95% CI 0.78, 1.25) between the two groups (Figure 5). There was also no significant difference in renal events in patients with balloon angioplasty only (OR 0.68; 95% CI 0.22, 2.10) or additional stent placement (OR 1.02; 95% CI 0.80, 1.29) (Figure 6).

Renal events in 1 year and with at least 2 years of follow-up

Renal events between balloon angioplasty only and additional stent placement
There was no significant difference in cardiac events within 1 year (OR 0.91; 95% CI 0.42, 1.97) or with at least 2 years of follow-up between the two groups (OR 0.97; 95% CI 0.78, 1.21) (Figure 7). There was also no significant difference in the incidence of cardiac mortality beyond 2 years of follow-up between the two groups (OR 0.90; 95% CI 0.61, 1.32) (Figure 8). There was no significant difference in all-cause mortality at 1 year (OR 0.76; 95% CI 0.23, 2.50) or with at least 2 years of follow-up between the two groups (OR 0.93; 95% CI 0.74, 1.16) (Figure 9).

Cardiac events in 1 year and with at least 2 years of follow-up
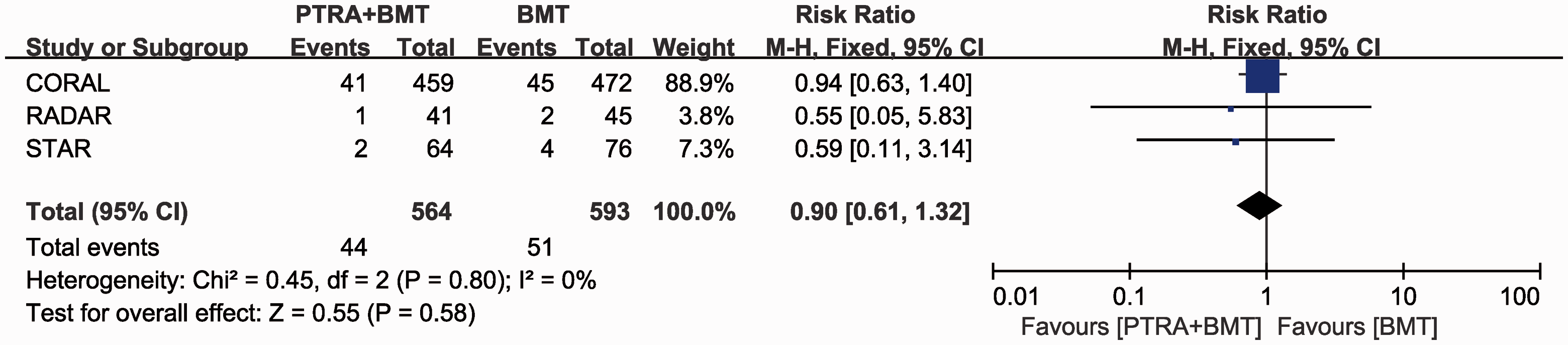
Cardiac mortality after 2 years of follow-up

All-cause mortality in 1 year and with at least 2 years of follow-up
For a degree of ARAS >70%, BMT plus PTRA did not significantly reduce the incidence of renal events at 1 or 2 years of follow-up (OR 1.28; 95% CI 0.52, 3.15) compared with BMT alone (Figure 10). We also found no significant difference in renal events in patients with grade 2 hypertension between the two groups within 2 years of follow-up (OR 0.69; 95% CI 0.35, 1.37) (Figure 11).

Degree of stenosis >70% in 1 year of follow-up
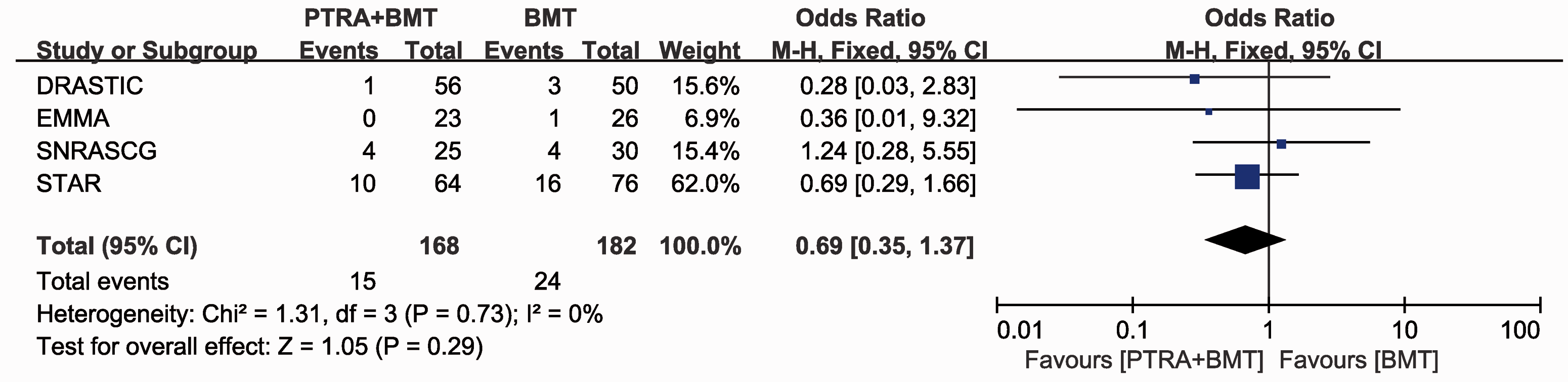
Grade 2 hypertension within 2 years of follow-up
Discussion
In this study, we found that BMT plus PTRA significantly reduced the incidence of refractory hypertension within 2 years of follow-up compared with BMT alone. The ability of BMT plus PTRA to reduce resistant hypertension was proven by three previous RCTs.24,31,32 Our results also support recommendations of the American College of Cardiology and American Heart Association guidelines 33 and the Society for Cardiovascular Angiography and Interventions appropriate use criteria 34 that PTRA is beneficial in patients with resistant hypertension. Many researchers have suggested that patients showing renal blush grade, 36 an abnormal renal frame count,35,36 unstable angina or congestive heart failure,37,38 or flash pulmonary edema 38 have a significantly improved prognosis of hypertension.
In our meta-analysis, there was no reduction in renal events for BMT plus PTRA during the follow-up in patients with balloon angioplasty only, additional stent placement, or grade 2 hypertension. For patients with a degree of stenosis of 70% in the kidney, we still could not find any obvious reduction in renal events. Additionally, renal events resulted from diabetes, nephritis, nephropathy, heart failure, and a solitary functioning kidney. In a previous meta-analysis, 39 7 studies focused on the efficacy of PTRA on patients with a solitary functioning kidney, involving 253 cases. This previous meta-analysis showed that a renal artery stent was beneficial for patients with a solitary functioning kidney regarding improved or stabilized renal function. The benefit rate was 0.77. The authors of some recent retrospective studies40–42 reached the conclusion that PTRA might be conducive to refractory control of blood pressure and kidney function, but only for those with high-risk clinical manifestations, including rapid deterioration of kidney function, episodic pulmonary edema, and post-transplant renal artery stenosis. Nevertheless, our results showed little evidence of the benefits of PTRA in improving renal function.
In our study, we did not find any significant difference in cardiac events, cardiac mortality, or all-cause mortality between PTRA plus BMT and BMT alone. Authors in a previous study found that almost half of the patients who had congestive heart failure had ARAS. 8 Therefore, determining the hemodynamic significance simply by the degree of anatomical stenosis is limited.20,43,44 When ARAS is compounded by heart failure, determining which factor contributes more significantly to the occurrence of renal events is extremely difficult. Some other studies27,45 were unable to detect a clinically significant benefit from PTRA on left ventricular mass in patients with ARAS of 50% to 80%. When stenosis was ≥80% in a recently published RCT, 29 there was improvement in clinical outcomes in cardiac events in 3 years after PTRA. Iwashima et al. 45 found that fibromuscular dysplasia, severe ARAS (≥90%), and a higher left ventricular mass index were independent predictors of better cardiac outcomes.
Several previous meta-analyses evaluated the role of PTRA in ARAS as follows. In a meta-analysis by Natalie et al., 210 patients were recruited from three randomized studies (EMMA, 23 SNRASCG, 24 and DRASTIC 25 ). They showed a more significant reduction in systolic/diastolic blood pressure (P=0.02/P=0.03) and a trend in improvement of creatinine levels in the PTRA arm (P=0.06). Shetty et al. 46 identified five RCTs (EMMA, 23 SNRASCG, 24 DRASTIC, 25 STAR, 26 and ASTRAL 31 ) and discovered an upward trend in systolic blood pressure (P=0.07), diastolic blood pressure (P=0.12), or serum creatinine levels (P=0.07) in patients who underwent PTRA compared with those who had BMT only.
There are some limitations of our review. First, in the studies that we summarized, different criteria were used to select patients for angiography. Therefore, we included a heterogeneous population. Potential confounding factors between randomly assigned treatment groups might have reduced the chance of identifying advantages of PTRA over BMT. Second, some RCTs (EMMA, 23 SNRASCG, 24 DRASTIC, 25 STAR, 26 RASCAD, 27 CORAL, 28 and ASTRAL 31 ) included many patients with stenosis <70% who might not have obtained a benefit from PTRA. Third, the NITER study was terminated prematurely because of an insufficient inclusion. Finally, the criteria to preserve renal function in our included RCTs varied from each other. Therefore, we could not perform a meta-analysis on the effect of PTRA on renal function.
In conclusion, our study shows that PTRA plus BMT reduces the incidence of refractory hypertension, but does not improve the rates of stroke, renal events, cardiac events, cardiac mortality, and all-cause mortality compared with BMT alone. Because of the low strength of the meta-analysis for these findings, we believe that if candidates for PTRA are carefully selected, PTRA will have more effect.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520983585 - Supplemental material for Use of percutaneous transluminal renal angioplasty in atherosclerotic renal artery stenosis: a systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_0300060520983585 for Use of percutaneous transluminal renal angioplasty in atherosclerotic renal artery stenosis: a systematic review and meta-analysis by Yonghui Chen, Hongrui Pan, Guangze Luo, Peng Li and Xiangchen Dai in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_0300060520983585 - Supplemental material for Use of percutaneous transluminal renal angioplasty in atherosclerotic renal artery stenosis: a systematic review and meta-analysis
Supplemental material, sj-pdf-2-imr-10.1177_0300060520983585 for Use of percutaneous transluminal renal angioplasty in atherosclerotic renal artery stenosis: a systematic review and meta-analysis by Yonghui Chen, Hongrui Pan, Guangze Luo, Peng Li and Xiangchen Dai in Journal of International Medical Research
Footnotes
Acknowledgement
We thank Dr. Song from the Department of Urology for proofreading the manuscript in a professional manner.
Author contributions
Research idea and study design: Y-HC, H-RP, and X-CD; data acquisition: Y-HC and H-RP; data analysis/interpretation: H-RP; statistical analysis: Y-HC and H-RP; manuscript writing: Y-HC, H-RP, G-ZL, and X-CD.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.