
Abstract
Objective
This study was performed to evaluate the surgical indications, clinical efficacy, and preliminary experiences of nonstructural bone grafts for lumbar tuberculosis (TB).
Methods
Thirty-four patients with lumbar TB who were treated with nonstructural bone grafts were retrospectively assessed. The operative time, operative blood loss, hospital stay, bone graft fusion time, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) concentration, visual analog scale (VAS) score, Oswestry Disability Index (ODI), American Spinal Injury Association (ASIA) impairment grade, and Cobb angle were recorded and analyzed.
Results
The mean operative time, operative blood loss, hospital stay, Cobb angle correction, and Cobb angle loss were 192.59 ± 42.16 minutes, 385.29 ± 251.82 mL, 14.91 ± 5.06 days, 9.02° ± 3.16°, and 5.54° ± 1.09°, respectively. During the mean follow-up of 27.53 ± 8.90 months, significant improvements were observed in the ESR, CRP concentration, VAS score, ODI, and ASIA grade. The mean bone graft fusion time was 5.15 ± 1.13 months. Three complications occurred, and all were cured after active treatment.
Conclusions
Nonstructural bone grafts may achieve satisfactory clinical efficacy for appropriately selected patients with lumbar TB.
Keywords
Introduction
Spinal tuberculosis (TB) is the most common type of extrapulmonary TB, accounting for about 50% of osteoarticular TB. 1 Spinal TB mostly occurs in the lower thoracic and lumbar vertebrae, resulting in vertebral body destruction, collapse, kyphosis, and even paralysis. 2 Surgical treatment of TB is mainly suitable for patients with spinal instability, severe kyphosis, or impaired neurological function. 3
Radical debridement is the key to successful spinal TB surgery because it helps to control TB lesions, improve the effect of anti-TB chemotherapy, promote bone graft fusion, and reduce the risk of TB recurrence. 4 At present, the most commonly used bone grafts in spinal TB surgery are autogenous iliac bone grafts and titanium mesh bone grafts. 5 Although these two bone graft methods have achieved high bone fusion rates and satisfactory clinical efficacy, increasingly more attention is being paid to associated surgical problems such as donor site complications, titanium mesh subsidence, and major surgical trauma.6,7 Thus, many surgeons are looking for a new bone graft method that can reduce surgical trauma and complications.
In recent years, the use of nonstructural bone grafts has produced satisfactory clinical efficacy in spinal fusion surgery. 8 Our previous study showed that nonstructural bone grafts have the advantages of less surgical trauma and a shorter bone fusion time than iliac bone grafts and titanium mesh bone grafts in the surgical treatment of single-segment thoracic TB. 9 Therefore, nonstructural bone grafts are expected to become a general bone graft technique in spinal TB surgery. However, some spinal surgeons have wondered whether these positive results can be extrapolated to the lumbar TB surgery population because the lumbar spine sustains a greater loading force than the thoracic spine and is devoid of the protection of the rib cage.
The use of nonstructural bone grafts to repair bone defects in lumbar TB surgery has been rarely reported. Xu et al. 10 reported that the mean bone graft fusion time was 5.1 months among 32 patients with monosegmental lumbar spinal TB undergoing compact bone grafting. Liu et al. 11 described 21 patients with lumbosacral spinal TB who received nonstructural bone grafts, and all patients achieved bone fusion within 6 months postoperatively; however, this study only included patients with spinal TB at the L5/S1 segment. Additionally, the two abovementioned studies mainly concentrated on imaging outcomes (such as the Cobb angle); the clinical outcomes were rarely reported. Moreover, neither study specifically identified the surgical indications for the use of nonstructural bone grafts for lumbar TB, which may result in confusion among spinal surgeons and limit the application of this technique.
Therefore, we conducted the present retrospective cohort study not only to evaluate the clinical efficacy and safety of nonstructural bone grafts in patients with single-segment lumbar TB but also to specify the surgical indications for this bone graft method.
Material and methods
This retrospective cohort study was approved by the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University (2017-067). All of the participants provided written informed consent to participate in this study before their data were used for research purposes. The work is reported in line with the STROBE criteria. 12 All details that may identify the patients have been de-identified in this study.
Patient selection
The medical records of hospitalized patients who were diagnosed with spinal TB in our department from January 2015 to December 2017 were retrospectively analyzed.
The inclusion criteria were as follows: (1) preoperative diagnosis of spinal TB; (2) age of >18 years; (3) single-segment lumbar TB (L1/2–L4/5); (4) surgical treatment by one-stage posterior debridement, bone graft fusion, and internal fixation; (5) use of a nonstructural bone graft (autologous granular bone graft) during surgery; (6) follow-up time of >12 months; and (7) availability of complete clinical and imaging data.
The exclusion criteria were as follows: (1) suspected spinal TB without a pathological diagnosis; (2) multisegmental spinal TB, cervical or thoracic spine TB, or other types of TB; (3) history of spinal surgery; and (4) spinal TB with active pulmonary TB, a malignant tumor, or other severe conditions.
Preoperative management
All patients were treated with regular anti-TB chemotherapy (rifampicin at 450 mg/day, isoniazid at 300 mg/day, pyrazinamide at 1500 mg/day, and ethambutol at 750 mg/day) for at least 2 weeks preoperatively. All patients underwent X-ray, computed tomography (CT), and magnetic resonance imaging examinations and laboratory tests after admission. The preoperative sagittal Cobb angle was also measured on lateral X-ray examination. Surgery was performed when the symptoms of TB poisoning (such as low fever, night sweats, and wasting) had been relieved, the erythrocyte sedimentation rate (ESR) had returned to normal or significantly decreased, and any underlying diseases such as diabetes, coronary heart disease, or hypertension were under control. However, if the patient developed rapid deterioration of neurological function, the surgery was performed immediately.
Surgical procedure
The patients were placed in the prone position after induction of general anesthesia, and a longitudinal midline incision was made. The sacrospinalis was then stripped off the lamina, and the facet joints on the contralateral side were exposed through the Wiltse approach. 13 Pedicle screws were inserted into the one or two normal vertebrae superior and inferior to the lesion segment, and the titanium rod of the non-debridement side was temporarily locked. Unilateral laminectomy was performed to clear off the caseous necrotic tissue, pus, granulation tissue, sequestrum, and necrotic disc. The paravertebral or psoas abscess was then drained using a soft catheter tube inserted into the abscess cavity.
The vertebral plate harvested during surgery was converted into 3- to 5-mm granular bone fragments, implanted into the vertebral space, and tamped down. If the local bone particle volume was too low, another 3-cm-long incision was made along the posterior superior iliac spine to expose the iliac crest, and the cancellous bone was removed to create bone particles. The posterior margin was covered with a gelatin sponge containing isoniazid to prevent bone graft particles from entering the spinal canal. Finally, the rods were locked. Streptomycin (1.0 g) and isoniazid (0.3 g) were placed in the lesion, two drainage tubes were placed in the incision, and the incision was closed layer by layer. The pathological materials taken from the lesion site were sent for culture and pathological examination.
Postoperative management
Antibiotics were prophylactically administered for the first 3 days after surgery, and the preoperative anti-TB chemotherapy was continued for 18 to 24 months. The incision drain was removed when the drainage volume was <40 mL/day, and an X-ray examination was performed after extubation. One week after surgery, the patients were allowed to get out of bed while wearing braces, the application of which was continued for 3 months. An X-ray examination; measurement of the ESR, C-reactive protein (CRP) concentration, and hepatic and renal function; and CT and magnetic resonance imaging examinations (if necessary) were performed 1, 3, 6, and 12 months postoperatively. The postoperative and follow-up sagittal Cobb angle was measured on a lateral X-ray.
Outcome assessment
The following clinical outcomes were assessed: (1) operative time, operative blood loss, and hospital stay; (2) visual analog scale (VAS) score and Oswestry Disability Index (ODI); (3) ESR and CRP concentration preoperatively and at the last follow-up; (4) neurological function preoperatively and at the last follow-up using the American Spinal Injury Association (ASIA) impairment grade; and (5) complications throughout follow-up.
The following imaging outcomes were assessed: (1) the Cobb angle preoperatively, postoperatively, and at the final follow-up as measured on a lateral X-ray (the Cobb angles of lordosis and kyphosis of the surgical segments are expressed as positive and negative values, respectively) and (2) the bone graft fusion time. The criterion reported by Bridwell et al. 14 was used to evaluate whether bone fusion had been achieved according to the CT scan during follow-up. Grade I and II were defined as bone graft fusion in this study.
Statistical analysis
IBM SPSS Statistics for Windows, Version 19.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Quantitative data are expressed as mean ± standard deviation. A paired t-test was used for intragroup comparison of quantitative data. The Mann–Whitney rank sum test and χ2 test were used for intragroup comparison of ordered and disordered qualitative data, respectively. A P value of <0.05 was considered statistically significant.
Results
Thirty-four patients were included in this study. Their mean age, body mass index, operative time, operative blood loss, and hospital stay were 39.71 ± 15.75 years, 21.31 ± 2.06 kg/m2, 192.59 ± 42.16 minutes, 385.29 ± 251.82 mL, and 14.91 ± 5.06 days, respectively. The mean Cobb angle correction and Cobb angle loss were 9.02° ± 3.16° and 5.54° ± 1.09°, respectively (Table 1).
Patients’ general characteristics.

Data are presented as n or mean ± standard deviation.
The mean follow-up time was 27.53 ± 8.90 months, and the ESR, CRP concentration, VAS score, and ODI were significantly lower at the final follow-up than preoperatively (P < 0.001). The ASIA grade was also significantly improved at the final follow-up (P = 0.004). The mean Cobb angle was 15.07° ± 3.95° preoperatively and significantly increased to 18.74° ± 5.43° at the final follow-up (P < 0.001). The mean bone graft fusion time was 5.15 ± 1.13 months (Table 2).
Comparison of clinical and radiological outcomes between preoperative period and final follow-up.
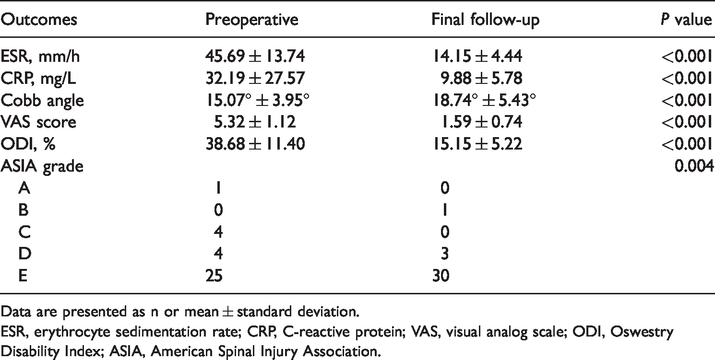
Data are presented as n or mean ± standard deviation.
ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; VAS, visual analog scale; ODI, Oswestry Disability Index; ASIA, American Spinal Injury Association.
Three patients developed postoperative complications (hepatic function damage in two and renal function damage in one). All complications were cured after active treatment.
Discussion
The operative time and operative blood loss of nonstructural bone grafts in the present study were similar to those reported by Xu et al., 10 but they were significantly less than those of iliac bone grafts and titanium mesh bone grafts in our previous study. 15 Three possible reasons for these differences are as follows. (1) Iliac bone grafts and titanium mesh bone grafts have a high requirement for the bone grafting bed, requiring extensive removal of bone tissue during the surgery. 16 (2) It may be difficult to implant an iliac bone mass or titanium mesh into the intervertebral space because of its large volume or sharp edge, whereas granular bone is small and convenient to implant. (3) The titanium mesh is serrated and does not easily slip after implantation; therefore, if the model is unsatisfactory, it is difficult to remove during surgery.
The mean bone graft fusion time was 5.15 ± 1.13 months in our study, which is similar to the times reported in the studies by Xu et al. 10 and Liu et al. 11 but significantly shorter than that of iliac bone graft and titanium mesh bone graft repair reported in another previous study. 15 Two possible reasons for these differences are as follows. (1) The contact area between the granular bone and vertebral body was large because of the small volume of the granular bone, and this may be beneficial to nutrient infiltration and neovascularization. 17 (2) The implanted granular bone can induce proliferation of peripheral bone mesenchymal cells, secrete bone morphogenetic protein, and promote osteogenesis. 18
The main concerns regarding nonstructural bone grafts used in lumbar spinal TB surgery are the insufficient supporting force and poor ability to correct kyphosis because of the loose structure of the graft.10,11 In our study, the Cobb angle correction was satisfactory and similar to the results reported by Xu et al. 10 A possible reason is that the correction of kyphosis deformity mainly depends on the posterior pedicle nail–rod system rather than the support of the anterior column. 19 However, the Cobb angle loss was more severe than that reported by Xu et al., 10 which may be explained as follows. (1) The patients in the study by Xu et al. 10 were asked to stay in bed for 4 weeks postoperatively, while in our study, the patients were allowed to get out of bed only 1 week after surgery. (2) A brace was used for at least 12 months postoperatively in the study by Xu et al., 10 but it was used for only 3 months in our study. (3) In some patients in our study, the bilateral lamina and spinous processes were removed during the surgery, which may have affected the stability of the lumbar spine. 20 (4) Granular bone is easily absorbed because of its small volume. 21 (5) The difference in the length of the posterior fixation segment may also affect local stability and the Cobb angle loss.19,22 However, Cobb angle loss does not necessarily indicate poor improvement of clinical symptoms.
The ESR, CRP concentration, VAS score, ODI, and neurological function were all significantly improved at the final follow-up compared with preoperatively, similar to the findings in previous studies.9–11 This may be due to the effectiveness of anti-TB chemotherapy, radical TB lesion debridement, and spinal canal decompression. 23 The improvements in clinical outcomes may indicate that although the Cobb angle loss after nonstructural bone graft repair in lumbar TB surgery is greater, it does not affect patients’ clinical symptoms or control of TB lesions. This result may be related to the short bone graft fusion time of nonstructural bone grafts because after bone graft fusion, the loss of the Cobb angle is reportedly mild and does not negatively affect the clinical outcome.9,15
Although the incidence of complications of nonstructural bone graft repair in this study (8.8%) was higher than that reported by Liu et al. 11 (4.8%), no serious complications occurred. The main complications in this study were hepatic and renal function damage, which were mainly related to the long-term anti-TB chemotherapy. All cases were cured after active treatment, which also indicates the safety of nonstructural bone grafts in lumbar spinal TB surgery.
In our previous study, we considered that the indication for use of nonstructural bone grafts in single-segment thoracic TB was bony destruction of <50% of the vertebral height. 9 Therefore, when we initially applied nonstructural bone grafts to lumbar TB, these grafts were also mainly applied to patients with vertebral bone destruction of <50% (Figure 1). However, with increases in cases and surgical experience, we found that nonstructural bone grafts also had satisfactory clinical efficacy in some cases of lumbar TB with vertebral bone destruction of >50% but with no serious bone cortical destruction and in which the pedicle screws could be implanted in at least one side of the affected vertebra (Figure 2). We believe that two possible reasons for this are as follows. (1) If the cortical bone is relatively complete, the stability of the spinal anterior column may be not seriously destroyed. (2) The posterior pedicle screw system is a type of three-column fixation that can effectively maintain the stability of the spinal anterior column and is conducive to bone graft fusion. 22

A 46-year-old man with L2/3 spinal tuberculosis who underwent nonstructural bone graft repair. (a–d) Preoperative computed tomography showed that the L5 vertebral body and the L2/3 intervertebral disc were destroyed (<50% of the height of the vertebrae). (e, f) Postoperative X-ray. (g–j) Computed tomography at 5 months postoperatively showed bone fusion between L2 and L3, and X-ray examination showed good location of the posterior instrument. (k, l) X-ray at 24 months postoperatively showed good location of the posterior instrument.

A 29-year-old woman with L1/2 spinal tuberculosis who underwent nonstructural bone graft repair. (a–d) Preoperative computed tomography showed that the L1/2 vertebral body and the L1/2 intervertebral disc were destroyed (>50% of the height of the vertebrae), but the cortical bone was still complete and the pedicle screws could be implanted in both sides of the L1 and L2 vertebrae. (e, f) Postoperative X-ray. (g–j) Computed tomography at 5 months postoperatively showed bone fusion between L1 and L2. (k, l) The posterior instrument was removed at 20 months postoperatively.
Therefore, we consider that the indications for one-stage posterior debridement, nonstructural bone graft repair, and internal fixation for single-segment lumbar TB are as follows: (1) progressive aggravation of neurological impairment or local instability or kyphosis deformity; (2) single-segment lumbar TB with (a) bony destruction of <50% of the height of the vertebrae or (b) bony destruction of >50% of the height of the vertebrae, but with no serious bone cortical destruction and the ability to implant pedicle screws into at least one side of the affected vertebra; and (3) localization of the TB lesion mainly in the former column with no involvement of the posterior column.
Based on our experience with successful nonstructural bone graft repair in lumbar TB surgery, we recommend the following. First, unilateral laminectomy rather than bilateral laminectomy should be performed, and the spinous process and posterior ligamental complex should be retained during the surgery to preserve the local stability. Second, during debridement of the TB lesions, the sclerotic bone and bone bridge between the anterior edge of the vertebral bodies should be preserved. Third, rigid pedicle screw fixation should be guaranteed with either no or only mild distraction of the vertebral interspace.
This study had three main limitations. First, this was a single-center retrospective study. Second, the sample size was small and the follow-up time was short. Third, the surgeons had different levels of experience and thus may have had different surgical experiences with granular bone grafts.
In summary, the use of nonstructural bone grafts may achieve satisfactory clinical efficacy in alleviating symptoms, correcting kyphosis, and improving neurological function for appropriately selected patients with single-segment lumbar TB. Because of the potential limitations of this study, prospective comparative studies with long-term follow-up are needed to validate our findings.
Supplemental Material
sj-pdf-1-imr-10.1177_0300060520982780 - Supplemental material for Nonstructural bone graft for single-segment lumbar tuberculosis: surgical indications, clinical efficacy, and preliminary experiences in 34 patients
Supplemental material, sj-pdf-1-imr-10.1177_0300060520982780 for Nonstructural bone graft for single-segment lumbar tuberculosis: surgical indications, clinical efficacy, and preliminary experiences in 34 patients by Xing Du, Yunsheng Ou, Guanyin Jiang, Yong Zhu, Wei Luo and Dianming Jiang in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Chongqing (No. cstc2019jcyj-msxmX0358) and the Achievement Transformation Project of Chongqing Education Committee (No. KJZH17110).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.