
Abstract
Intravenous misplacement of the nephrostomy catheter following percutaneous nephrostolithotomy (PCNL) is extremely rare, and little information is available about this complication. Because the patient’s prognosis may be poor, sufficient attention should be paid to early identification and treatment of this complication. We present an uncommon case of a patient with intravenous nephrostomy catheter misplacement after PCNL at our hospital. In our patient, the tip of the nephrostomy catheter was located in the inferior vena cava. It was successfully managed using two-step catheter withdrawal under fluoroscopy, and the percutaneous nephrostomy catheter was able to be withdrawn 7 to 8 cm back into the collecting system in stages with the surgical team on standby. There were no severe complications such as deep vein thrombosis that developed during or after the catheter withdrawal. Patients could be managed conservatively using intravenous antibiotics, strict bed rest, and tube withdrawal using computed tomography (CT) or fluoroscopy guide in most cases combined with information in the literature. Additionally, open surgery could be used as an alternative treatment.
Keywords
Introduction
Percutaneous nephrolithotomy (PCNL) is an important approach to use when removing kidney stones, and it was introduced by Fernström and Johansson in 1976. 1 It is a minimally invasive procedure to remove kidney stones that are larger than 2 cm in size. 2 PCNL is safe and effective in most cases, but it can be associated with uncommon complications. 3 To stop bleeding and drain fluid and urine from the collecting system after surgery, retaining a nephrostomy catheter in the renal pelvis is a routine procedure. 4 However, intravenous misplacement of the nephrostomy catheter is a rare complication that is associated with PCNL.4,5 A report by Fu et al. 4 showed that the incidence of intravenous nephrostomy tube misplacement after PCNL was 0.23 per thousand. Improper treatment was administered to patients with this complication, which may lead to serious consequences such as perforation, infection, hemorrhage, and embolization.6,7 It is very important to completely understand early identification and treatment options for this complication. However, few publications about intravenous misplacement of a nephrostomy tube have been reported.
We report the case of a patient in whom surgery was stopped because of excessive bleeding, and the nephrostomy tube was retained and clamped during PCNL. In this procedure, the nephrostomy tube passed through the renal parenchyma and renal vein and into the inferior vena cava (IVC). We also performed a literature review of previous cases.
Case report
A 58-year-old male patient was admitted to hospital because of right kidney calculi that were found during a routine examination over 3 months before hospital admission. Relevant examinations such as a plain X-ray of the abdomen (KUB) (Figure 1), intravenous urography (IVU), and abdominal computed tomography (CT) were performed after admission to our hospital. Percutaneous nephrostomy was performed to remove the stone. The prone position was used to perform the PCNL. Between the posterior axillary line and scapular line, the puncture site was localized to the 11th intercostal space. Percutaneous punctures that were guided by ultrasound were performed using an 18-gauge needle. Urine in the renal pelvis was not completely aspirated after the puncture. A zebra guide wire was inserted into the collecting system. We judged that the guide wire should be coiled in the renal pelvis after a successful puncture. Access to the excretory system was achieved gradually by fascial dilators ranging from the smallest size to 20F. Severe bleeding from the sheath immediately after dilator removal led to a sudden interruption of the procedure. An 18 F nephrostomy catheter was promptly inserted and closed to control the bleeding.

Preoperative plain film of the abdomen (KUB).
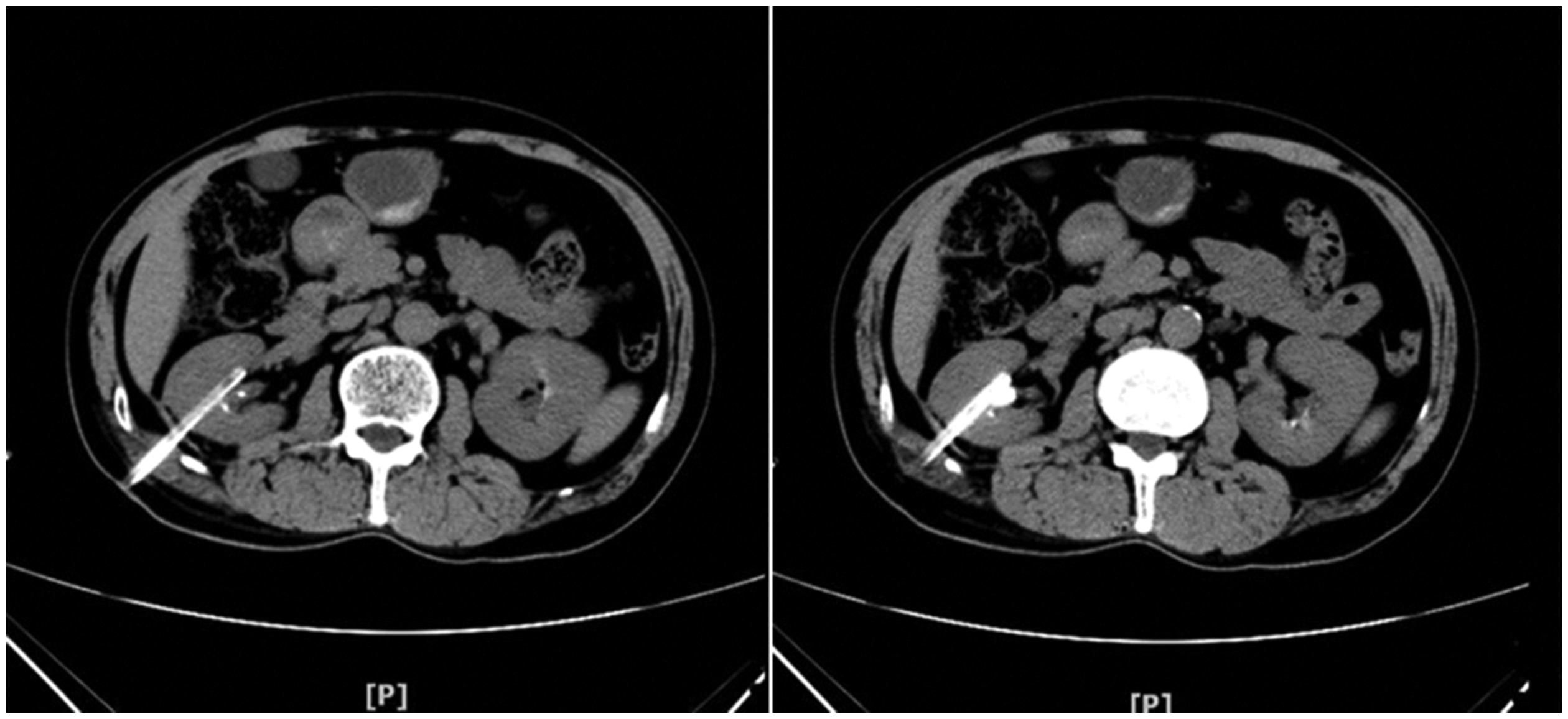
A quick nephrostogram was not performed after placement of a nephrostomy tube to locate the position of the nephrostomy tube. Blood loss was estimated to be from 400 to 500 mL, which was mainly due to outflow from the fistula channel via the skin of the nephroscope, and it was mixed with some flushing water and urine. Hemoglobin levels decreased by 15 g/L after surgery, and the patient also had mild hematuria. His blood pressure did not decrease. We thought that the bleeding was caused by damage to the renal parenchyma and microvascular structures. A plain CT scan of the kidney that was performed 5 days after surgery showed that there was a great possibility that the nephrostomy catheter had traversed from the middle to lower pole of the right kidney directly into the right renal vein and ending in the IVC (Figure 2).

Plain computed tomography (CT) scan of the kidney after 5 days of the percutaneous nephrostomy (PCNL).
Abdominal computed tomography angiograph (CTA) and three-dimensional reconstruction (Figure 3) were immediately applied to assess the patient’s specific condition, which revealed that the nephrostomy tube had pierced the renal parenchyma, entered the right renal vein, and extended up into the IVC. We immediately ordered the patient to remain on strict bed rest until 2 weeks after surgery. In the postoperative 2 weeks, the nephrostomy tube was withdrawn from IVC and right renal vein into the collecting system, guided by X-ray with interventional treatment, and during this time, a surgical team was on emergency standby. Right renal artery, right renal vein, and IVC angiography were performed during the catheter withdrawal. The tube withdrawal process was smooth and no bleeding occurred, and the patient’s postoperative course was uneventful. Five days after the catheter was withdrawn into the collecting system, the patient underwent an unenhanced CT (Figure 4). He was discharged on day 7 after tube withdrawal, and the residual stones were treated using PCNL 1 month after discharge.

Abdominal computed tomography angiograph (CTA) and three-dimensional reconstruction to show the position of the catheter.
Unenhanced computed tomography (CT) of the kidney 5 days after the catheter was withdrawn into the collecting system.
Discussion
Although PCNL is a routine procedure, some complications including kidney or adjacent organ (such as the liver, spleen, and bowel) injury, sepsis, hemorrhage, excretory system perforation, or access loss, are possible during or after PCNL. 4 Among these PCNL complications, hemorrhage is the most significant complication. Generally, venous bleeding is mild during the PCNL procedure, and it can stop spontaneously or require that a nephrostomy tube be left in the renal pelvis.4,8 The complication of severe bleeding during percutaneous procedures is mainly associated with arterial injuries.4,9 Leaving the nephrostomy catheter in the renal pelvis is an effective method to stop venous bleeding.9,10 However, the tube can occasionally pierce the renal parenchyma and migrate into the renal vein and even into the IVC.9,10 Several publications have shown rare complications that are related to nephrostomy tube misplacement into the vessel following PCNL.2,4,5,9,11–15 The data from these publications are summarized in Table 1.
Reports on managing intravenous migration of a nephrostomy tube.

*The patients developed deep vein thrombosis.
PCNL, percutaneous nephrostolithotomy; M, male; F, female; L, left; R, right; IVC, inferior vena cava; ESWL, extracorporeal shock wave lithotripsy; NA, not available.
Controllable bleeding is a common complication during PCNL.2,4,9 However, the nephrostomy tube that was used to control the bleeding was inadvertently inserted into the venous system, including into the IVC, resulting in rare complications, 2 which have been attributed to anatomical and subjective factors. The anatomical, or objective, factors include multiple branches of the renal vein, many collateral anastomoses of the venous system, anterior and posterior grouped veins with communicating branches in the fornix, the funnel part wrapped by a vein, co-infection, and inflammation. These factors cause the kidney tissues to become vulnerable by isolating the kidney, which leads to compensatory hypertrophy with an abundant blood supply, and the kidney is also vulnerable to stones that are embedded in the target calyx. The subjective or surgical factors include blind puncture dilatation, the guide wire penetrating the vein, vibration, and tearing of the working sheath, which result in venous rupture, and intraoperative bleeding, which leads to blurred vision.
A search of relevant databases showed that 13 patients developed this rare complication, not including our patient.2,4,5,9,11–15 The previous cases2,4,5,9,11–15 showed that, even if there was a perforation into the major renal vein, the hemorrhage could be controlled by the placement of a nephrostomy tube. Intravenous misplacement of the nephrostomy catheter was a rare complication that was associated with PCNL.4,5 There were five cases5,11,13,15 in which the tracts were allowed to heal and the nephrostomy catheter was withdrawn in stages under fluoroscopic guidance. The nephrostomy tube was removed using other methods in seven patients,2,4,5,9,12,13 and one case report 14 did not state the method that was used for nephrostomy catheter withdrawal. Three patients who were reported by Fu et al. 4 and Kotb et al. 2 were treated with open pyelotomy or ureterolithotomy to withdraw the nephrostomy catheter. Wang et al. 9 reported the case of a patient in whom there was intravenous nephrostomy catheter misplacement and subsequent pseudoaneurysm after PCNL. Throughout treatment, antithrombotic therapy was used in only three cases.4,11,15 Among all cases, only one patient developed a deep vein thrombosis. 2 All of the patients2,4,5,9,11–15 were successfully managed using one-step or two-step catheter withdrawal under close monitoring.
In our patient, intravenous nephrostomy catheter misplacement was successfully managed using a two-step catheter that was withdrawn under fluoroscopy. The percutaneous nephrostomy catheter was withdrawn 7 to 8 cm back into the collecting system in stages with a surgical team on standby. The withdrawal distance could vary depending on the patient and the catheter position. There were no severe complications such as a deep vein thrombosis that developed during or after catheter withdrawal.
Conclusions
Intravenous misplacement of the nephrostomy catheter following percutaneous nephrostolithotomy is extremely rare, and little information is available about this complication. Because the patient’s prognosis may be poor, sufficient attention should be paid to the early identification and treatment of this complication. In addition, patients could be managed conservatively with intravenous antibiotics, strict bed rest, and tube withdrawal using CT or fluoroscopy as a guide, in most cases, and this could be combined with information from the literature. However, open surgery could be applied as an alternative treatment.
Footnotes
Consent to participate
The patient provided informed consent for the use of his imaging data and publication of this case.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.