
Abstract
Scalp congenital hemangiomas are a rare, but well-known, vascular malformation in infants. These hemangiomas are usually benign, but occasionally these are associated with cardiac complications and disfigurement. Giant hemangiomas that are associated with high-output heart failure require intervention because they have a high mortality rate and do not respond to medical therapy. We report here a case of a premature newborn who was diagnosed with a giant scalp hemangioma associated with cardiac failure. The newborn underwent successful arterial feeder embolization of the superficial temporal artery. He then underwent surgical excision 14 days after embolization. We believe that preoperative embolization of a giant scalp hemangioma in newborns is a safe measure for alleviating underlying cardiac failure and minimizing the risk of intraoperative bleeding.
Keywords
Introduction
Infantile hemangiomas (IHs) are among the most common soft tissue tumors that occur in infancy, especially in premature infants with a low birth weight.1,2 These tumors are frequently found in the head and neck (60%), followed by the trunk (25%) and extremities (15%). 3 Based on their clinical course, IHs are classified into rapidly involuting congenital hemangiomas (RICHs) and non-involuting congenital hemangiomas (NICHs). 4 Most congenital hemangiomas (CHs) do not require treatment in the early postnatal period. Nonetheless, surgical intervention is indicated for scalp IHs, especially when life-threatening complications are expected. 4 Giant hemangiomas that are associated with high-output heart failure require intervention because they have a high mortality rate and do not respond to medical therapy. 5
We report a case of a premature newborn who was diagnosed with a giant scalp hemangioma associated with cardiac failure. He underwent preoperative endovascular treatment and surgical excision.
Case presentation
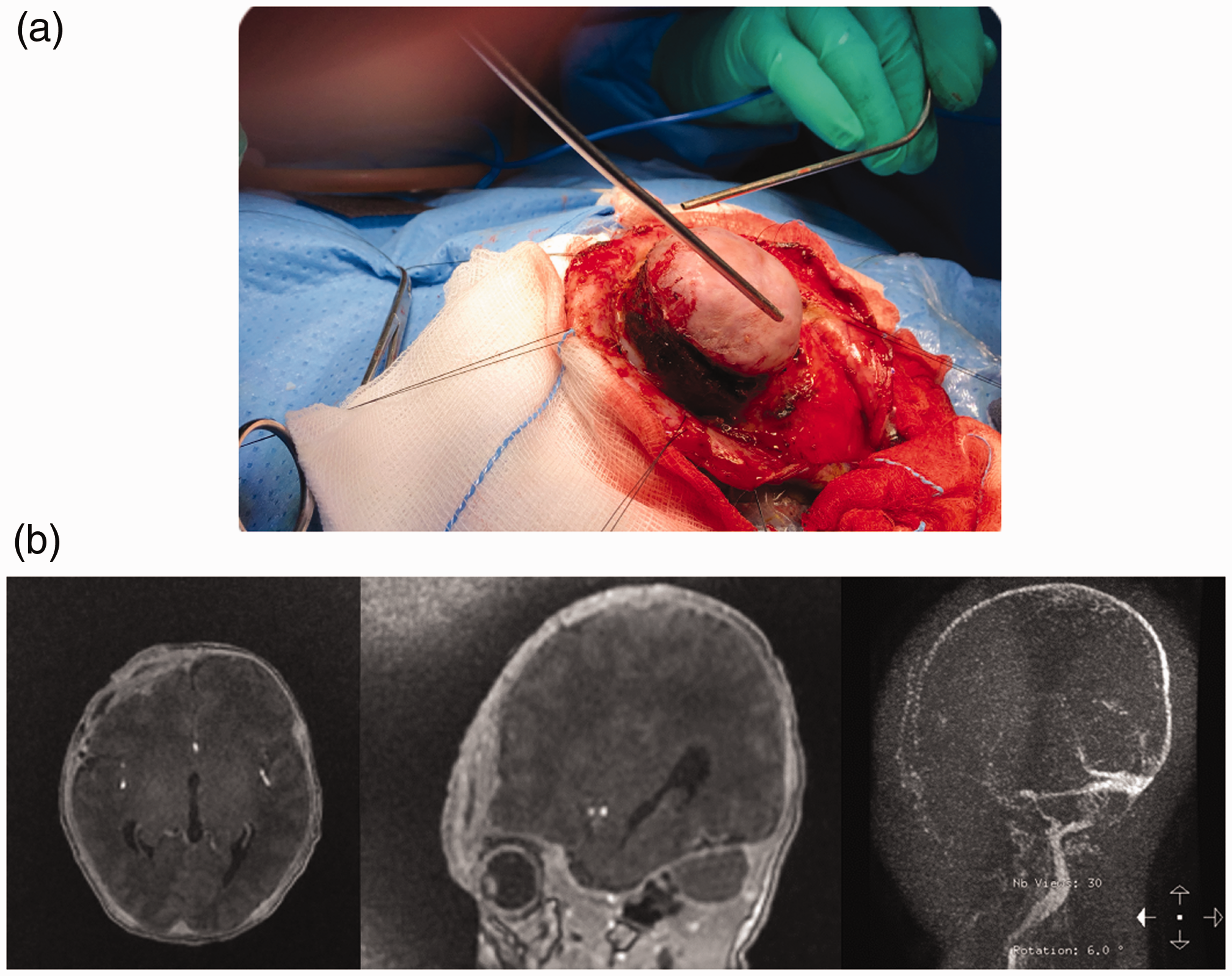
A 1-day-old premature male newborn (35 weeks’ gestational age; birth weight of 2420 g) was delivered by emergency cesarean section. He presented at our Pediatric Neurosurgery Department with a giant right frontal supraorbital scalp hemangioma, which caused pulmonary hypertension and heart failure. A physical examination showed a huge lesion in the right frontal supraorbital area. The lesion was firm with abnormal discoloration at its apex. The circumference of the lesion was 23 cm and it was surrounded by dilated engorged veins that compressed the right eye lid (Figure 1a). The patient was intubated owing to inability to maintain saturation, apnea episodes, bradycardia, and pericardial effusion. A chest X-ray showed moderate to severe cardiomegaly (Figure 1b). An echocardiogram showed biventricular enlargement, volume overload, pulmonary hypertension, and pericardial effusion. Brain magnetic resonance imaging showed an extracranial, high-flow, vascular mass in the right frontal region with erosion of the underlying right frontal bone and local dural thickening (Figure 2a). The high-flow vascular mass was supplied by the external carotid artery and partially supplied by the right middle cerebral artery with early draining veins noted in the venous phase (Figure 2a). The patient underwent emergent angiography owing to a deteriorating condition of the heart. Angiography showed highly vascular lesions that were supplied by branches from the external carotid artery and internal carotid artery, but they were mainly supplied from the superficial temporal artery (Figure 2b). Successful arterial feeder embolization of the superficial temporal artery using Onyx (Medtronic, Minneapolis, MN, USA) was achieved. Postembolization images showed decreased vascularity of the lesion with remaining supply from the internal carotid artery branches (Figure 2c).
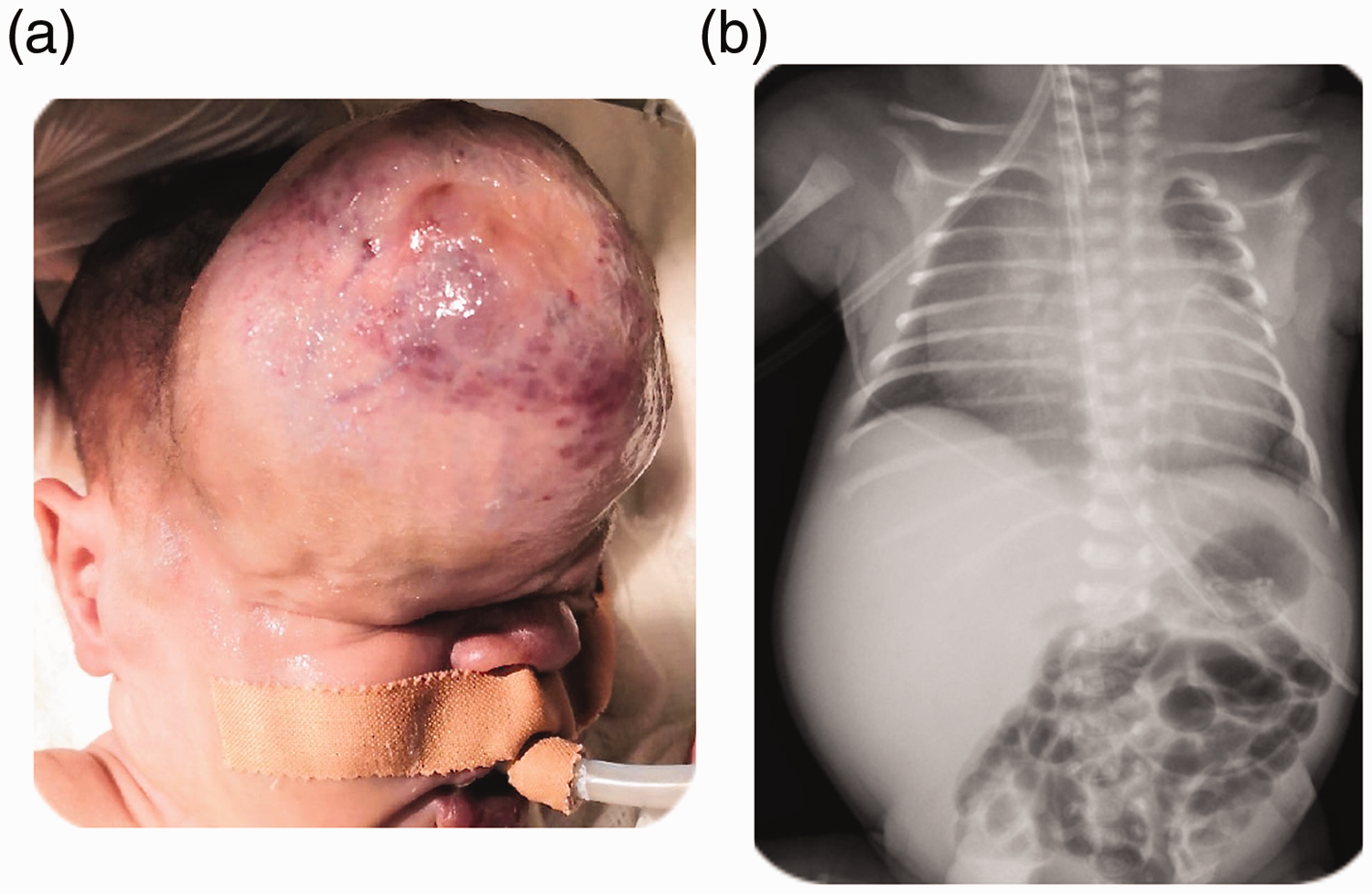
Image of a giant right frontal supraorbital scalp hemangioma (a). Chest X-ray shows moderate to severe cardiomegaly (b).

Brain magnetic resonance imaging shows an extracranial, highly vascular, fast-flow mass in the right frontal region (a). Cerebral angiography shows a highly vascular lesion supplied by branches from the external carotid artery and internal carotid artery, but it is mainly supplied from the superficial temporal artery (b). Postembolization images show a decrease in vascularity of the lesion with remaining supply from branches of the internal carotid artery (c). The circumference of the lesion decreased from 23 to 18 cm at 14 days postembolization (d).
Unfortunately, the patient’s right lower limb became pale with weak pulses postembolization. Ultrasound Doppler of the right lower limb showed spasms in the right external iliac artery, right common femoral artery, and proximal right superficial femoral artery without evidence of thrombosis. Vascular surgery, neurointervention, and hematology teams were consulted. Following conservative management, heparin was initiated at a therapeutic dose. A few days later, his leg vascularity improved with no permanent injury. Within 14 days postembolization, the circumference of the lesion had decreased from 23 cm to 18 cm (Figure 2d).
The patient’s cardiac function improved after embolization. He underwent surgical resection 14 days after embolization and discontinuation of heparin (Figure 3a). Total resection of the lesion with minimal blood loss was achieved (Figure 3b). Postoperatively, the patient was extubated, and he maintained saturation in room air. All diuretics and anti-heart failure medication were weaned off and discontinued before discharge. He was discharged 1 week after surgery. The histopathological diagnosis was RICH.
Intraoperative image (a). Postoperative magnetic resonance imaging shows complete resection (b).
Discussion
Infantile CHs are rare, fully developed lesions. 6 This condition begins in the first few months of birth with a rapid proliferative phase of the vascular endothelium followed by a slow regression phase, which starts between 12 and 15 months of birth and continues up to 7 years of age. 2 These CHs are classified into the two major types: RICH and NICH. 7 NICHs grow with age, while RICHs are self-resolving and require no treatment. 8 Infantile scalp CHs are more challenging to manage and require careful surgical planning than those in other regions because of their location and the potential risk of functional morbidity and aesthetic outcomes.2,7 Surgical treatment for scalp CHs is indicated when there is bleeding, ulceration, hemodynamic instability, disfiguring deformity, or compromised vision.2,8
The association of heart failure with hemangioma is common in visceral and multiple hemangiomas, but extremely rare in the case of scalp CHs. 9 The characteristic fast-flow nature of CHs and resulting shunting of blood lead to development of heart failure. 1 The size of hemangioma appears to be the main factor associated with development of heart failure because this complication has not been reported in the case of tumors <7 cm in diameter. 2 Furthermore, this tendency of CHs to cause heart failure requires further analysis. 10
Few studies have reported sporadic cases of scalp hemangiomas that showed symptoms of cardiac failure upon presentation4,7,11,12 (Table 1). Recently, Shah et al. 4 reported a case of a premature infant with right parietal hemangioma that caused high-output heart failure. Their patient underwent embolization using n-butyl cyanoacrylate glue and detachable coils, which reduced the size of the hemangioma and improved heart function. Another report described a premature infant, who presented with scalp hemangioma on fetal ultrasound and symptoms of high-output heart failure, and was treated with ligation of feeding arteries and surgical excision. 7 Moreover, Konez et al. 12 and Vaksmann et al. 11 reported cases with different outcomes. Konez et al. 12 reported a patient who was treated with embolization that significantly reduced the lesion size in 1 year and was free of the disease with only a tiny scar at the surgical site. However, Vaksmann et al. 11 reported a girl who was born full term with a hemodynamically stable condition and scalp hemangioma, and was treated with prednisolone. However, this patient experienced worsening cardiac function at 4 days of life and did not respond to medical treatment. She continued to deteriorate until she died at the age of 5 days. Wolfe et al. 13 reported a case of scalp hemangioma in a 2-month old infant who presented with Kasabach–Merritt syndrome. This patient was treated endovascularly by Onyx embolization, which reduced the lesion size and resolved thrombocytopenia.
Reported cases of infantile scalp hemangioma associated with cardiac failure.
Endovascular and open surgical approaches for treating infantile scalp hemangioma are well described in the literature. In patients with mild symptoms of this condition who are controlled by medical treatment, waiting is beneficial to allow body mass to increase and minimize the interventional risks. 14 Although endovascular embolization of feeding arteries is a safe and effective treatment strategy, the risk of recurrence significant. 1 Endovascular intervention for infantile scalp CH reduces intraoperative bleeding and the operation time and improves associated conditions, including heart failure and thrombocytopenia. However, adequate preparation for this condition is required for application in neonates to prevent complications. 4
Multidisciplinary decision-making is crucial in premature infants with poor cardiac function who cannot tolerate surgery. Endovascular embolization is considered as the first modality of treatment for CH because it has less risk than surgery, which is associated with a high bleeding rate and unstable cardiac function. The main aim of preoperative embolization is to obliterate the arterial feeders, decrease the blood supply, and minimize arteriovenous shunting at the lesion. This leads to a decrease in load on the heart and improvement in cardiac function. Analysis of angioarchitecture, hemodynamics of the lesion, and selection of embolic material and vascular access are crucial in the process of managing high-flow vascular lesions. 14
Neurointerventional treatment in premature infants requires experienced personnel and special preparation to address issues, including device and agent selection, contrast use, radiation exposure, and minimization of blood loss. Our patient experienced post-procedure spasms in the right external iliac artery, right common femoral artery, and proximal right superficial femoral artery, and this was managed conservatively. The patient’s cardiac function improved after embolization and was resolved after surgery. He was discharged after 1 week. Therefore, endovascular embolization is a safe and effective method for improving cardiac function, decreasing the size of the hemangioma, and facilitating surgical excision, and should be considered before surgery.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics statement
The authors’ institute does not require ethical approval for Case Reports. The patient’s parents provided informed consent for a video and photography, which were included in the surgical consent, and publication for the case report.