
Abstract
Objective
This study was performed to evaluate the association of preoperative anxiety with inflammatory indicators and postoperative complications in patients undergoing scheduled aortic valve replacement surgery.
Methods
A prospective cohort study was performed. The Hamilton Anxiety Scale was used to assess preoperative anxiety. The serum white blood cell (WBC) count and concentrations of C-reactive protein, interleukin (IL)-6, and IL-8 were measured 1 day preoperatively and 3 and 7 days postoperatively. Postoperative complications were also recorded.
Results
Seventy-three patients were included. The incidence of preoperative anxiety was 30.1% (22/73). The payment source was the only independent risk factor for preoperative anxiety. The incidence of postoperative complications was lowest in the mild anxiety group. The WBC count 3 days postoperatively was significantly lower in the mild than moderate-severe anxiety group. The IL-8 concentration 1 day preoperatively was highest in the no anxiety group.
Conclusions
Mild preoperative anxiety might help to improve clinical outcomes. However, further investigations with more patients are warranted. Patients with different degrees of anxiety may have different levels of inflammatory cytokines.
Keywords
Introduction
Although cardiac surgery usually improves patients’ prognoses, many of these patients experience preoperative anxiety. 1 Indeed, cardiac surgery via a sternotomy is a particularly invasive procedure associated with a high risk of perioperative complications that are sometimes life-threatening. Patients scheduled to undergo such a procedure must make difficult decisions when choosing surgical options that carry risks of severe postoperative complications and mortality. As shown in previous studies, anxiety is ubiquitous among patients undergoing cardiac operations.2,3 However, despite the remarkably improved surgical treatments for cardiac diseases in recent years, 4 few studies have focused on the psychological issues of patients undergoing cardiac surgeries. 5 Accordingly, a review has suggested that clinicians should pay more attention to the physical/mental stress of patients undergoing major cardiac operations. 6
The status of perioperative anxiety has been evaluated in several studies, including in patients undergoing coronary artery bypass grafting operations.7,8 These studies often included patients undergoing coronary artery bypass grafting and/or valve surgeries.9,10 Because the clinical symptoms, surgical procedures, and prognoses are different between patients with coronary disease and valvular disease, the role of perioperative anxiety in patients undergoing aortic valve replacement via a median sternotomy should be evaluated exclusively. Moreover, a recent systematic review demonstrated a potential association between anxiety and inflammatory dysregulation as reflected by increased proinflammatory markers. 11
Stress-induced immunoprotection or immunopathology may affect the levels of proinflammatory factors, thereby influencing the clinical outcomes of these patients.12,13 However, to our knowledge, few studies have focused on this issue in patients undergoing cardiac surgery. The relationship between the symptom severity of anxiety and inflammatory markers has also been rarely studied. 11 Some interventions, such as music therapy or massage therapy, might alleviate patients’ excessive anxiety as evidenced by previous studies.14,15 However, anxiety is a complex psychological reaction influenced by various factors related to the personal experiences of the individual patient, including culturally specific sociodemographic factors. 16 Because the factors that induce anxiety may be unique in individual patients undergoing valve surgeries, clarification of the associated risk factors for preoperative anxiety may be useful for the development of potential targets of interventions before these patients’ operations, compared with general preventative measures such as music therapy or massage therapy. 17
The current study was performed to evaluate anxiety and related risk factors in a cohort of patients undergoing scheduled aortic valve replacement via a median sternotomy in China and to observe the association of preoperative anxiety with postoperative complications and perioperative inflammatory indicators in these patients.
Materials and methods
This was a prospective cohort study. This study was approved by the Research Ethics Committee of Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences (approval No. 20190404), and all included participants were aware of this study and provided written consent. The study was conducted in accordance with the Declaration of Helsinki.
Patients
From November 2016 to November 2019, consecutive patients with aortic valve disease who were scheduled to undergo aortic valve replacement for the first time and who provided written consent to participate in this observational study were prospectively enrolled.
Patients were excluded if they (1) had a history of psychopathy, (2) had acute inflammation at the time of admission, (3) were taking drugs such as bronchodilators or β-adrenergic receptor agonists with known side effects of anxiety, (4) underwent an emergency operation, (5) did not quit smoking before surgery, or (6) had a language barrier that prevented them from communicating sufficiently.
Psychological measurements
The Hamilton Anxiety Scale (HAM-A), a proven and valid questionnaire to assess anxiety in patients undergoing cardiac surgeries18,19 and in Chinese populations, 20 was used to measure the anxiety level of the eligible patients. The HAM-A comprises 21 items. Each item is scored on a 5-point scale (0 = not present to 4 = very severe). In this study, the patients’ anxiety levels were defined according to the overall scores as follows: 20 0 to 6 = no anxiety, 7 to 13 = mild anxiety, 14 to 20 = moderate anxiety, and ≥21 = severe anxiety.
Two trained investigators performed the psychological assessments 1 or 2 days before the operation. The investigators were trained by specific psychologists before the HAM-A evaluation was performed. Additionally, both investigators were blinded to the study design. All eligible patients were grouped according to their anxiety levels into the no anxiety group, mild anxiety group, moderate anxiety group, and severe anxiety group.
Data collection
Following enrollment, the patients’ baseline characteristics were recorded by a data collector. Serum inflammatory factors including the white blood cell (WBC) count, C-reactive protein (CRP) concentration, interleukin (IL)-6 concentration, and IL-8 concentration were measured 1 day preoperatively and 3 and 7 days postoperatively with immunofixed time nephelometry (Dade Behring Diagnostics, Deerfield, IL, USA) in the clinical blood laboratory of our hospital. The incidences of postoperative complications, including low cardiac output syndrome, organ failure, severe infection, pulmonary disorder, and postoperative death, were recorded until discharge.
We used the following measures to minimize potential biases of the study: (1) the designers of the study were not permitted to take part in data collection, (2) the data collector was not allowed to take charge of data analysis and did not know the research protocol, (3) the data collector ensured that all eligible patients fully understood every item of the HAM-A and that the survey was conducted in a quiet room without any disturbance, and (4) the statistician analyzed the data independently without any disturbance.
Statistical analysis
For normally distributed continuous variables with homogeneity of variance, comparisons among multiple groups were conducted by one-way analysis of variance. Continuous variables with a skewed distribution were transformed into scaled data, and the Kruskal–Wallis H test was carried out among the groups. The presence of a normal distribution was assessed via the Kolmogorov–Smirnov test (P > 0.05). The presence of homogeneity of variance was assessed using Levene’s test (P > 0.05). The chi-squared test was applied for categorical data. Binary logistic regression was carried out to identify risk factors for anxiety, and Spearman’s rank correlation was used to assess the correlation between the level of anxiety and risk factors. A P value of ≤0.05 indicated statistical significance. The data analysis was carried out with IBM SPSS Statistics for Windows, Version ≥22.0 (IBM Corp., Armonk, NY, USA).
Results
Preoperative anxiety and related risk factors in patients undergoing aortic valve replacement via median sternotomy
In total, 132 patients were initially screened, and 73 eligible patients were finally enrolled in the study (Figure 1). Among these 73 patients, 51 had no anxiety, 14 had mild anxiety, and 8 had moderate-severe anxiety (7 had moderate anxiety and 1 had severe anxiety). The patients’ baseline clinical and sociodemographic variables according to the severity of their preoperative anxiety are presented in Table 1. Six variables (relationship with friends/relatives, degree of satisfaction in communication with doctors, blood type, alcohol consumption, quit smoking recently, and payment source) showed statistically significant differences among patients of different groups.

Flow chart of participant enrollment.
Baseline clinical and sociodemographic characteristics of patients with different severities of preoperative anxiety (n = 73).

Data are presented as mean ± standard deviation or n (%).
Further comparisons between any two groups were carried out.
Normal distribution (P = 0.200) and homogeneity of variance (P = 0.991).
Non-normal distribution (P = 0.002); thus, the continuous data were transformed into scaled data.
One patient was unsatisfied with the communication. He cancelled the operation and transferred to another hospital.
Quit smoking within 1 month.
Further pairwise comparisons were then conducted (Table 2). We conducted binary logistic regression to clarify the independent risk factors for preoperative anxiety. We found that the payment source was the only independent risk factor for anxiety (Table 3).
Pairwise comparisons of baseline variables with statistically significant differences among patients with different severities of preoperative anxiety.

Binary logistic regression analysis for the risk factors of preoperative anxiety.
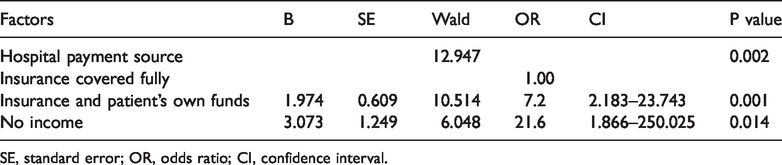
SE, standard error; OR, odds ratio; CI, confidence interval.
Association of preoperative anxiety with postoperative complications and inflammatory indicators in patients undergoing aortic valve replacement via median sternotomy
The incidences of postoperative complications, the IL-8 concentration 1 day preoperatively, and the WBC count and CRP concentration on the third day postoperatively were significantly different among the three groups (Table 4). Further pairwise comparisons of the four variables were then conducted. The incidence of postoperative complications was lowest in the mild anxiety group (mild anxiety group versus no anxiety group, adjusted P value (P') = 0.015; mild anxiety group versus moderate-severe anxiety group, P' = 0.020). The WBC count 3 days postoperatively was lower in the mild anxiety group than moderate-severe anxiety group (P' = 0.015). The IL-8 concentration 1 day preoperatively was highest in the no anxiety group (mild anxiety group versus no anxiety group, P' = 0.013; no anxiety group versus moderate-severe anxiety group, P' = 0.007). The remaining pairwise comparisons showed no statistically significant differences (Table 5).
Incidence of postoperative complications and levels of inflammatory cytokines among patients with different severities of preoperative anxiety (n = 73).

Data are presented as n (%) or median (interquartile range).
Further comparisons between any two groups were carried out.
Non-normal distribution (P = 0.001); thus, the continuous data were transformed into scaled data.
BO, before operation; AO, after operation; WBC, white blood cell; CRP, C-reactive protein; IL, interleukin.
Pairwise comparisons of incidences of postoperative complications and inflammatory cytokines with statistically significant differences among patients with different severities of preoperative anxiety.

WBC, white blood cell; CRP, C-reactive protein; IL-8, interleukin 8
Statistically significant
Discussion
In this pilot prospective cohort study, we found that preoperative anxiety was common in patients who underwent aortic valve replacement via a median sternotomy. The patients with moderate to severe anxiety accounted for 30.1% of the enrolled patients, which is similar to the proportion in a previous report. 9 Interestingly, we found that the incidences of postoperative complications were significantly lower in patients with mild anxiety than in those without anxiety or with moderate to severe anxiety. This is different from previous findings, which showed that patients’ prognosis worsens as the severity of anxiety increases in a dose–response manner. 21 Our study suggests that mild anxiety may be protective. Anxiety is induced by unpleasant stimuli. It is characterized by somatic, emotional, cognitive, and behavioral components and often creates worry, fatigue, fear, dread, uneasiness, and muscle tension. 22 In 2013, Grupe and Nitschke 23 stated that mild anxiety may promote adaptive activities to deal with jeopardizing stimuli. Furthermore, they stated that positive adaptive activities result in improved outcomes whereas excessive anxiety results in negative activities and mental conditions, which are correlated with negative clinical effects. 23 This is consistent with our results.
According to our current understanding, mental suffering associated with open heart surgery should be considered a comprehensive injury caused by both physical damage and psychological stress to the patients. Moreover, it can also worsen patients’ socioeconomic status. Indeed, the financial burden of treatments can be tremendous because patients must stop their current work for prolonged periods, which further decreases their household income and increases their economic burden. Indeed, the decline in socioeconomic conditions further exacerbates patients’ psychological status. 24
In this study, the payment source was identified as the only independent risk factor for preoperative anxiety. Insurance coverage was considered a prophylactic factor for reducing patients’ anxiety level. Lower insurance coverage required more out-of-pocket expenditures. This resulted in a reduced household income (as discussed above), which is a risk factor for exacerbation of anxiety disorders. 25
This study was performed in a hospital in China. Although most patients’ expenses were covered by medical insurance, a significant proportion of patients with low annual incomes could not afford the uninsured portion of the medical expenses. This financial burden might have induced anxiety in these patients. In 2019, Su et al. 26 proposed that an income-matching payment system might contribute to resolving this issue. In our study, patients in the mild anxiety group were the largest proportion of patients receiving copayments (and therefore paying medical bills with both insurance and their own funds). The potential association among copayment, mild anxiety, and a lower incidence of postoperative complications may be related to better compliance in these patients. Those without insurance coverage or who had low income were more likely to be non-compliant with treatments. 27 Although full insurance coverage can reduce a patient’s anxiety level, overtreatment may compromise treatment outcomes. 28 In contrast, copayment might enhance patients’ compliance and their decision-making process during treatment.29,30 These plausible reasons contribute to better clinical outcomes in patients receiving copayments.
The degree of satisfaction in communicating with doctors in this study reflected whether the treatment information supplied by the doctors to the patients was sufficient and satisfactory. Our results showed that good communication with doctors greatly reduced moderate-severe anxiety in patients. These results are in accordance with the conclusions proposed by Lassen et al. 31 Extensive preoperative counseling can also alleviate mental trauma. The potential risks of operations and specific expected tasks for patients should be clearly explained because most patients undergoing open heart surgery are undergoing this procedure for the first time.
In a previous study, Mishra et al. 32 audiotaped preoperative consultations with patients and freely gave the patients access to these recordings, increasing the patients’ acquisition of treatment knowledge and subsequently reducing their anxiety. However, a recent review of randomized controlled trials evaluating the effects of preoperative education on anxiety and clinical outcomes showed inconsistent results among the included studies. 33 A study by Deyirmenjian et al. 34 demonstrated that appropriate preoperative education and counseling should be offered based on each patient’s cultural background, language, and religious preferences. This suggests that complex interactions exist between communication content and anxiety, which warrants further investigation.
An association between ABO blood types and personality traits was proposed based on a large population investigation in Japan. 35 Interestingly, in the present study, we found that blood type A predominated among patients with moderate-severe anxiety, whereas blood type O was more prevalent among patients with mild anxiety. Most patients in the no anxiety group had blood type B. However, the relevance of blood types to personality traits is controversial, 36 necessitating further large-scale studies in the future.
Recent studies have demonstrated that inflammatory cytokines might be involved in the mechanisms mediating the pathophysiological effect of anxiety distress.37,38 We measured several serum indicators, including the WBC count and concentrations of CRP, IL-6, and IL-8, before the operations to investigate their variations in patients with different anxiety levels. The IL-8 concentration on the first day before the operation in the no anxiety group was the highest among all three groups. Janelidze et al. 39 also reported that the IL-8 concentration in both plasma and cerebrospinal fluid were negatively correlated with the severity of patients’ anxiety symptoms, which might explain the lower IL-8 production contributing to pathophysiological changes that mediate anxiety symptoms. 37 However, because the exact molecular mechanisms involved were not revealed, further investigations should be carried out.
The study has some limitations. This was a pilot study focusing on the anxiety status of patients scheduled for aortic valve replacement. We enrolled only 73 patients because of the strict inclusion and exclusion criteria that were applied to avoid potential selective bias. The conclusions of this study should be further validated in future studies with large sample sizes. The postoperative anxiety level might be correlated with the preoperative anxiety status. It might also be involved in the patients’ recovery process. However, postoperative anxiety was not measured in the present study.
In conclusion, the payment source is the independent determinant of preoperative anxiety in patients undergoing scheduled aortic valve replacement via a median sternotomy in China. Mild preoperative anxiety seemed to be beneficial for clinical outcomes with complicated reasons related to local socioeconomic and medical factors. Patients with different degrees of anxiety may have different levels of inflammatory cytokines.
Footnotes
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the National Key Research and Development Program [2018YFC1002600]; the Science and Technology Planning Project of Guangdong Province, China [No. 2017A070701013 and 2017B090904034, 2017030314109, 2019B020230003]; and the Guangdong Peak Project [DFJH201802]. The authors declare that the funding bodies were not involved in the study design; the data collection, analysis, or interpretation; or the writing of the manuscript.
Author contributions
QG and JZ conceived and designed the research; HPM, HYZ, HLQ, JZC, JMC, and JL collected the data and conducted the research; JZC, JMC, ZRC, YT, and XHL analyzed and interpreted the data; QG and HPM wrote the initial paper; JZ revised the paper; and JZ had primary responsibility for the final content. All authors read and approved the final manuscript.