
Abstract
A 59-year-old patient underwent the duodenal endoscopic mucosal resection of a hyperplastic polyp. Four hours after the procedure she developed severe epigastric pain. Laboratory and imaging results were consistent with mild acute edematous pancreatitis. After several days of dietary therapy and intravenous crystalloid fluids the patient recovered, and 1 month later was asymptomatic and had no signs of pancreatic inflammation. This case illustrates a rare but clinically important complication of therapeutic upper endoscopy, which may be attributable to thermal injury of the duodenal wall and the adjacent pancreas. It also underscores the importance of the close follow up of patients who undergo invasive endoscopic procedures and the need for additional preventive measures to be taken when resecting duodenal lesions.
Introduction
Duodenal polyps are much more rarely encountered than colorectal polyps during endoscopy, 1 and they are typically incidental findings. 2 Whereas duodenal polyps may be endoscopically removed to reduce the risk of subsequent cancer, most do not require treatment because they are benign. 3 However, there are no current guidelines that provide appropriate diagnostic and treatment algorithms. Duodenal endoscopic mucosal resection (EMR) is an invasive procedure that is associated with certain complications, even in experienced hands, but pancreatitis is a rare complication. Here, we report a case in which mild acute pancreatitis developed after the endoscopic mucosal resection of a hyperplastic duodenal polyp.
Case report
The Ethics committee of the University Hospital, Varna, Bulgaria, approved the publication of the present case report. The patient gave her written informed consent at admission for all the required procedures. The details of the case have been de-identified in order to protect patient anonymity.
A 59-year-old female patient with a hyperplastic sessile duodenal polyp of approximately 12 to 13 mm in diameter (grade 0-Is, according to the Paris classification) was referred to our clinic for elective polypectomy. Ultrasonographic examination of her abdomen showed no biliary or pancreatic abnormalities. Before performing the procedure, upper endoscopy was performed using both forward- and side-viewing endoscopes. This revealed that the lesion was located in the proximal portion of the duodenum, distant from the major papilla, which appeared normal. After saline infiltration, during which a good lifting sign was observed, the polyp was removed in two pieces (Figures 1 and 2). The first piece was excised using a spiral snare, initially using several bursts of forced coagulation (45 W), followed by the use of ENDO CUT slow-cut mode (45 W; Olympus ESG-100, Hamburg, Germany). The remaining piece was removed using a monofilament snare and ENDO CUT slow-cut mode (45 W). No intra- or post-procedural hemorrhage was observed. Four hours after the polypectomy, the patient developed severe epigastric pain and upper abdominal tenderness. Plain abdominal X-ray imaging excluded perforation. Contrast-enhanced computerized tomography (CT) revealed diffuse swelling of the pancreas, with moderate fluid collection around the head, body, and tail, between the duodenum and Gerota’s fascia (Figure 3). The laboratory results were as follows: amylase activity, 2669 U/L (upper limit of normal 118 U/l); lipase activity, 7124 U/l (upper limit of normal 67 U/L); and C-reactive protein, 118 mg/L. The remaining laboratory test results were unremarkable. There were no signs of other organ involvement; therefore, a diagnosis of mild edematous pancreatitis was made. The patient recovered after several days of treatment using diet and intravenous crystalloid fluids, and there were no signs of further complications on a second CT examination. One month after the procedure the patient remained asymptomatic and there was no evidence of abdominal fluid on ultrasonographic examination.
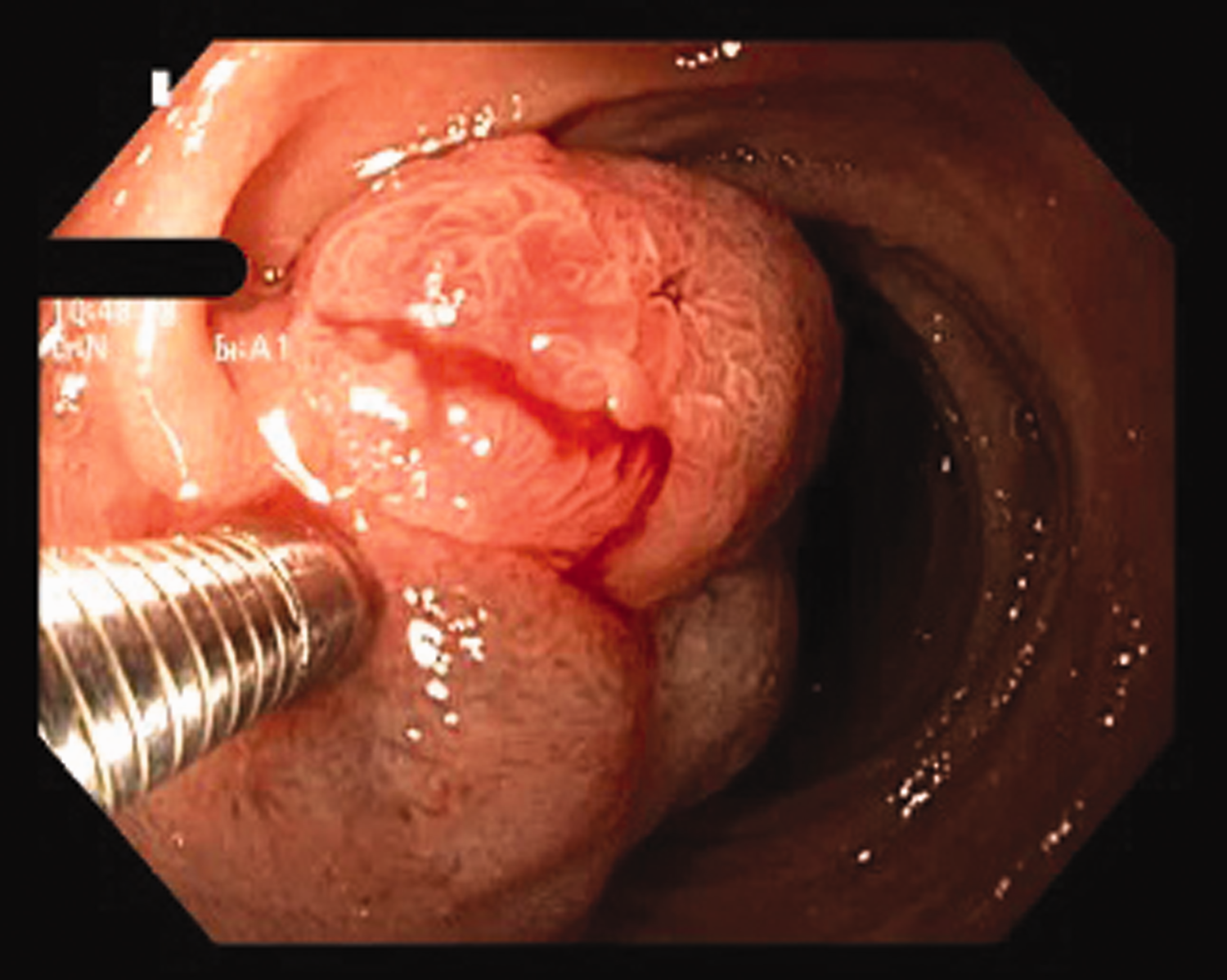
Endoscopic image of the duodenal polyp after saline infiltration, showing good lifting sign. Equipment used: Olympus Exera II H180 gastroscope, without magnification.

Endoscopic image of the same polyp after partial resection. Minimal bleeding is present after the initial excision, which stopped after the complete removal of the lesion. Equipment used: Olympus Exera II H180 gastroscope, without magnification.
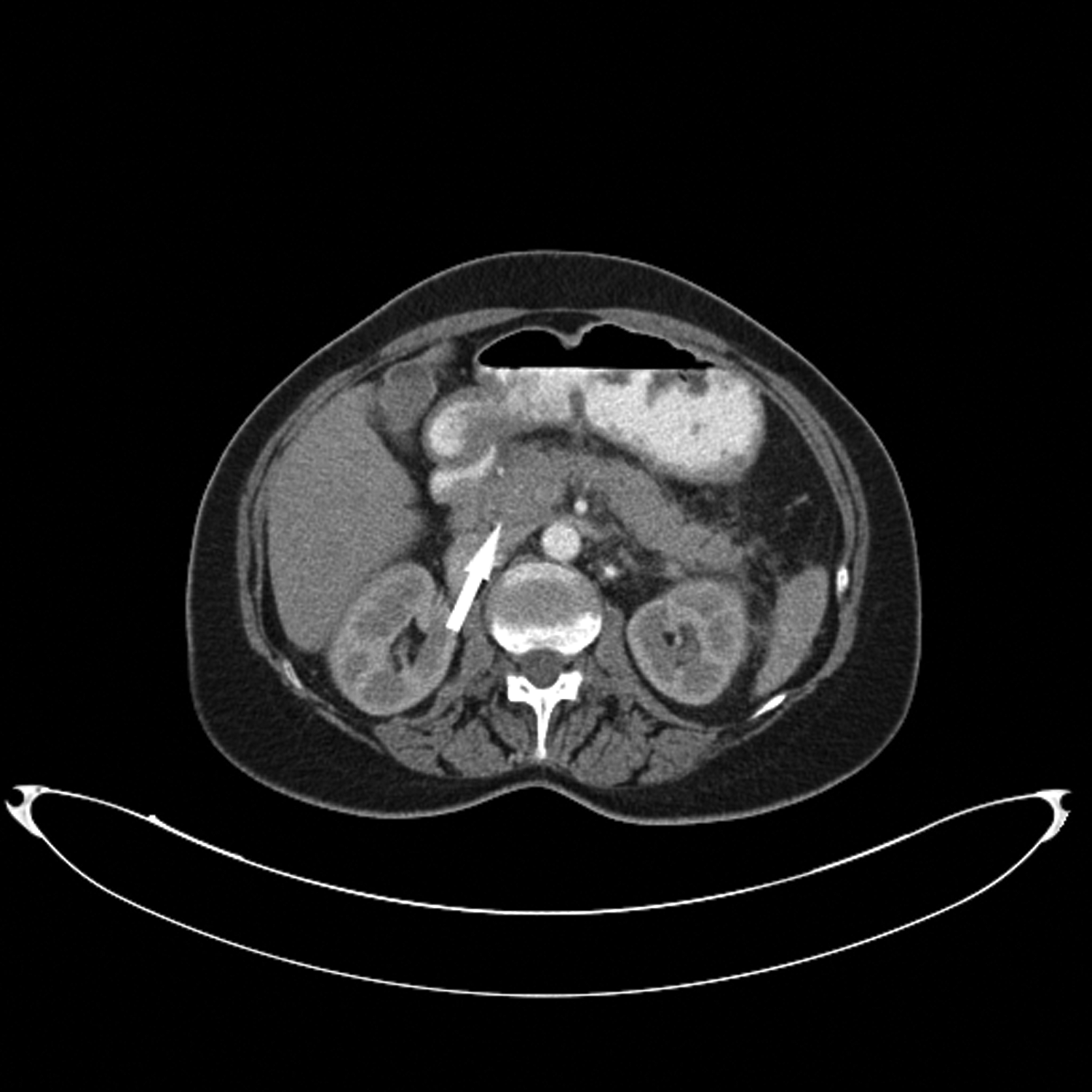
Abdominal contrast-enhanced computed tomography image, revealing swelling of the pancreatic head (arrow).
Discussion
Duodenal polyps are diagnosed in approximately 1.5% to 3% of patients that are referred for upper endoscopy, and can be classified as non-neoplastic or neoplastic. The former can be subdivided into hyperplastic polyps, hamartomas, or cysts of Brunner’s glands, gastric or pancreatic heterotopia, and hyperplastic, inflammatory, or hamartomatous polyps; and the latter into intestinal or gastric-type adenomas, serrated adenomas, and neuroendocrine tumors. 4 The natural history of duodenal polyps is poorly understood, and therefore removal is indicated when they are large or symptomatic, or when histological examination reveals the presence of dysplasia or cancer. 5 Endoscopic polypectomy, the mainstay of the treatment of these lesions, achieves complete resection in most cases. However, complications, such as bleeding and perforation, have been reported, with incidences varying between 4.5% and 13.9%. 5
In the present case, previously performed histology showed that the polyp was benign, but because the patient was symptomatic and afraid of its progression to cancer, elective resection was planned after all of the possible consequences of the procedure had been explained. However, the development of pancreatitis was not anticipated because of the size and the histological features of the lesion. To our knowledge, only a few cases of post-procedural acute pancreatitis have been reported to date. The first two cases of mild acute pancreatitis after the removal of two 1-cm duodenal adenomas by snare polypectomy, without pre-procedural saline infiltration, were described in 1975. 6 Subsequently, Kwak et al. reported a 5-mm dysplastic polyp of the duodenum in a 60-year-old male patient that was removed by snare polypectomy after adrenaline infiltration. As in the present case, acute pancreatitis was diagnosed 4 hours after the procedure, but the patient’s condition further deteriorated, and he died 62 days later because of multi-organ failure. 7 Weigt et al. identified mild pancreatitis in a 43-year-old female patient with familial adenomatous polyposis who had undergone treatment of multiple duodenal polyps, and the patient recovered quickly after the procedure. 8 Finally, a 17-year-old boy with Hodgkin’s lymphoma who underwent duodenal biopsy because of epigastric pain experienced complications of intramural duodenal hematoma and lethal necrotizing pancreatitis. 9 Thus, pancreatitis can be a complication of duodenal postpolypectomy, simple duodenal biopsy, or the more traumatic snare polypectomy.
The established technique for polyp removal is snare polypectomy. Electrocautery, generated from an electrosurgical unit and transmitted to the metal ring of the snare, can be used to incise tissue through cellular rupture, or coagulate through cell shrinkage. 10 However, sometimes, the applied electric current can extend into the duodenal muscularis propria, and even the serosa, resulting in a transmural burn, without perforation. 11 The closeness of the pancreatic body to the duodenal wall and the extension of the diathermy from the polypectomy site to the adjacent pancreatic tissue is the most probable cause of the complication that developed in the present case. The transmitted heat could destroy acinar cells and trigger the activation of trypsin. There are several possible ways to prevent extensive thermal injury of the duodenal wall. One of these is the use of saline infiltration prior to the procedure, which was performed in the present patient, but was probably insufficient. Therefore, the use of a monofilament snare and the ENDO CUT mode alone, with short coagulation periods, may be more appropriate. Alternatively, a single en-bloc resection of the lesion would avoid the exposure of the intestinal wall to the damaging effects of the diathermy. However, polyps can slip when caught loosely with the snare and subsequent removal of the remnant may be required to prevent recurrence. Another effective preventive measure is underwater EMR, which has been proven to be feasible without injection, and to be safe because thermal injury to the duodenal wall is minimized by the shallowness of the incision and the small defect created. 12 This was not performed in the present patient. Injection of saline into the deep intestinal wall layers, and potentially also the pancreas, could also explain the complication that developed in the present patient because such injury to the pancreatic tissue might also induce enzymatic activation. A final possible explanation is that the polypectomy included an unrecognized ampulla (ampullectomy), causing an obstruction of the pancreatic duct due to swelling of the orifice. However, duodenoscopy showed that the polyp was proximal to the papilla, and the lesion showed a good lifting sign during saline infiltration.
In conclusion, acute pancreatitis after duodenal EMR is a rare, but severe and sometimes life-threatening condition. In the colon, small lesions can typically be removed without complication, but the proximity of the pancreas should be borne in mind when removing duodenal polyps, and additional measures should be taken to minimize the risk of deep thermal injury to the intestinal wall. These measures may include saline infiltration, single complete en-bloc excision, or underwater EMR.
Ethics statement
The publication of this manuscript was approved by the Local Ethics Committee of University Hospital “St. Marina”, Varna, Bulgaria. The patient gave their written informed consent at admission for all the procedures performed.
Footnotes
Author contributions
Conceptualization: M.M.; writing, original draft preparation: M.M., J.C.H.; writing, review and editing: M.M., J.C.H., S.A., D.G., A.K., N.G. All authors read and agreed the published version of the manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.