
Abstract
Vaginal cancer is a rare disease of the lower genital tract. We present the case of a 54-year-old woman with occult vaginal cancer after hysterectomy for cervical intraepithelial neoplasia (CIN) III. Despite persistently negative cytology and colposcopy results, a lesion was finally detected by vagino-recto-abdominal examination and she underwent radical parametrectomy and lymph node dissection. We consider the possibility that transabdominal suturing of the vaginal cuff after hysterectomy may reduce the ability to detect subsequent vaginal lesions, and discuss the benefits of a vaginal suture approach. We recommend that suturing the vagina apex transvaginally instead of transabdominally would benefit patients during follow-up.
Keywords
Introduction
Vaginal intraepithelial neoplasia (VaIN) and vaginal cancer are rare diseases of the lower genital tract. 1 There is a high risk of VaIN after hysterectomy in patients with a history of cervical precancer or cancer. These hysterectomy patients may thus benefit from a vaginal suture approach following hysterectomy to improve the visibility of the vagina during colposcopy, as well as high-risk (hr) human papillomavirus (HPV) and cytology tests during follow-up. Here we present a patient with occult vaginal cancer finally detected by physical examination, despite negative cytology and colposcopy results.
Case presentation
A 54-year-old woman underwent minimally invasive hysterectomy at her local hospital 5 years earlier because of cervical intraepithelial neoplasia (CIN) III. During follow-up, her cytology results were negative but hrHPV was continually positive. VaIN II–III was detected by vaginal biopsies at the local hospital in 2017. The patient was treated with interferon for 1 year, followed by repeat cervical screening. The cytology results were still negative but hrHPV was still positive, and the patient was therefore referred to the colposcopy department of the Obstetrics and Gynecology Hospital of Fudan University for further treatment. The patient received colposcopy by an experienced colposcopist in our department in March 2018. The colposcopy results appeared normal and the vaginal biopsy showed vaginal epithelium. However, because of her former history of CIN III, the patient was advised to visit a gynecologist every 3 months. The results of repeat liquid-based cytology and hrHPV tests 3 months later were again cytology negative and hrHPV positive. The patient therefore underwent repeat colposcopy by the same colposcopist in January 2019. The colposcopy appearance was normal; however, there were scattered plaques at the front vaginal wall, presenting as thin acetowhite epithelium and nonstained with Lugol’s solution (Figure 1a, b). The colposcopist therefore recommended repeat colposcopy 1.5 months later, which was accordingly carried out by the same colposcopist in March 2019. We still detected normal squamous epithelium, but with slight bleeding at the right dimple (Figure 1c, d). The biopsy was normal, but given the patient’s consistently positive hrHPV and negative cytology and histopathology follow-up results, the colposcopist performed an additional vagino-recto-abdominal examination, though a previous vagino-abdominal examination carried out when the patient was first referred had revealed no abnormality. The colposcopist detected a 3- × 1.5-cm mass at the right corner, and magnetic resonance imaging (MRI) confirmed a 2.3- × 2.3-cm mass (Figure 2a). These findings indicated recurrent VaIN II or a more severe lesion (all pathologies were reaffirmed). The patient also received HPV genotyping, which identified hrHPV 16. The patient underwent radical parametrectomy and lymph node dissection. The histopathological results showed invasive squamous vaginal cancer (IIB) (Figure 2b, c). The patient was discharged uneventfully 2 weeks after surgery and received subsequent radiotherapy. No abnormalities were detected after 1 year of follow-up.

Colposcopy presentations of occult vaginal cancer. (a, b) Scattered plaques were found in January 2019; (c, d) images in March 2019. (a, c) Acetic acid staining; (b, d) Lugol’s staining.
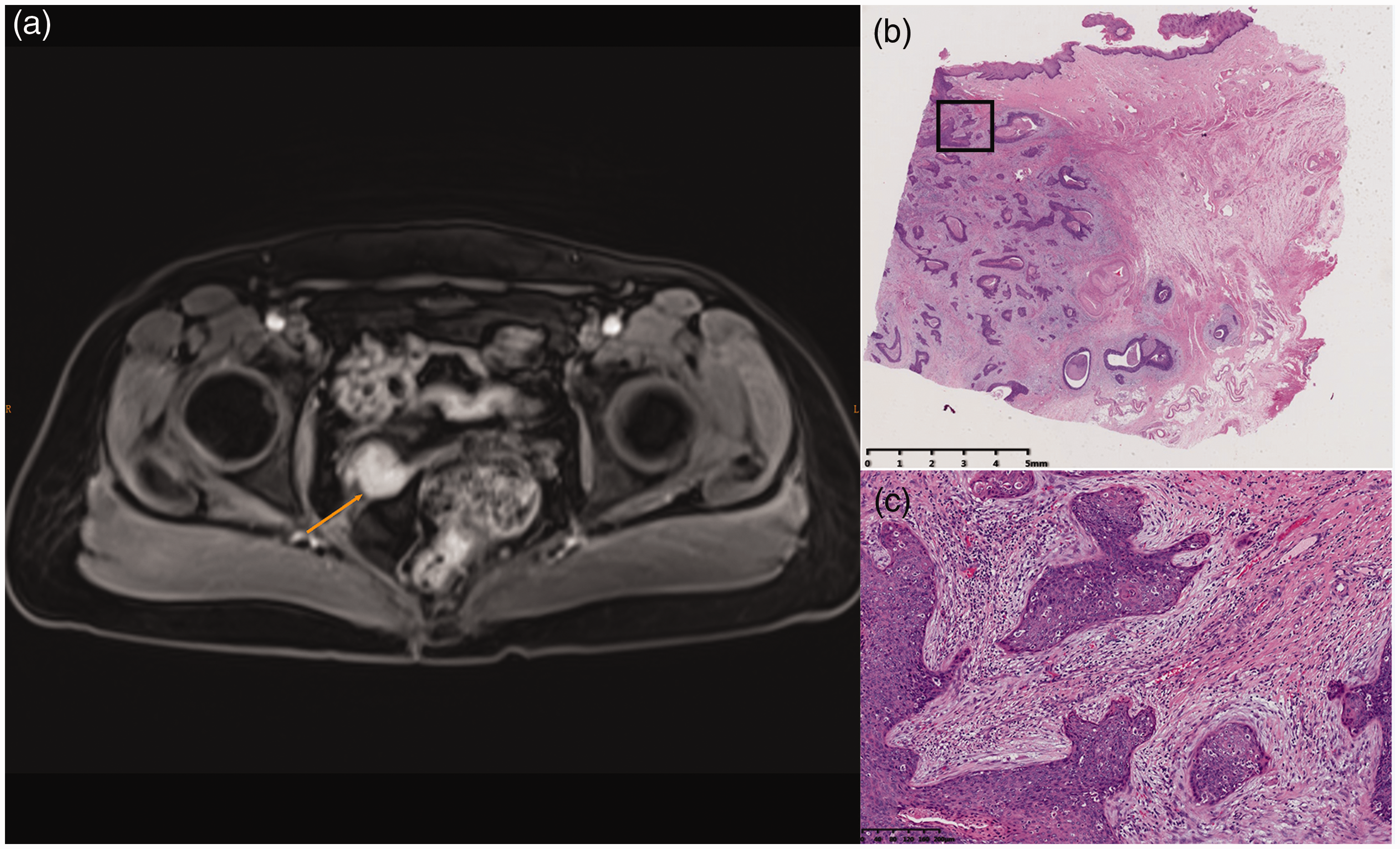
Enhanced magnetic resonance image and pathology of vaginal cancer. (a) An enhanced mass measuring 2.3 × 2.3 cm was detected at the right vagina apex (arrow). (b) Pathology indicated invasive squamous vaginal cancer; (c) magnified view of boxed area in (b). (b, c) Hematoxylin–eosin staining.
The patient gave her informed consent for publication of this case report.
Discussion
According to the literature, the morbidity of vaginal cancer is 0.4 to 0.6/100,000 women, while that of VaIN is 0.2 to 0.3/100,000 women. The average detection rate of VaIN among patients with all lower genital tract intraepithelial lesions in our hospital was 11% (1923/16,732), exposing an increasing trend from 2013 to 2015. VaIN appears to be rarer than vaginal invasive cancer because it is frequently underdiagnosed. In addition, there is currently limited evidence to support the development of guidelines recommending screening for post-hysterectomy patients with cervical precursors, and current screening management is related to patients undergoing loop electrosurgical excision procedure. Cytology and hrHPV tests plus careful colposcopic examination of the entire lower genital tract are therefore essential for diagnosing vaginal and vulvar lesions in women who have undergone hysterectomy for CIN or cervical cancer. 2
Notably, the vaginal cancer in the current patient was an occult invasive squamous cell carcinoma. The right dimple was difficult to inspect fully and the biopsy results were negative. This may be because the surgeon who carried out the minimally invasive hysterectomy sutured the vaginal cuff transabdominally. After cutting the uterus, surgeons usually suture the vaginal cuff from the abdominal view, and tie the two ends of the vaginal apex to the cardinal ligaments to form two dimples. However, the area between the suture opening and cutting edge are then invisible. In addition, there is no standard distance from the suture opening to the cutting edge, and it is therefore difficult to inspect and biopsy the whole vagina during colposcopy at follow-up, because part of the vagina is not visible. In contrast, suturing by the vaginal route may be preferable. 3 To compare the benefits of these suture approaches, we searched PubMed for published papers using the terms “hysterectomy” and “VaIN”. We identified 69 papers, of which only two discussed the suture approach: one suggested that a vaginal approach reduced the risk of lesions because it would be easier to assess the vagina fully, both during the operation and at follow-up, while the other study found no difference between the suture techniques.4,5 Based on our experience, we recommend minimally invasive or abdominal hysterectomy with vaginal suture on the vaginal cuff opening for cervical lesions. However, more studies are needed to confirm this.
The current patient was previously diagnosed with VaIN II–III, which might have been attributed to the biopsy. Although biopsy represents a method of both diagnosis and treatment, it is also associated with the risk of the lesion spreading to the dimple as occult disease after biopsy. Vaginohysteroscopy may be a suitable method for diagnosing such vaginal lesions. 6 However, there is currently a lack of research focusing on the role of vaginohysteroscopy in patients with cervical disease during follow-up.
Vagino-recto-abdominal examination is currently highlighted as the most valuable single noninvasive diagnostic method for assessing women with suspected endometriosis. 7 However, clinicians should also remain aware of the significance of careful physical examination in patients with cervical disease. In the current case, it was difficult to detect the invisible vaginal cancer, and physical examination played a key role in its diagnosis.
In 2011, Zhao et al. published an article on the follow-up outcomes of a large cohort of US women with negative cytology and positive hrHPV tests. Among 869 women identified at the 4-year follow-up, 290 had colposcopic examination and biopsies, and 211 were detected with CIN1 and low-grade squamous intraepithelial lesions or more severe lesions (24.3%). 8 hrHPV positivity, especially HPV 16 and 18, is thus an independent risk factor for CIN, and requires further management. 9 Patients with persistent hrHPV should be followed-up with colposcopy. The HPV type in the current patient was finally shown to be hrHPV 16.
In addition, vaginal cancer is usually diagnosed by physical examination and pelvic biopsy. However, MRI provides excellent spatial and contrast resolution, 10 and thus helps to diagnose the disease and determine the tumor stage. It may therefore be necessary to carry out a thorough examination plus imaging.
In conclusion, suturing transvaginally instead of transabdominally after hysterectomy may lower the risk of vaginal cancer. Vaginohysteroscopy, vagino-recto-abdominal examination, and MRI may all be effective methods for detecting occult vaginal cancer.
Footnotes
Acknowledgement
The authors thank the patient for her kind cooperation during the treatment and follow-up.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by funding from the Research and Innovation Project of Shanghai Municipal Education Commission [No. 2019-01-07-00-07-E00050] and the Shanghai Science and Technology Natural Science Foundation [No. 19ZR1406900].